
Vitamin D: The First Study on COVID-19 Infection Risk
Vitamin D: The First Study on COVID-19 Infection Risk

Today, the first study on the association between vitamin D status and infection risk was published in fully peer-reviewed and final form in the journal Nutrients (a journal I published part of my doctoral research in).
Background to the Issue
Up to this point, there have been four studies published as preprints associating vitamin D status with the severity of infection or the risk of dying, but none of them have examined the association with the risk of getting infected in the first place.
Here are my previous four newsletter issues on vitamin D:
In sum, this is what we knew, prior to today's paper:
Vitamin D status below 30 ng/mL is associated with more severe disease or with mortality in COVID-19 patients from South Asian, Indonesian, and Belgian (European) hospitals.
For mortality in Indonesia, the association persists after adjusting for age, sex, and preexisting conditions. For severity as judged by CT scan in Belgium, the association exists only in males.
25(OH)D close to 30 ng/mL and up to 35 ng/mL is associated with less severe outcomes, but their is precious little data above 35 ng/mL. There does not appear to be a level above this associated with complete freedom from severe disease, and one person in the most severe group in the Belgian study had a 25(OH)D of 55 ng/mL.
Here is what we still didn't know, prior to today's paper:
Whether the association is causal, and if so, whether vitamin D supplementation prevents, restrains, or reverses the disease.
If the association is causal, what the mechanisms involved are.
Whether there is a U-shaped curve where 25(OH)D at some level above 35 ng/mL is associated with worse disease.
Whether current 25(OH)D can predict future risk of disease or future severity of disease.
Whether vitamin D impacts the rate of infection (as opposed to disease severity or mortality).
The new paper provides no evidence of causality, mechanism, or prediction of future risk based on current levels, but it provides the first data on the association with the risk of infection (addressing the last bullet point), and we can analyze it for any hints of a U-shaped curve (addressing the third bullet point).
Background For Today's New Paper
Swiss and Italian researchers collaborated to analyze data from the patients of a Swiss hospital who were tested for COVID-19 between March 1 and April 14. The patients were tested because they had symptoms such as cough, sore throat, breathing difficulties, with or without fever, a feeling of fever, muscle pain, or sudden anosmia (loss of smell) or ageusia (loss of taste). Thus, the sample is all people who were sick, some of whom were sick with something else, some of whom were sick with COVID-19.
The vitamin D status testing had to be within seven weeks of the COVID-19 test, and they compared the positives and negatives to a larger sample of people who had their vitamin D status tested during the same seasonal period of 2019.
It turned out that vitamin D status was tested a median of 3 days after the COVID-19 test, so it reflects vitamin D status after the people are infected.
Results Of Today's New Paper
There were 107 patients who got tested, 27 positive, and 80 negative.
The median 25(OH)D was 11.1 ng/mL in positives and 24.6 ng/mL in negatives. This difference was statistically significant (p=0.004), which means there is a very low (0.4%) likelihood that such a difference would be observed as a result of random chance. The COVID-19 negative patients had 25(OH)D that was similar to 1377 controls tested in 2019, except that this much larger sample had approximately 20 outliers with 25(OH)D between 60 and 100 ng/mL, and none of the COVID-19 positives or negatives from 2020 had 25(OH)D that high.
When stratified by sex, everything lost statistical significance. This is unsurprising because the number of people in each group was reduced, causing statistical power to be lost. However, the 25(OH)D between males and females was similar within the positive group, and similar within the negative group, suggesting that biological sex does not alter the association. This is consistent with the Indonesian study showing that sex did not alter the association with mortality and inconsistent with the Belgian study showing the association with severity existed in males but not females.
When stratified by age, the association was only found in the 43 patients over the age of 70. In these patients, the median 25(OH)D of negatives was 23.1 ng/mL, and the median value of positives was 9.3 ng/mL (p=0.037). By contrast, in the 46 patients under the age of 70, the median in negatives was not stated in the text but appears from the graph to be about 25.6 ng/mL and the median in positives was 17.2 ng/mL. While the positives did have a somewhat lower value, this difference was not statistically significant (p=0.277).
A Closer Look
Why wasn't the association statistically significant under the age of 70?
The box-and-whisker plot provides some answers:
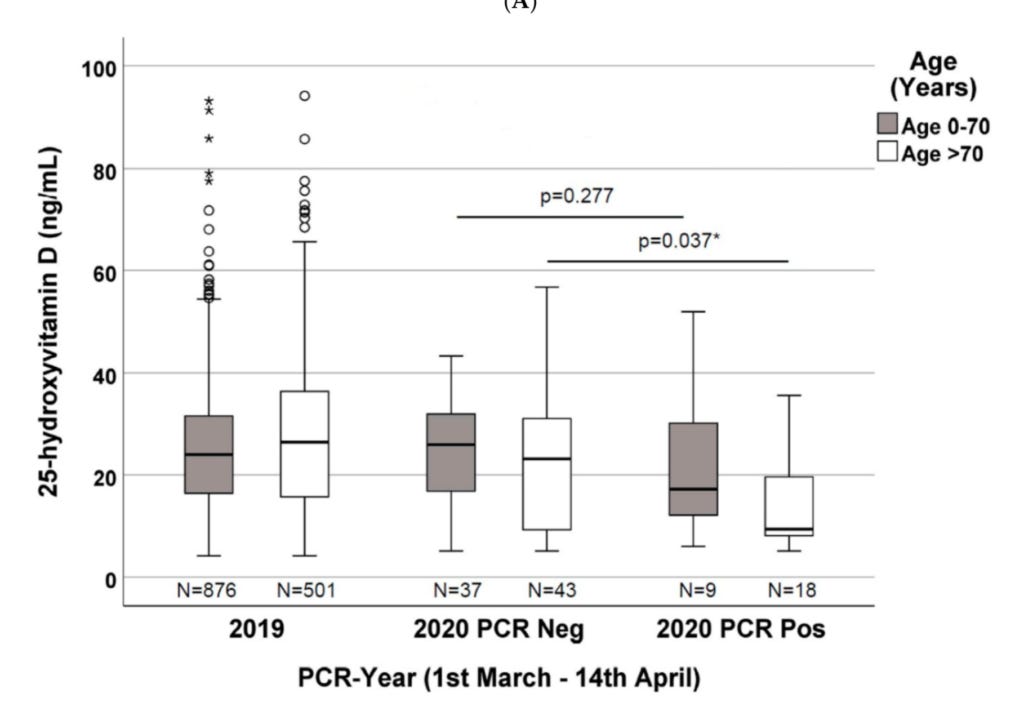
The line in the box is the median, or 50th percentile. This is the point at which 50% of people had lower values and 50% had higher. The lower boundary of the box is the 25th percentile, and the upper boundary of the box is the 75th percentile. The ends of the “whiskers” are the maximum and minimum values.
Let's first compare the negatives (middle) to the positives (right) under the age of 70 (gray) to see why the difference was not significant.
For the precise numbers besides the medians, I estimated them using the ruler in PowerPoint. These should be approximately correct, but if their graph is not perfectly scaled my numbers might be a little off.
Although the median was a little lower in the positives, the maximum value was actually higher in the positives (52 ng/mL) than in the negatives (43 ng/mL), and the 75th percentiles were almost identical (32 for negative, 30 for positive). The minimums of the two groups were also almost identical (close to 5 ng/mL). The median was lower because the bottom 50% of people in the positive group had lower 25(OH)D than the bottom 50% in the negative group; but the top 50% of the positive group more than made up for that. As a result, the ranges mostly overlap, except for the fact that the maximal value in the positive group was about 10 ng/mL higher than that in the negative group.
This actually seems to argue against a meaningful association in people under 70. They didn't provide a statistical analysis of the value of predicting a positive or negative COVID-19 result using 25(OH)D. But it seems like having a 25(OH)D of 25 ng/mL doesn't make you more likely to be negative than positive; it just makes you more likely to be in the top 50% of the positives and the bottom 50% of the negatives. Having 40 ng/mL actually makes you more likely to be found among the positives, and 50 ng/mL is only found among the positives.
Things look different over 70. The minimums (close to 5 ng/mL) and 25th percentiles (6 ng/mL for positives and 7 ng/mL for negatives) are almost identical, but the 75th percentiles are 20 ng/mL in the positive group and 31 ng/mL in the negative and the maximums are 35 in the positives and 57 in the negatives.
This suggests that in people over the age of 70, having a 25(OH)D around 30 ng/mL gives a very small chance of being positive, perhaps about 10%, while a 25(OH)D over 35 ng/mL is only found among negatives.
This finding that the association is limited to those over 70 is inconsistent with the Indonesian study finding that the association with mortality persists after adjusting for age, but the Indonesian study did not cover infection risk.
Are There Hints of a U-Shaped Curve?
On the one hand, one could argue that there are hints of a U-shaped curve for those under 70. Levels over 40 ng/mL are mostly found in positives, and levels over 43 ng/mL are only found in positives.
However, those same levels in the over-70 group are only found among negatives.
Unless we have strong biological plausibility for explaining why levels over 40 ng/mL would predispose young people to a higher infection risk and older people to a lower infection risk, I think we should avoid forming any conclusion here.
It is of course conceivable. Studies in rats but not humans show that older people have less ACE2, and perhaps the effect of vitamin D on ACE2, the entryway for the virus to get into a cell, differs by age.
Until we can arrive at a clear causal argument for the difference, however, I find it better to say that there remains too little data above 35 ng/mL to clarify whether it associates with higher or lower risk.
Although one could argue from these data that those under 70 should stick to 30 ng/mL and those over 70 should shoot for 35 ng/mL, given the small sample size of this study and the even smaller sample size of the age-specific subgroups, I am sticking to my position that 30-35 ng/mL should be the target. (I had previously capped this at 34 ng/mL, but this and the Belgian study favor 35 as fine and the difference is tiny).
What This Study Adds
This study is the second study done in Europe and the first study done in Switzerland.
It is the first study to show an association with infection risk, instead of just disease severity or mortality. This suggests that the antiviral activity of vitamin D shown for colds and flu might be relevant for COVID-19.
It suggests that age may modify the relationship between levels above 35 ng/mL and infection risk, but also suggests that maintaining 30-35 ng/mL will protect most people over 70 from becoming infected without hurting the infection risk of those under 70, if we interpret this as causal, which is a big if.
What We Still Don't Know
We still don't know whether the infection is depleting the vitamin D, whether the vitamin D is impacting the risk of infection, or both. We don't know if current vitamin D status can predict future infection risk, or if vitamin D supplementation would decrease the risk of infection. We have hints of a possible U-shaped curve in people under the age of 70, but whether a U-shaped curve exists remains unclear.
The Bottom Line
30-35 ng/mL 25(OH)D may protect against the risk of infection, as well as the infection becoming severe or fatal. For infection risk, this might be limited to those over 70. It is not clear whether vitamin D supplementation to maintain this range will be protective, but it appears harmless in the context of COVID-19 and possibly very beneficial.
Stay safe,
Chris
Please Support This Service
These research updates are made possible by purchases of The Food and Supplement Guide to the Coronavirus. The guide contains my most up-to-date conclusions about what we should be doing for nutritional and herbal support on top of hygiene and social distancing for added protection. Due to the absence of randomized controlled trials testing nutritional or herbal prevention, these are my best guesses for what is likely to work without significant risk of harm, based on the existing science.
Many people have asked why I am charging for this instead of giving it away for free, given that this is a time of crisis and people are in need.
Unfortunately, I have not been immune to the effects this virus has had on the economy. My revenue from my other offerings started falling in February, and by mid-March I had days where my revenue was zero. I have three people who work for me full-time, and I am doing everything I can to avoid laying any of them off. By mid-March I had depleted 75% of my emergency fund in order to avoid any layoffs, and without charging for the guide I would not have been able to hold out much longer.
Charging for the guide has allowed me to keep everyone working, replete some of my savings, and devote myself to researching COVID-19 full-time. As a result I now publish this daily COVID-19 Research Updates newsletter you are currently reading, am involved in the design of several clinical trials that are in the process of being submitted for registration now, and am able to continually update the guide for free whenever my research warrants it.
By purchasing the guide, you are enabling me to continue devoting my skills to the most important issue we now face. I am genuinely grateful for your contribution. You can purchase the guide using this link.
Disclaimer
I am not a medical doctor and this is not medical advice. I have a PhD in Nutritional Sciences and my expertise is in conducting and interpreting research related to my field. Please consult your physician before doing anything for prevention or treatment of COVID-19, and please seek the help of a physician immediately if you believe you may have COVID-19.
Subscribe
If you aren't subscribed to the research updates, you can sign up here.
Archive
You can access an archive of these updates here.
Comments and Questions
To leave a comment or question, please use the Facebook post for this newsletter.
*Footnotes
* The term “preprint” is often used in these updates. Preprints are studies destined for peer-reviewed journals that have yet to be peer-reviewed. Because COVID-19 is such a rapidly evolving disease and peer-review takes so long, most of the information circulating about the disease comes from preprints.