
What Can Modern Toxicology Tell Us About Food Toxins and Food Intolerances?
What Can Modern Toxicology Tell Us About Food Toxins and Food Intolerances?

“The dose makes the poison.” — Paracelsus (1493-1541)
“What is food to one is bitter poison to others.” — Lucretius (ca. 99 BC — ca. 55 BC)
This post will be the first in a series of posts on food toxins and food intolerances. As an introduction, I'd like to review some of the recent advances in our understanding of toxicology, to see how a basic understanding of toxicology might be able to shed some light on the toxicity of foods.
Although the sayings attributed to Paracelsus and Lucretius above may seem contradictory, taken together they capture two central concepts of modern toxicology. Some drugs, for example, are just inherently toxic at high enough doses. Reactions to these drugs are called type 1, type A, or “intrinsic” adverse drug reactions. Other drugs only produce toxicity in suscpetible individuals. Reactions to these drugs are called type 2, type B, or “idiosyncratic” drug reactions. Some authors call them “bizarre” drug reactions (1). Idiosyncratic reactions are estimated to account for 13% of all drug-induced liver injury (2) and somewhere between 5% and 20% of all adverse drug reactions (1).
In reality, the separation of drugs into some that produce “intrinsic” toxicity and others that produce “indiosyncratic” toxicity is probably an illusion. For example, acetaminophen (e.g., Tylenol) is the drug most commonly responsible for intrinsic drug reactions, but over a third of people develop clear signs of liver toxicity when taking the maximal dose allowed on the label, while nearly a fifth of people tolerate the dose with complete impunity (3).
One review (4) recently argued that all drugs have a therapeutic curve and a toxicity curve, but with drugs whose toxicity is usually called “idiosyndratic” the toxicity curve just lies much further away from the therapeutic curve:
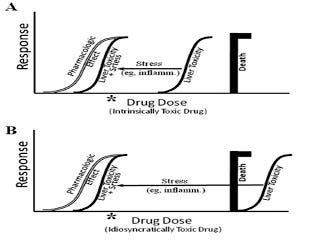
Figure from Roth, R.A. and P.E. Ganey, Intrinsic versus idiosyncratic drug-induced hepatotoxicity–two villains or one? J Pharmacol Exp Ther, 2010. 332(3): p. 692-7.
In the case of the intrinsic reaction, shown at the top, the therapeutic (left) and toxicity (right) curves are fairly close together, so that toxicity predictably develops at a high dose. However, as indicated by the arrow, individual susceptibility can shift the toxicity curve leftward so that it overlaps with the therapeutic range. This would allow, for example, someone to develop toxicity taking Tylenol at an approved dosage.
In the case of the idiosyncratic reaction, shown at the bottom, the therapeutic (left) and toxicity (right) curves are very far apart. Since the liver toxicity curve lies to the right even of the lethal dose, liver toxicity never develops under normal conditions. However, once again, individual susceptibility can shift the toxicity curve leftward so that it overlaps with the therapeutic range. This allows the “idiosyncratic” or “bizarre” reaction to occur.
In other words, these aren't two types of reactions, but they are two principles that are important in any toxic reaction: how dangerous the toxin is, and how susceptible the person is.
Food toxicities and intolerances also clearly involve both principles. On the one hand, celiacs predictably improve in the majority of cases by removing gluten from their diets and many non-celiacs benefit as well. On the other hand, many people eat grains, beans, peanuts, salicylates, oxalates, glutamates, amines, polyphenols, barbecued meat, bacon, and every other potentially toxic food and food chemical with impunity until they die at a ripe old age, sometimes over the age of 100.
What, then, contributes to this individual susceptibility?
Let's turn again to modern drug toxicology and see what we find.
Here are a few of the well studied factors that contribute to individual susceptibility:
Nutritional Status. Acetaminophen causes toxicity in part by causing a massive 90% depletion of glutathione, the master antioxidant and detoxifier of the cell. (See my related blog post, “The Biochemical Magic of Raw Milk and Other Raw Foods: Glutathione.”) The standard treatment is N-acetyl-cysteine, a highly bioavailable form of the amino acid cysteine, which our cells use to make glutathione. It is especially effective at mitigating the toxicity of acetaminophen when provided during the first ten hours of toxicity (5).
Intestinal Flora. In the 1970s and 1980s, researchers provided compelling evidence that the mechanism by which galactosamine, carbon tetrachloride, and halothane produce liver toxicity is by causing the movement of endotoxin from the gut into the bloodstream (6). If they added endotoxin, the toxicity increased. If they provided any number of materials that “mop up” endotoxin in the intestine, without adding any additional endotoxin, they could prevent the toxicity of these chemicals. Nowadays, researchers are investigating the role of endotoxin in priming a person to idiosyncratically react to the antidepressant chlorpromazine, the antihistamine ranitidine, the antibiotic trovafloxacin, and several NSAIDs. Endotoxin is a component of the cell wall of gram-negative bacteria. Many stressors can temporarily increase the transport of endotoxin across the intestinal barrier, while probiotics decrease the levels of endotoxin in the intestine.
Genes. C57BL/6 mice are used for many experiments. Although researchers often make additional genetic modifications to these mice, they are actually already genetically defective: they have a genetic deficiency of the enzyme that converts the B vitamin niacin from its NADH form to its NADPH form, which is needed to recycle glutathione (7). Researchers have further used these mice to create a deficiency of the maganese-dependent enzyme superoxide dismutase, which, like glutathione, is critical to the cell's natural antioxidant defense system. These mice suffer from poor mitochondrial function as a result. They develop toxic reactions to flutamide (7) and troglitazone (8), two drugs that are considered “idiosyncratic” and are otherwise difficult to use to produce toxicity in animals. About one in 5,000 people have a similar genetic mutation, although many people may have poor mitochondrial function for nutritional, lifestyle, and other reasons.
Immunological Reactions. About a fifth of idiosyncratic liver toxicity is associated with immunological signs and symptoms such as eosinophilia (an increase in a certain type of immune cell in the blood), rash, fever, and autoimmune antibodies or antibodies to drug-modified proteins; when these occur, they generally occur within one to six weeks after beginning the drug (9). Some authors argue that the immune system could confuse “self” and “nonself” when toxic drugs form complexes with proteins, causing the immune system to recognize the protein itself as toxic (10). Others argue that the immune system does not have anything to do with recognizing “self” or “nonself” but instead recgonizes “danger,” and that it is tissue damage that causes the immune system to come along and clean up the mess, including cleaning up our own proteins when they are damaged or spilling out where they don't belong (11). The role that these immunological reactions play in toxicity, whatever their cause, remains obscure.
This is not a comprehensive list of factors that affect drug toxicity, but it contains some of the most important kinds of factors, and gives us a clue what types of things to look for when understanding why some foods are toxic.
Here's a brief outline of some of the factors that are most likely to be involved in food toxicity and food intolerance:
The intrinsic toxicity of the food.
Proper preparation of the food to neutralize the toxins.
Genetic, and perhaps epigenetic, variations in the activities of enzymes and other proteins that activate the toxin, detoxify the toxin, transport the toxin, or mount an immunological response to the toxin.
Variations in intestinal flora, including bacteria that degrade the toxin or bacteria that counteract the body's detoxification mechanisms.
Secretion of sugars such as mannose into the digestive system that bind to lectins (such as gluten) and protect against their toxicity.
Secretion of IgA antibodies into the intestinal tract, which bind to undigested food particles and protect against their toxicity.
Variations in nutritional status, including nutrients involved in modulating the immune response, supporting detoxification mechanisms, and protecting the integrity of the gastrointestinal tract.
How these factors should be expected to affect the toxicity of wheat, other grains, beans, oxalates, amines, salicylates, and various other foods and food toxins will be the subject of upcoming blog posts.
Stay tuned!
References
1. Pirmohamed, M., Pharmacogenetics of idiosyncratic adverse drug reactions. Handb Exp Pharmacol, 2010(196): p. 477-91.
2. Holt, M. and C. Ju, Drug-induced liver injury. Handb Exp Pharmacol, 2010(196): p. 3-27.
3. Watkins et al., Aminotransferase elevations in healthy adults receiving 4 grams of acetaminophen daily: a randomized controlled trial. JAMA. 2006 Jul 5;296(1):87-93.
4. Roth, R.A. and P.E. Ganey, Intrinsic versus idiosyncratic drug-induced hepatotoxicity–two villains or one? J Pharmacol Exp Ther, 2010. 332(3): p. 692-7.
5. Hinson, J.A., D.W. Roberts, and L.P. James, Mechanisms of acetaminophen-induced liver necrosis. Handb Exp Pharmacol, 2010(196): p. 369-405.
6. Lind, R.C., et al., The involvement of endotoxin in halothane-associated liver injury. Anesthesiology, 1984. 61(5): p. 544-50.
7. Kashimshetty, R., et al., Underlying mitochondrial dysfunction triggers flutamide-induced oxidative liver injury in a mouse model of idiosyncratic drug toxicity. Toxicol Appl Pharmacol, 2009. 238(2): p. 150-9.
8. Ong, M.M., C. Latchoumycandane, and U.A. Boelsterli, Troglitazone-induced hepatic necrosis in an animal model of silent genetic mitochondrial abnormalities. Toxicol Sci, 2007. 97(1): p. 205-13.
9. Pachkoria, K., et al., Genetic and molecular factors in drug-induced liver injury: a review. Curr Drug Saf, 2007. 2(2): p. 97-112.
10. Pessayre, D., et al., Mitochondrial involvement in drug-induced liver injury. Handb Exp Pharmacol, 2010(196): p. 311-65.
11. Li, J. and J.P. Uetrecht, The danger hypothesis applied to idiosyncratic drug reactions. Handb Exp Pharmacol, 2010(196): p. 493-509.