
Wheat: In Search of Scientific Objectivity and New Year’s Resolutions
Wheat: In Search of Scientific Objectivity and New Year’s Resolutions

Well it's that time again, so Happy New Year!
January is a great time for trying new things to improve our lives and make them a bit better than they were the year before. A number of people in the blogosphere have offered some great dietary ideas for January. Stephan Guyenet recently passed on Matt Lentzner's call for a Gluten-Free January. If you're up for a challenge, and a potentially bigger bang for a bigger buck, take on John Durant's 2011 Paleo Challenge and go “Paleo” for January.
As Melissa McEwen recently pointed out in her post about the 2011 Paleo Challenge, “Choosing plant foods because of their history without taking biochemistry into account is dogma, not science.”
She was referring to the disproportionate demonization of white potatoes, but I'd like to take this opportunity to poke a few holes in the disproportionate demonization of wheat of all foods, while nevertheless supporting the concept of the January gluten-free and Paleo challenges.
In particular, I'd like to provide a critical review of a study widely cited to show that wheat causes intestinal inflammation in people who do not have celiac disease, which in fact did nothing of the sort.
Since there are no validated tests for non-celiac gluten sensitivity (yes, I'm very prepared to defend this statement), going gluten-free for a while and reintroducing gluten is the best way to see whether you're sensitive. If you feel a lot better while gluten-free, but regress to how you felt before when you reintroduce gluten, it's pretty reasonable to conclude your are likely to be gluten-sensitive.
The main caveat to this approach is that most gluten products on the market are processed in ways that make them more toxic instead of less toxic, so getting rid of these nasty products doesn't necessarily indicate a problem with gluten per se.
Another caveat is that gluten is among the most difficult proteins to digest, so anyone with digestive problems caused by something else is likely to have problems with gluten, and it may be the case that such a person could tolerate gluten at a later time.
Nevertheless, better to get rid of the nasty stuff now and sort out the details later.
I went gluten-free, casein-free (GFCF) for a year and a half. My health got worse during that period. In particular, I developed my first panic attack in years, and I experienced periodic jitters that seemed like they might be related to blood sugar or cortisol problems.
I don't think I have enough evidence to definitively attribute these problems to the GFCF diet, and I was never able to separate the effects of going gluten-free from the effects of going casein-free, but I've been eating properly prepared gluten- and casein-containing foods again for years now and I no longer have these problems. So I think I am justified in concluding that going GFCF is not essential and probably isn't even beneficial to my health.
Nevertheless, many other people report benefits from going gluten-free, and whether you're sensitive is a question you are much more equipped to answer than your doctor is, so if you haven't done it already, I'd recommend going gluten-free. And while you're at it, might as well throw in a stab at a stricter Paleo diet as well.
While we're all being open-minded and non-dogmatic about this, I'd like to offer a brief critical review about a study that has been widely cited as showing that gluten causes intestinal inflammation in non-celiacs (1), when in fact it did nothing of the sort.
In this study, the researchers took intestinal biopsies from six individuals without celiac and then cultured them in laboratory dishes, and showed that adding wheat gluten or several difficult-to-digest fragments of the protein increased the production of interleukin-15 (IL15), an inflammatory signal. All of the non-celiac subjects were sick with problems like hiatal hernia and chronic gastritis.
If we're going to use this study to hate on wheat, we should start hating on coconut oil, because that ol' “one meal of saturated fat will practically kill you” study (2) was of much higher quality than this one. At least in that study they actually fed people coconut oil. Nevertheless, their interpretation of the study was enormously flawed, and I published an extensive critique on my web site and published a much shorter letter in the Journal of the American College of Cardiology criticizing the authors' conclusions (3).
For the sake of objectivity, I'll have to offer a few critiques of the wheat study too, so here goes.
Here's a brief list of my problems with this study:
This is not an in vivo study.
There is no full report of the methods or data.
The images supposedly demonstrating the data look awful.
The study is completely uncontrolled, and there is no way to conclude that the effect is unique to gluten and no way to conclude that the effect is even attributable to gluten rather than to the solvent or to any inflammatory contaminants.
1. This is not an in vivo study.
No one fed any wheat to anyone in this study. Concluding something about eating wheat from this study is therefore complete nonsense.
That's not to say that such a finding wouldn't be interesting. If it were convincing (and it isn't, for reasons described below), it would be a good reason to conduct a study feeding wheat to non-celiacs to see if it causes any inflammation. Then again, they should conduct such a study anyway.
The investigators found six people who did not have celiac, but were otherwise pretty sick. They took intestinal biopsies, incubated the cells in laboratory dishes, and challenged them with three proteins. One was the full gluten protein (gliadin), one was a synthetic imitation fragment of this protein 19 amino acids in length (19-mer), and one was a fragment 33 amino acids in length (33-mer) that had been treated with the enzyme transglutaminase in order to render it toxic.
Had they fed wheat to these people, the people would have substantially digested the gliadin molecule. Although the 19-mer and 33-mer fragments are particularly difficult to digest and are therefore thought to play a role in celiac, recent evidence suggests that microbial enzymes from bacteria in our mouths digest 33-mer (4) and evidence dating back seven years has suggested that in people who do not have active celiac disease, both 19-mer and 33-mer are totally degraded once they enter the cells that line the intestine (5).
On top of this, the authors state that the version of 33-mer they used was “deaminated.” This means that they treated it with an enzyme called tissue transglutaminase (TG).
Ordinarily, TG remains within our cells in an inactive form, but when our tissues get damaged, the cells activate it and release it so that it can start repairing the damaged tissue. However, it also modifies the 33-mer fragment of the gluten protein by stealing nitrogen from the amino acid glutamine and thereby converting it to the amino acid glutamate. This is in all or almost all instances required to make 33-mer “immunogenic.” In other words, the immune system will only mount a response to the gluten fragment after it has been processed by TG (6).
Surely, we can all see now why this study is worthless for telling us how the patients would have responded had they actually eaten wheat. Perhaps since these patients were all sick and were not in any remote sense a random sample of the population, they would have been producing some TG enzyme. Or, perhaps they would have fully digested the gluten and all its protein fragments from a mixture of microbial and endogenous enzymes beginning in the mouth and ending inside the intestinal cell.
2. There Is No Full Report of the Methods or Data
This study was published as a brief report, almost like a letter to the editor with pictures.
This suggests that the editors of the journal either found the study 1) only moderately interesting, or 2) too inconclusive to give it space for a full report.
If this study was the first of its kind to definitively show that wheat causes intestinal inflammation in non-celiacs, I would think that would be of great interest. The lack of details provided in this short format makes it very difficult to critically evaluate. Nevertheless, there are some things that stick out that suggest the study is almost uninterpretable.
3. The Images Supposedly Demonstrating the Data Look Awful
You can take a look at their figure on the second page here. Most of it looks like a blurry mess.
Ideally what you would want to see in a Western blot is a clear, distinct, relatively thin black line demonstrating the protein, in this case IL15. On one side you want to see a “ladder” showing various molecular weights and on the other a clean line representing your protein of interest, sometimes shown alongside a “positive control” that was purchased commercially.
Here's an example of a good Western blot (7):

On the right we see a ladder with different protein fragments of known molecular weight, each shown as black lines. On the left, we see several proteins that the authors isolated. We are confident they are the correct proteins because 1) the staining is associated with an antibody demonstrating some specificity to what they are looking for and 2) the lines appear at the correct molecular weight, as judged by the ladder on the right.
In our study, what we would like to see is a clear absence of the line in our control cells and the clear presence of a line indicating our protein of interest in the gluten-treated cells. Is that what we see? In some cases, kind of. In others, all I see is a blur.
Let's take a look:
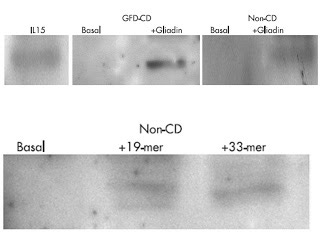
Rather than a ladder, we just have a positive control on the upper left, marked IL15. A ladder takes up a lot of space, so that's ok. But that should be the best-looking line, and instead it looks like a blur. We have the best-looking line in the third column showing a biopsy from a celiac patient treated with gluten. But is there a response to gliadin in the non-celiac individual shown in the upper right? I just see a massive blur.
In the second row, we see the cells treated with the 19-mer and 33-mer fragments. It kind of looks like there are some lines there, but they look pretty horrible.
Sometimes it's hard to get these images to copy into files or onto print. The computer can produce objective quantitative data that can be presented as a bar graph next to the images of the blots, but we don't have that here, perhaps because the journal wouldn't give the authors space. Still, I'd feel more confident about their findings if they could show us that the computer can see these lines, because they look pretty fuzzy to me.
Worst of all, you always submit your best images for publication. That means the others were probably even worse.
4. The Study Is Completely Uncontrolled
Even if we suspend our skepticism of the fuzzy lines and take the authors at their word that gliadin and its protein fragments caused the intestinal biopsies taken from sick non-celiac patients to produce IL15, the study is still completely uninterpretable because the authors did not use any appropriate controls.
Is this an effect specific to gluten and gluten fragments, or would virtually any protein or protein fragment have caused this effect? We don't know, because they didn't use a negative protein control.
Actually, the authors state that they expected 33-mer to have no effect on IL15:
and, although not expected, the “non-toxic” immunodominant 33-mer was also able to induce an innate response.
One way of looking at this is that their negative control failed and turned out positive. 33-mer is known for stimulating the immune system in other ways, but they only expected 19-mer to cause the production of IL15. Maybe many other proteins would elicit the same response.
But it gets worse. Was this even an effect of the protein, or was it an effect of the solvent? We don't know, because there was no vehicle control. In fact, since there is no “methods” section, we don't even know what they dissolved the proteins in!
Or, was it an effect of contaminants? The authors state that they discarded any contaminating endotoxin, but they do not state clearly whether they discarded it from the synthetic peptides or from the intestinal biopsies, or how they discarded it. Sometimes endotoxin purification can introduce other contaminants.
On the other hand, sometimes proteins purchased commercially are themselves already contaminated with endotoxin, which could produce an inflammatory response. In fact, this is so potentially problematic that any study showing an inflammatory effect of incubating cells with a protein purchased commercially should be viewed with extreme skepticism if the authors do not verify that it is free of endotoxin.
Conclusion: Consider Going Gluten-Free or Paleo Anyway!
I hope I've convinced some of you that this particular study absolutely can not be used to justify any dietary conclusions, let alone “wheat is inherently toxic and evil.”
However, if we waited for conclusive scientific evidence for everything we believe in or act on, we would vegetate. If it's possible that you're gluten-sensitive and you still have some unresolved health problems, why not go gluten-free? Heck, why not go full Paleo? It's just for January. If you feel better, stick with it and see what happens!
What's more, share your results with the rest of us! Let's fix up published literature and personal and clinical experience on a blind date. Once they embrace, we'll all be better off.
References
1. Bernardo D, Garrote JA, Fernandez-Salazar L, Riestra S, Arranz E. Is gliadin really safe for non-coeliac individuals? Production of interleukin 15 in biopsy culture from non-ceoliac individuals challenged with gliadin peptides. Gut. 2007;56(6):889-90. [pubmed link]
2. Nicholls SJ, Lundman P, Harmer JA, Cutri B, Griffiths KA, Rye KA, Barter PJ, Celermajer DS. Consumption of saturated fat impairs the anti-inflammatory properties of high-density lipoproteins and endothelial function. J Am Coll Cardiol. 2006. 15;48(4):715-20. [pubmed link]
3. Masterjohn C. The anti-inflammatory properties of safflower oil and coconut oil may bemediated by their respective concentrations of vitamin E. J Am Coll Cardiol. 2007;49(17):1825-6. [pubmed link]
4. Helmerhorst EJ, Zamakhchari M, Schuppan D, Oppenheim FG. Discovery of a novel and rich source of gluten-degrading microbial enzymes in the oralcavity. PLoS One. 201;5(10):e13264. [pubmed link]
5. Matysiak-Budnik T, Candalh C, Dugave C, Namane A, Cellier C, Cerf-Bensussan N, Heyman M. Alterations of the intestinal transport and processing of gliadin peptides in celiac disease. Gastroenterology. 2003;125(3):696-707. [pubmed link]
6. Tjon JM, van Bergen J, Koning F. Celiac disease: how complicated can it get? Immunogenetics. 2010;62(10):641-51. [pubmed link]
7. Moron B, Cebolla A, Manyani H, Alvarez-Maqueda M, Megias M, Thomas Mdel C, Lopez MC, Sousa C. Sensitive detection of cereal fractions that are toxic to celiac disease patients by using monoclonal antibodies to a main immunogenic wheat peptide. Am J Clin Nutr. 2008;87(2):405-14. [pubmed link]