
ACE2 Probably Does Not Explain Why Older Males Have More Severe Disease
ACE2 Probably Does Not Explain Why Older Males Have More Severe Disease

In an April 16 YouTube video titled “Vitamin D may reduce susceptibility to COVID-19-associated lung injury,” Dr. Rhonda Patrick of Found My Fitness suggested that older people have more severe COVID-19 outcomes than younger people and males have more severe outcomes than females because each of these groups has lower ACE2.
This was in the context of an argument that, although ACE2 is the entryway of the virus into the cells, the normal healthful physiological function of ACE2 is needed to protect against the most severe aspects of the disease, and one of the ways the virus damages the lungs is to lower the ACE2 available for this healthful function.
In support of her point about age and sex, she cited a paper showing that ACE2 declines with age, and does so more in males than females, in the lungs of rats.
In my response, I pointed out that ACE2 expression had recently been measured in the lungs of humans, and it did not differ by age or sex.
The preprint* released two days ago that I covered yesterday as the first paper to address whether human airway ACE2 is impacted by ACE inhibitors or angiotensin receptor blockers (ARBs) is also the second paper to address whether ACE2 in the human airway varies by age or sex, and it has confirmed the findings of the first paper showing that it does not.
The first paper was a collaboration by researchers from Google, Cold Spring Harbor Laboratory, Stony Brook, Johns Hopkins, and Hofstra.
They analyzed data collected in The National Cancer Institute's The Cancer Genome Atlas Program, which analyzed the gene expression in over 20,000 samples of 33 cancers and matched controls. The authors of this paper downloaded the data to perform statistical analyses on it.
As you can see from the figure below, the variation in ACE2 expression within human lung tissue was broad, but the data is spread randomly across the age groups and the sexes:

This is showing mRNA expression, which is the copy of the genetic information used by the cell to make a protein. mRNA expression sometimes, but not always, predicts how much protein would be found in the same cell.
They did include original lab work showing that ACE2 mRNA strongly correlates with ACE2 protein in isolated human cancer cells (r=0.82, strong enough to explain 67% of the variation), but this doesn't mean that it correlates as strongly in male and female human lung tissue across the age groups they studied.
The second paper was a collaboration by researchers from the medical schools of Stanford, Columbia, University of Minnesota, UC San Diego, and Taiwan's China Medical School.
In this paper, they used a technique known as immunofluorescence to examine archived samples of nasal tissue.
Immunofluorescence is used to image the protein, and can be used both to quantify the amount of protein and also to show where it is found in the cell. This is far better suited to addressing how ACE2 expression impacts COVID-19 risk, because it is the ACE2 protein on the surface of the cell, not the amount of mRNA, that matters.
While the first paper looked at the lung, part of the lower respiratory tract, this paper is looking at the nose, part of the upper respiratory tract.
The data below are for ages below and above 65 in three cohorts: Stanford (left), National Taiwan University (middle), and China Medical University (right).

There are no statistically significant differences between the age groups in any cohort, but there does seem to be a possible trend toward lower ACE2 in the higher-age groups of the first two cohorts. Certainly, the data is not as randomly spread across the age groups as is the mRNA expression data from the first study.
Still, even if a larger study were to show statistical significance, the size of the possible effect looks small, with the median about 22% lower in the Stanford Cohort and 14% lower in the National Taiwan University cohort.
For sex, the data is spread more randomly:
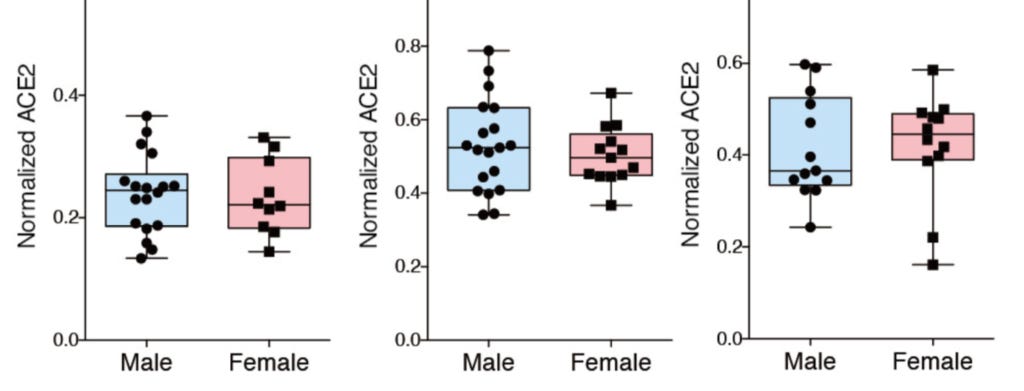
Females have slightly lower ACE2 in the Stanford and National Taiwan University cohorts, somewhat greater ACE2 in the China Medical University cohort, and none of the differences are statistically significant.
The first study looked at the lung, the second looked at the nose. The first study had a much larger data set than the small study. The mRNA expression of the first study looks like a completely random distribution across multiple age groups and between males and females. The protein expression of the second study does not look quite as random, but there are no significant differences for age or sex. It is conceivable that a larger study of protein content could show a difference, but the data accumulated so far do not support any difference in human airway ACE2 expression.
For why older males are at greater risk of severe COVID-19 than females or younger males, we probably have to look elsewhere.
Stay safe,
Chris
Please Support This Service
These research updates are made possible by purchases of The Food and Supplement Guide to the Coronavirus. The guide contains my most up-to-date conclusions about what we should be doing for nutritional and herbal support on top of hygiene and social distancing for added protection. Due to the absence of randomized controlled trials testing nutritional or herbal prevention, these are my best guesses for what is likely to work without significant risk of harm, based on the existing science.
Many people have asked why I am charging for this instead of giving it away for free, given that this is a time of crisis and people are in need.
Unfortunately, I have not been immune to the effects this virus has had on the economy. My revenue from my other offerings started falling in February, and by mid-March I had days where my revenue was zero. I have three people who work for me full-time, and I am doing everything I can to avoid laying any of them off. By mid-March I had depleted 75% of my emergency fund in order to avoid any layoffs, and without charging for the guide I would not have been able to hold out much longer.
Charging for the guide has allowed me to keep everyone working, replete some of my savings, and devote myself to researching COVID-19 full-time. As a result I now publish this daily COVID-19 Research Updates newsletter you are currently reading, am involved in the design of several clinical trials that are in the process of being submitted for registration now, and am able to continually update the guide for free whenever my research warrants it.
By purchasing the guide, you are enabling me to continue devoting my skills to the most important issue we now face. I am genuinely grateful for your contribution. You can purchase the guide using this link.
Disclaimer
I am not a medical doctor and this is not medical advice. I have a PhD in Nutritional Sciences and my expertise is in conducting and interpreting research related to my field. Please consult your physician before doing anything for prevention or treatment of COVID-19, and please seek the help of a physician immediately if you believe you may have COVID-19.
Subscribe
If you aren't subscribed to the research updates, you can sign up here.
Archive
You can access an archive of these updates here.
Comments and Questions
To leave a comment or question, please use the Facebook post for this newsletter.
*Footnotes
* The term “preprint” is often used in these updates. Preprints are studies destined for peer-reviewed journals that have yet to be peer-reviewed. Because COVID-19 is such a rapidly evolving disease and peer-review takes so long, most of the information circulating about the disease comes from preprints.