If there’s a single vitamin you need to know more about, it’s vitamin K2. The first reason is you’re probably not getting enough. The second is that it doesn’t get the attention it deserves, and it’s really hard to find reliable and easy-to-use information about it.
This resource is meant to change that. It begins by teaching you everything you need to know about the vitamin, including its benefits, how much you need, and how to get it from food. It includes shareable infographics to make the concepts fun and easy to understand. Finally, it provides reviews of the available supplements and a searchable database of the vitamin K2 contents of foods that can’t be found anywhere else.
If you’re a beginner, you can read the article straight through or pick the parts that are most interesting or useful to you. If you are an advanced user and already know a lot about vitamin K2 or have a strong science background, you can click on the buttons that say “click here for a more detailed explanation” in order to expand descriptions that are better suited to your level of expertise.
The Health Benefits of Vitamin K2
Vitamin K2 has a wide range of underappreciated health benefits:
-
- It prevents calcium from going into all the wrong places and makes sure it gets into all the right places. For example, it keeps it out of your kidneys, where it would cause kidney stones, and keeps it out of your blood vessels, where it would cause heart disease, but helps it to get into your bones and teeth, making your bones strong and your teeth resistant to cavities.
- It helps you make insulin and remain very sensitive to insulin. This means it helps stabilize your blood sugar, protects against diabetes, and prevents the metabolic problems that often arise as a consequence of obesity.
- It promotes sexual health by helping you optimize your sex hormones. For example, it increases testosterone and fertility in males, and it helps bring the high levels of male hormones found in women with polycystic ovarian syndrome (PCOS) back down to normal.
- It helps improve exercise performance by enhancing your ability to utilize energy during bouts of physical activity.
- It protects against cancer by suppressing the genes that make cells cancerous and expressing the genes that make cells healthy.
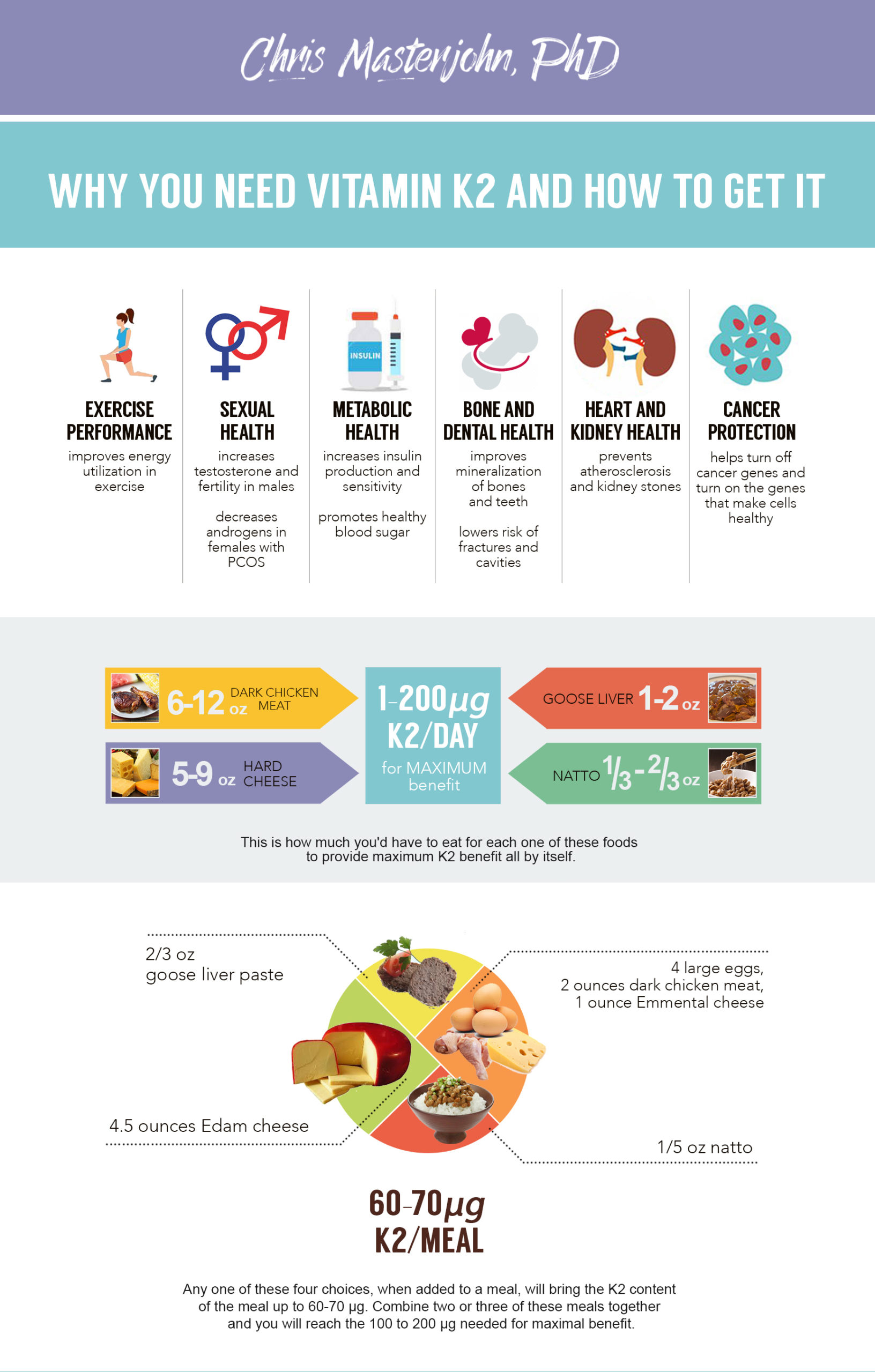
These roles are shown in the shareable infographic below. You can share it using the button in the upper right corner, or the buttons on the bottom strip. You can even use the button in the upper right corner to generate an embed code to share it on your own site if you have one.
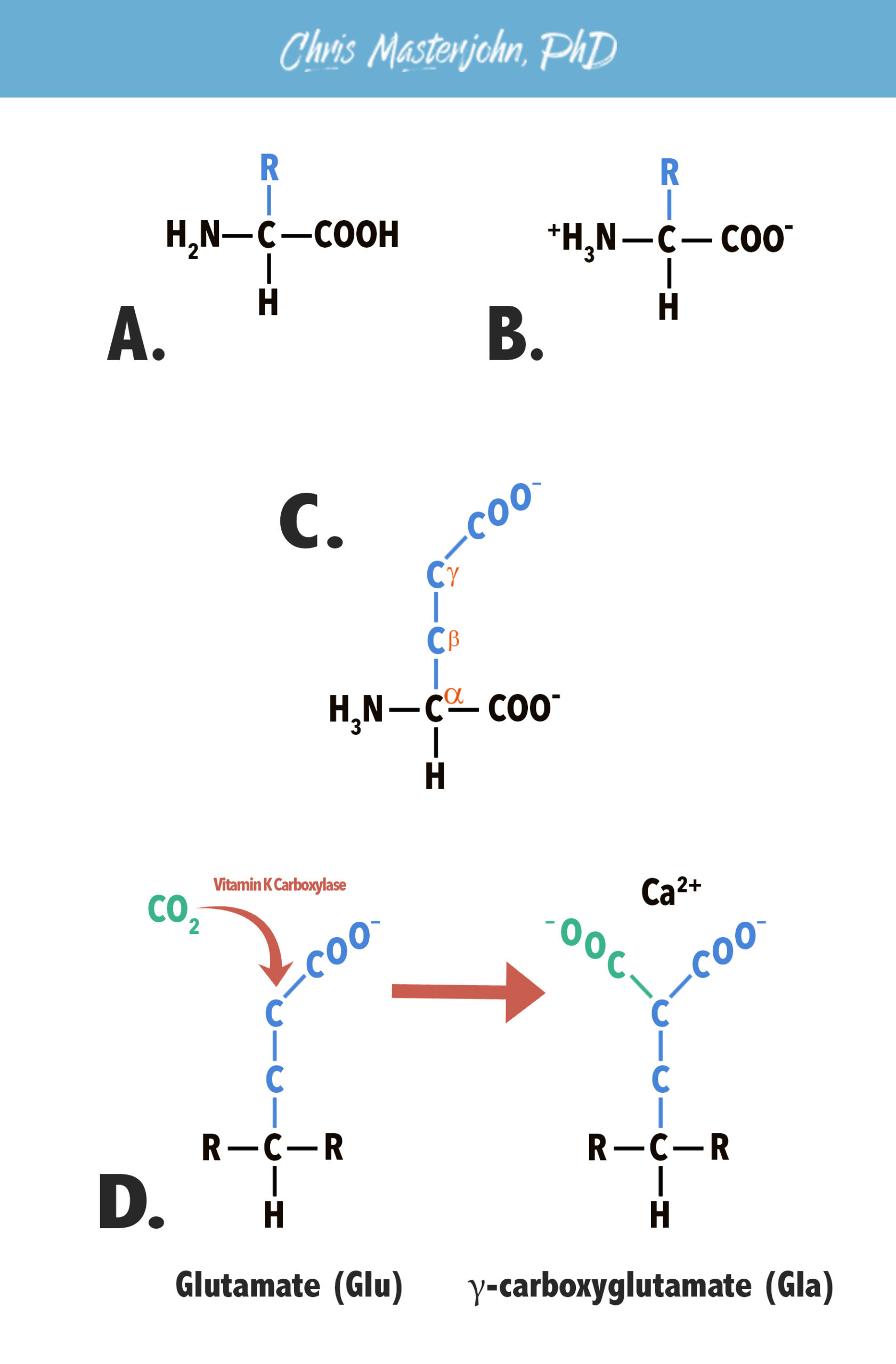
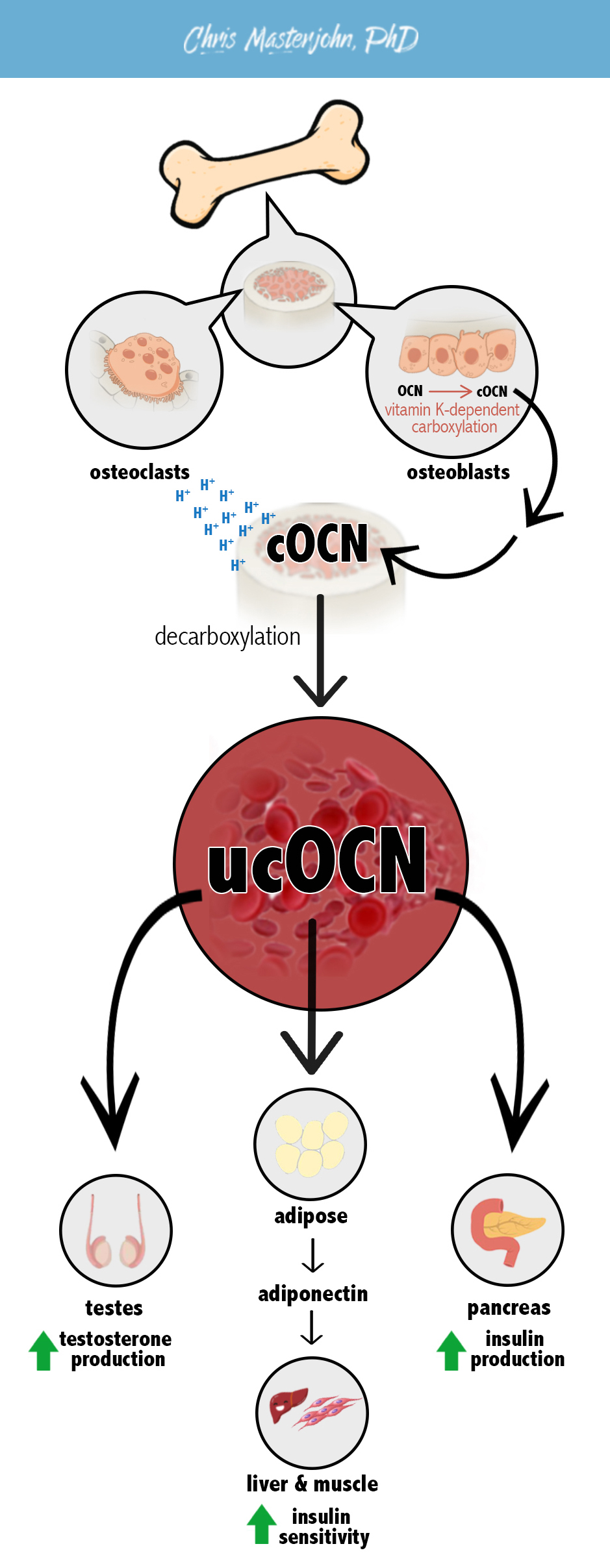
Vitamin K2‘s best-known and most well-established role is as a cofactor for the vitamin K carboxylase. This is a role that it shares equally with vitamin K1. The difference between vitamins K1 and K2 is discussed below, and in this section I will simply refer to “vitamin K.” The vitamin K carboxylase is an enzyme that adds carbon dioxide to the side chains of specific glutamate residues within specific vitamin K-dependent proteins. Once added to a glutamate residue, the carbon dioxide becomes a carboxyl group, so the process is known as carboxylation. Carboxyl groups carry negative charges, so carboxylation helps vitamin K-dependent proteins bind to calcium, which carries a positive charge. In other words, the most well-established role of vitamin K is to add carbon dioxide to proteins and thereby give them the ability to bind calcium. Since the carboxyl group is added to the third carbon of the glutamate sidechain, known as the gamma (𝛄) carbon, the process is known as 𝛄-carboxylation. Once modified in this way, glutamate becomes 𝛄-carboxyglutamate and is abbreviated “Gla.” Thus, vitamin K-dependent proteins often have the term “Gla” in their names. The figure below shows vitamin K-dependent 𝛄-carboxylation in more detail. A. The general structure of an amino acid, featuring a carboxyl group (COOH) on the right. B. At the pH range that prevails within the human body, carboxyl groups often ionize, giving them a negative charge. C. Glutamate. Moving from the central carbon through each carbon of the side chain, we label the carbons alpha (α), beta (β), and gamma (ɣ). Since the side chain carboxyl group is attached to the ɣ carbon, it is known as a ɣ-carboxyl group. D. ɣ-carboxylation. The vitamin K carboxylase uses vitamin K as a cofactor to add carbon dioxide to the ɣ carbon of the glutamate residue side chain. This converts glutamate, abbreviated Glu, to ɣ-carboxylglutamate, abbreviated Gla. The second ɣ-carboxyl group gives the side chain a second negative charge, which improves its ability to bind to calcium, which carries a positive charge. Although ionic calcium is shown in the figure, some vitamin K-dependent proteins bind to calcium salts rather than calcium ions. There are a wide variety of vitamin K-dependent proteins made in different tissues that fulfill different functions but that all undergo the same process of 𝛄-carboxylation. In each case, calcium-binding is essential for the protein’s activities. However, the role that calcium-binding plays is different for different proteins. We have known about the importance of vitamin K for blood clotting since the 1930s (Suttie, 2014). Blood clotting is regulated by a variety of proteins known as clotting factors that are all made in the liver and sent out into the blood, where they circulate in inactive form until blood vessel damage makes clotting necessary. In the clotting factors, vitamin K-dependent 𝛄-carboxylation allows calcium to serve as a structural “glue” that binds the protein into an active shape. Initially, we only knew that vitamin K was necessary to the function of prothrombin, the precursor to thrombin, which activates fibrinogen to fibrin to form blood clots. We now know that vitamin K is also needed for properly functioning factors VII, IX, and X, which are pro-coagulant proteins involved in the conversion of prothrombin to thrombin. Vitamin K is just as necessary for the function of proteins S and C, which act as anticoagulants by inactivating other clotting factors that are not dependent on vitamin K, factors V and VIII. There is a seventh vitamin K-dependent plasma protein, protein Z, that may have additional anticoagulant functions. Thus, vitamin K is required for the proper function of both procoagulants and anticoagulants within the clotting cascade and serves as a raw material necessary for the proper regulation of blood clotting rather than serving as a coagulant or an anticoagulant itself. Vitamin K is necessary for the carboxylation of osteocalcin, a protein produced in bone and also sometimes referred to as bone Gla protein. In this case, vitamin K-dependent 𝛄-carboxylation allows osteocalcin to bind to the calcified extracellular matrix of bone tissue (Koshihara, 1997). Scientists first discovered osteocalcin in the 1970s. Since it was made in bone, most scientists in the field assumed that it played an important role in mineralizing bone or in regulating the turnover of bone mineral or the structural organization of bone. In the 1990s, however, scientists produced the osteocalcin-knockout mouse, which is genetically modified to lack the gene that codes for osteocalcin. Osteocalcin knockout mice have no obvious defects in any measures of bone health. Their bones are adequately mineralized, and although their structural architecture is slightly different than that of normal mice, one study found their bones were stronger than those of normal mice (Ducy, 1996) and the worst that could be said about their bone architecture was that it seemed “less mature” than that of normal mice (Boskey, 1998). For three decades, the role of osteocalcin was elusive and the statements made about its function were vague and unconvincing. In 2007, things began to change (Lee, 2007). The scientists who had developed the osteocalcin knockout mouse began more intensively investigating their phenotype and publishing papers about their metabolic and hormonal health. And here, unlike in bone, the effects of osteocalcin are dramatic. Osteocalcin knockout mice are fat, deficient in insulin (like type 1 diabetics), insensitive to insulin (like type 2 diabetics), and they have low metabolic rates and high blood sugar. The males are also infertile and have low testosterone (Oury, 2011). Surprisingly, all of this is reversed with undercarboxylated osteocalcin rather than fully carboxylated osteocalcin. Undercarboxylated osteocalcin is produced by bone when vitamin K status is inadequate, and its circulation in serum had been interpreted as a sign of vitamin K inadequacy right up through the publication of these papers. In fact, some vitamin K researchers argue that it should still be used in this way, adding controversy to the implications of the osteocalcin knockout mouse studies (Booth, 2013). I believe the best way to reconcile these conflicting ideas is as follows: vitamin K-dependent 𝛄-carboxylation of osteocalcin takes place in osteoblasts and allows the carboxylated osteocalcin (cOCN) to leave the osteoblasts and accumulate in bone matrix, which is its proper site of storage. During bone resorption, osteoclasts produce acid that decarboxylates osteocalcin and releases it into the serum in its undercarboxylated form (ucOCN) (Ferron, 2007; Oury, 2013). From there, it acts on multiple tissues to improve insulin secretion, insulin sensitivity, blood glucose, the metabolic rate, body composition, and, in males, testosterone production and fertility. This is illustrated in the figure below. Vitamin K is necessary for the carboxylation of matrix Gla protein (MGP), which is made primarily in vascular smooth muscle cells and chondrocytes (cartilage cells) (Luo, 1997). Wherever there is a blood supply, there is MGP, so MGP is made throughout the body. In this case, vitamin K-dependent 𝛄-carboxylation allows MGP to bind calcium so that it can prevent calcium from going into the wrong places, like into the kidneys and blood vessels, and help it go into the right places, like the extracellular matrix of bones and teeth. MGP appears to act primarily by limiting the formation of calcium salts. This helps prevent pathological calcification of soft tissues (tissues other than the bones and teeth). For example, MGP protects against kidney stones and against the calcification of blood vessels that occurs in heart disease. Bone has a complex protein infrastructure that becomes mineralized through the entry of very small calcium phosphate salts from blood. By limiting the size of these salts (Price, 2009), MGP helps them penetrate bone matrix and support its mineralization. MGP also supports growth during infancy, childhood, and adolescence by preventing premature calcification of the cartilage that helps bones to become larger. These roles of MGP are illustrated in the figure below. As described below, different forms of vitamin K reach different tissues to different degrees, so some forms better support some of the health outcomes discussed above than others. However, all the roles described above can be fulfilled by any form of vitamin K able to reach the relevant tissues. By contrast, MK-4 is a subform of vitamin K2 that has a unique role in regulating gene expression (Ichikawa, 2007; Ito, 2011). The mechanisms involved are unclear: some studies show that it binds to the steroid X receptor (SXR), while others show that it regulates gene expression through SXR-independent mechanisms. One of those mechanisms is to stimulate the phosphorylation of protein kinase A (PKA), but how it does this is also unclear: some studies show that it increases cyclic AMP (cAMP), a traditional PKA activator, while other studies show it activates PKA independently from cAMP. In other words, we know that MK-4 regulates gene expression, but we have a lot to learn about how it does this. Through its regulation of gene expression, MK-4 favors bone growth, protects against cancer, and increases the production of sex hormones. There are a variety of other vitamin K-dependent proteins whose functions are less clearly understood (Suttie, 2014). These include the following: Gla-rich protein, which accumulates in soft tissues during pathological calcification; periostin, which may be necessary for growth; Gas6, which promotes cell survival, and, along with protein S, helps clear away the debris of dead cells (for example, in atherosclerosis, where accumulating debris of dying cells causes a dangerous inflammatory state); and a family of four transmembrane Gla-rich proteins may act as cell surface receptors. Vitamin K also supports the production of important sulfur-based lipids known as sulfatides in the brain, and accumulates in the mitochondrion where it may play a direct role in the electron transport chain, as it has been shown to do in fruit flies (Vos, 2012). We can have varying degrees of confidence in different health benefits attributed to vitamin K. In this section, I refer generally to vitamin K. I discuss the difference between vitamins K1 and K2 below. This section is meant to be readable on its own, but if you don’t have a background in the biochemistry of vitamin K, it will be helpful to read the biochemistry section first. The only incontrovertible effect of vitamin K is to support blood clotting (Suttie, 2014). On this basis, vitamin K is used to prevent hemorrhage in infants and inhibitors of vitamin K recycling such as warfarin and other 4-hydroxycoumarins are used as the principle anticoagulant therapy. Genetic deficiencies in vitamin K-dependent clotting factors lead to well characterized coagulation disorders, and otherwise fatal cases of bleeding can be rescued with fully carboxylated clotting factors. Thus, there is no room for a reasonable person to doubt this role of vitamin K. Vitamin K supports the carboxylation of matrix Gla protein (MGP), which controls the distribution of calcium in the body and thereby supports the mineralization of bones and teeth, prevents the pathological calcification of soft tissues such as the heart, blood vessels, and kidneys, and supports growth during early development by preventing the premature calcification of growth plates. These roles are most clearly demonstrated in the MGP knockout mouse (Luo, 1997). It has short stature because of calcified growth plates, suffers from osteopenia and spontaneous fractures, and dies within two months due to the rupture of heavily calcified blood vessels. In other words, calcium fails to go into the right places (bone) and instead goes into all the wrong places (blood vessels and the growth plate cartilage). The evidence that MGP plays the same role in humans is extensive, and the sections below discuss that evidence in the context of each specific health benefit. The evidence for the importance of vitamin K in heart health is compelling. Uncarboxylated MGP accumulates in atherosclerotic plaque in proportion to the amount of calcium deposited in the plaque (Roijers, 2011) and circulates in plasma in proportion to the severity of vascular calcification (Schurgers, 2010; Dalmeijer, 2013). Inhibitors of vitamin K recycling such as warfarin and other 4-hydroxycoumarins worsen blood vessel calcification in patients at risk for heart disease (Zhang, 2014). People who consume more vitamin K2 in the diet have a lower risk of heart disease (Geleijnse, 2004; Gast, 2009; Buelens, 2009; Zwakenberg, 2016). Two different randomized controlled trials lasting three years support the role of vitamin K in heart health: one showed that vitamin K1 prevents the worsening of arterial calcification (Shea, 2009) and the other showed that vitamin K2 reduces arterial stiffness (Knapen, 2015). The first randomized controlled trial using vitamin K2 to prevent or reverse arterial calcification is currently underway and will likely be finished by 2018 (Vossen, 2015). Thus, a wide array of observational and experimental evidence in humans agrees that dietary vitamin K supports heart health. A number of randomized controlled trials from Japan have shown that a very high pharmacological dose (45 mg/day) of vitamin K2 as MK-4 exerts powerful protection against fracture risk in women with osteoporosis (Iwamoto, 2013). However, this pharmacological dose is far higher than what anyone could obtain from food, so its effects cannot be generalized to K2-rich foods or supplements using nutritionally relevant doses. The question is whether nutritional doses, which I would define as those under one milligram per day, offer meaningful support to bone health. Observational studies have associated the use of vitamin K antagonists as anticoagulants with lower bone mineral density (Caraballo, 1999) and have associated self-reported vitamin K intake with higher bone mineral density (Macdonald, 2008; Kim, 2015) and a lower risk of hip fracture (Apalset, 2011). Similarly, intake of natto, the richest source of vitamin K2, is associated with less bone loss over time in postmenopasual women (Ikeda, 2006). There are several randomized controlled trials (RCTs) using nutritional (100-200 μg/d) or borderline nutritional (1.5 mg/d) doses of vitamin K that suggest improvements in bone health, but they are not consistently convincing. Some show the improvement only in the lumbar spine (lower back) (Inoue, 2001; Moschonis, 2011; Kanellakis, 2012), and others only in the forearm (Koitaya, 2014; Bolton-Smith, 2007); one claims a benefit on the basis that bone health got worse in the control group or better in the vitamin K group without any difference between the two groups at the end of the study (Koitaya, 2014); and none of them report an improvement in whole body BMD or a decrease in the risk of fracture. Among all of the RCTs, the most convincing one showed that three years of 180 μg/d vitamin K2 as MK-7 improved several measures of bone health in postmenopausal women when compared to a placebo (Knapen, 2013). Bone mineral density and bone mineral content both increased at the lumbar spine (lower back) and femoral neck (the “ball” that fits into the hip “socket”), although not at the hip itself. Estimates of bone strength improved, and less shrinkage occurred in the height of the thoracic spine (mid-back). Although the number of fractures was too small for statistical tests, six subjects in the placebo group but only one subject in the vitamin K group suffered vertebral fractures. This latter finding hints at a possibly very large reduction in the risk of fracture, but a larger study with sufficient numbers of fractures for statistical tests would be needed to confirm it. The benefits to bone health in this study did not occur until the third year. Most other trials have only been one year long. Thus, while the RCTs are not in perfect agreement, the data are consistent with a powerful effect of vitamin K that takes several years to manifest. Future studies should be larger, at least three years long, and compare different doses and forms of vitamin K in different contexts to improve our understanding of how to best take advantage of this vitamin for bone health. For now, the principle is sufficiently compelling to consider it likely over time that optimizing vitamin K intake is likely to provide meaningful benefits to bone health. Vitamin K is centrally important to oral health. The salivary glands contain the second highest concentration of vitamin K2 within the body (Thijssen, 1994), and both vitamin K2 (Glavind, 1948) and vitamin K-dependent proteins (Zacharski, 1979) are secreted into saliva. Dentin, the tissue underneath the enamel, produces both osteocalcin and MGP (Trueb, 2007). Between 1945 and 1946, two studies tested the ability of menadione-laced chewing gum to protect against dental cavities in humans (Burrill, 1945; Mäkilä, 1968). Menadione is a precursor to the MK-4 form of vitamin K2, but it also has direct antibacterial effects. One study showed it was effective but the second failed to replicate the findings and the topic was largely forgotten thereafter. At the time, researchers thought any effect of menadione would be a result of its antibacterial activity. A study published in the 1950s, however, found that menadione prevented tooth decay in hamsters more effectively when injected into their abdominal cavities than when given orally (Gebauer, 1955). While it’s possible that some of the abdominally injected menadione made it into the saliva where it would have direct antibacterial activity, a more likely interpretation is that the abdominally injected menadione protected against tooth decay through its conversion to vitamin K2. This conversion is variable between and even within species, and variation in the ability of humans to make the conversion could have contributed to the conflicting findings with menadione-laced chewing gum. While no studies have yet clearly shown dietary or supplemental vitamin K to improve dental health, this is most likely a result of the dental field largely ignoring any role for nutrition in the prevention of tooth decay beyond the role of carbohydrates in promoting bacterial acid production. The ubiquity of vitamin K and its proteins in the tissues of the mouth makes its importance clear, and what we need to move forward are clinical studies that take its role seriously. Human kidneys contain high concentrations of vitamin K2 (Thijssen, 1996) and use it to activate MGP . By the mid-1980s, we knew that a vitamin K-dependent protein isolated from patients with kidney stones, presumably MGP, was between four and twenty times less effective at preventing the growth of calcium oxalate crystals compared to the same protein isolated from healthy patients (Vermeer, 1986). Patients on renal dialysis have very high circulating levels of inactive MGP, and vitamin K2 supplementation dose-dependently improves its activation (Caluwé, 2014). Observational studies show that patients who consume more than the recommended intake of vitamin K spend less time on dialysis (Boxma, 2012) and have improved survival (Cheung, 2015). These results suggest that patients with kidney disease have very high needs for vitamin K, but it is unclear whether vitamin K deficiency is a primary contributor to the initial development of kidney disease and so far no clinical trials have shown that vitamin K supplementation can prevent, treat, or reverse the disease. Still, it seems promising that optimizing vitamin K status could be a valuable prophylactic and seems advisable for renal patients to, with medical supervision, supplement with doses shown to improve MGP activation. When used during pregnancy, vitamin K antagonists interfere with the growth of bone and cartilage in the fetus, especially the maxilla and nose, leading to underdevelopment of the middle third of the face (Howe, 1997). Growing children and adolescents likely have a high demand for vitamin K. In boys and girls between the ages of 10-14, fracture risk increases to such an extent that a 14-year-old boy has the same risk as a 53-year-old woman (Saggese, 2002). This is accompanied by very high levels of undercarboxylated osteocalcin, ranging from 11 to 83 percent of total osteocalcin (O’Connor, 2007; van Summeren, 2007; van Summeren, 2008). Whether improved intake of vitamin K can reverse the fracture risk or improve the rate of growth remains to be seen, but should be regarded as plausible. Vitamin K plays two known roles in metabolic and hormonal health: one is to support the function of osteocalcin, an endocrine hormone produced by bone tissue, and the other is to support the production of sex hormones through the regulation of gene expression. The role of osteocalcin is most clearly supported by osteocalcin knockout mice: they are obese and have low metabolic rates, high blood sugar, poor insulin sensitivity, deficient levels of insulin and males have low testosterone and infertility (Lee, 2007; Oury, 2011). The role of gene expression is most clearly supported by cellular experiments that have characterized the related mechanisms and by a study showing that vitamin K increases the expression of the enzyme that converts cholesterol to pregnenolone in rats (Ito, 2011). Pregnenolone is the precursor to all of the steroid hormones, including all of the sex hormones, and vitamin K’s support of pregnenolone synthesis increases testosterone in male rats. To date, the targets of vitamin K’s regulation of gene expression are poorly characterized and they may impact sex hormones beyond simply increasing pregnenolone synthesis. Direct evidence that vitamin K supports these roles in humans is limited, but there are key reasons to believe that it does. The sections below discuss the human evidence in the context of each specific health benefit. A rare genetic defect in what appears to be the osteocalcin receptor results in fasting hyperinsulinemia and postprandial glucose intolerance, suggesting that osteocalcin plays the same role in metabolic health in humans as it does in mice (Oury, 2013). As noted below, this genetic defect also results in low testosterone. Several randomized controlled trials have shown that 1 milligram of vitamin K1 (Rasehki, 2015 a; Rasehki, 2015 b) or 30-90 mg of vitamin K2 as MK-4 (Choi, 2011; Sakamoto, 2000) given daily for one to four weeks improves a variety of markers of glucose and insulin metabolism. From among these, the trial most relevant to nutritional doses of vitamin K (Rasheki, 2015 a; Rasheki, 2015 b) compared 1 mg/day of K1 to a placebo over four weeks and found that it lowered glucose and insulin levels postprandially (after a glucose tolerance test) but not in the fasting state. It also increased adiponectin, supporting the mechanism outlined in animal experiments whereby osteocalcin is released from bone and acts on adipose tissue to increase adiponectin, which then acts on other tissues such as muscle and liver to increase insulin sensitivity. As described in the section on different vitamin K forms below, while certain forms of vitamin K2 may more effectively reach bone than K1, K1 does reach bone in substantial amounts, and the dose used in the Rasehki study was high. No one has yet compared nutritional doses of K1 to other forms of vitamin K, but we could predict that the forms that reach bone most effectively, such as MK-7, could prove even more effective. The authors of these studies have generally argued that their results contradict the animal experiments rather than supporting them. The animal experiments show that osteocalcin has to be in its undercarboxylated state to improve metabolic and hormonal health, and these supplementation trials have shown what has already been well established, that vitamin K increases the carboxylated form and decreases the undercarboxylated form. However, the animal experiments provide a view that is much more nuanced than “undercarboxylated good, carboxylated bad.” Vitamin K is needed to “prime” osteocalcin by allowing it to accumulate in bone matrix; bone decarboxylates it and releases it in response to specific stimuli, one of which is exercise. Vitamin K deficiency causes a continuous, slow, unregulated leak of undercarboxylated osteocalcin into the blood. Supplying vitamin K to bone allows bone to properly store the hormone and release it at the right time. While we need to learn more about osteocalcin physiology to completely reconcile all of these findings, the evidence that both vitamin K and osteocalcin are critical to metabolic health is strong. A rare genetic defect in what appears to be the osteocalcin receptor results in low testosterone in men, suggesting that osteocalcin plays the same role in sex hormone production in humans as it does in mice (Oury, 2013). As noted above, this genetic defect also results in poor metabolic health. Evidence that vitamin K optimizes sex hormones in humans is limited, but a recent randomized controlled trial in women with polycystic ovarian syndrome (PCOS) provides intriguing results (Razavi, 2016). PCOS is a condition involving insulin resistance and high levels of androgens (hormones that should be high in males and low in females). Compared to a placebo, a cocktail of vitamin D (400 IU), calcium, (1000 mg), and vitamin K2 (180 μg, as MK-7) taken over the course of nine weeks cut the levels of androgens in half. This could have been a result of osteocalcin-mediated improvements in insulin sensitivity, gene expression-mediated improvements in sex hormone production, or some combination of these mechanisms. The use of a nutritional cocktail precludes a definitive conclusion about the effect of vitamin K itself or how it would act alone, but the possibility that vitamin K has such a powerful effect on sex hormone optimization is promising. Cell experiments suggest that the MK-4 subform of vitamin K2 protects against cancer through its regulation of gene expression (Shearer, 2014). In 2004, a randomized controlled trial provided an incredible demonstration of this effect in humans: in women with viral cirrhosis, supplementation with 45 miligrams per day of MK-4 reduced the risk of liver cancer by over 80 percent over the course of 8 years (Habu, 2004). Other trials have looked at the ability of the same exact treatment regimen to reduce the recurrence of liver cancer in people who had already recovered from it once. A meta-analysis examined five of these trials and found that vitamin K2 reduced the recurrence of liver cancer by 29-34% at two and three years (Riaz, 2012). These results are less dramatic than those of the 2004 paper, but the trials were much shorter. Even in the 2004 paper, the effect of K2 at 2-3 years was small and only became large in years four through eight of the study. Thus, it may be that this treatment is highly protective against liver cancer when carried out over a long enough duration. The dose of MK-4 used in these studies is hundreds of times what any of us could expect to get from food. Unfortunately, we don’t know if such a high dose was actually needed. In other words, perhaps the first 200 micrograms of that dose (the first 0.44%) got rid of 80 percent of the cancer and the rest of the dose did nothing. Alternatively, it could be that such high doses have pharmacological effects that amounts of MK-4 found in food do not have. In that case, obtaining vitamin K2 from food could be irrelevant to cancer. Observational studies offer some limited support for the importance of K2 from foods: the EPIC-Heidelberg study found that German men who consumed more than 46 micrograms per day of K2 were almost two-thirds less likely to develop advanced prostate cancer and lung cancer as those consuming less than 26 micrograms per day (Nimptsch, 2008; Nimptsch, 2010). Thus, data from cell experiments, observational studies, and randomized controlled trials agree that vitamin K2 protects against cancer, but differences in the doses used and the types of cancer investigated leaves many open questions to be investigated by future research. Click here to close the detailed explanation.The Biochemistry Underlying the Health Benefits of Vitamin K2
Vitamin K-dependent 𝛄-Carboxylation
The Role of Vitamin K in Blood Clotting
The Role of Osteocalcin in Metabolic and Hormonal Health
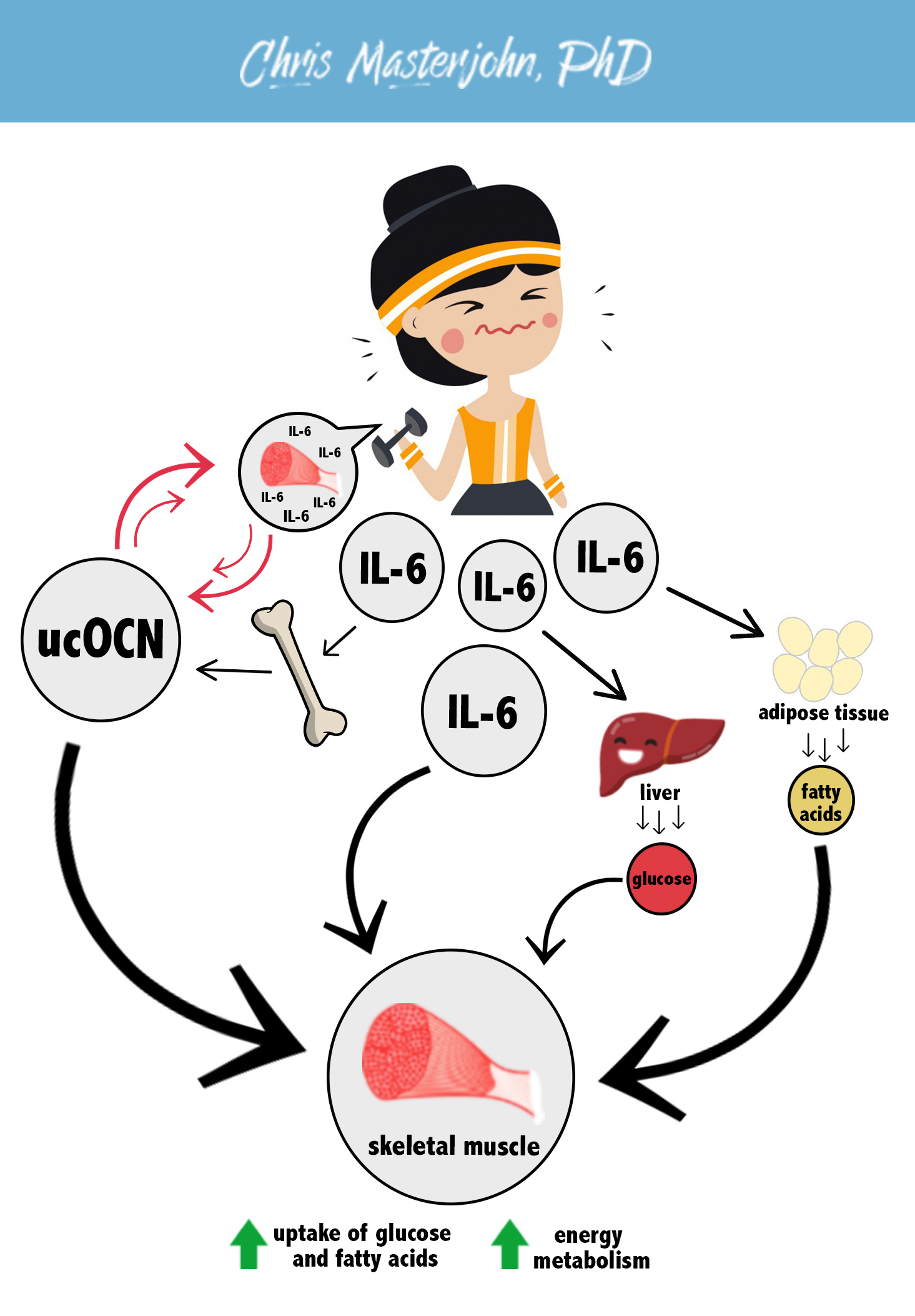
Most recently, the release of undercarboxylated osteocalcin from bone was shown to increase during exercise and play a role in allowing skeletal muscle to increase its utilization of energy (Mera, 2016). Exercising skeletal muscle secretes interleukin-6 (IL-6), which increases the release of undercarboxylated osteocalcin (ucOCN) from bone. ucOCN stimulates muscle to release more IL-6, and they amplify one another in a positive feedback loop. IL-6 acts on liver to release glucose and adipose tissue to release free fatty acids. IL-6 and ucOCN act on skeletal muscle to increase the uptake of glucose and fatty acids and increase their utilization for energy. This is illustrated in the figure below.
Matrix Gla Protein (MGP) Regulation of Calcium Distribution

MK-4 and Gene Expression
Other Functions of Vitamin K
Evidence For the Health Benefits Of Vitamin K2
Evidence for the Role of Vitamin K in Blood Clotting
Evidence for the Role of Vitamin K in Controlling Calcium Distribution
Evidence for the Role of Vitamin K in Heart Health
Evidence for the Role of Vitamin K in Bone Health
Evidence for the Role of Vitamin K in Dental Health
Evidence for the Role of Vitamin K in Kidney Health
Evidence for the Role of Vitamin K in Growth
Evidence for the Role of Vitamin K in Metabolic and Hormonal Health
Evidence for the Role of Vitamin K in Metabolic Health
Evidence for the Role of Vitamin K in Sex Hormone Optimization
Evidence for the Role of Vitamin K in Cancer
Why the Form of Vitamin K You Eat Is So Important
Vitamin K comes in different forms. Vitamin K1 is primarily found in plant foods and is most abundant in leafy greens. Vitamin K2 is only found in animal foods and fermented plant foods. The term “vitamin K2 ” actually refers to a collection of more specific forms known as menaquinones that are all abbreviated “MK” with a specific number attached: for example, MK-4, MK-7, MK-10, and so on.
Does it matter whether you eat one form or another? Absolutely. There are two reasons for this, so let’s deal with them one at a time.
First, once we eat foods with vitamin K in them, our bodies handle the different forms differently. Consider these examples:
-
- Vitamin K1 travels to our livers more effectively than it does to our bones or blood vessels. The liver is where we use vitamin K to make the proteins involved in blood clotting, so vitamin K1 is better at supporting blood clotting than it is at providing other health benefits.
- MK-7 is much more effective than K1 at reaching bone. This doesn’t just make it good for bones: our bones use vitamin K to produce a hormone known as osteocalcin, which improves metabolic and hormonal health and increases exercise performance. Thus, MK-7 better supports these health benefits than K1 . The portion of MK-7 that reaches the liver, moreover, stays active in the liver much longer than K1 before being broken down; as a result, MK-7 is even better than K1 at supporting blood clotting.
- MK-4 is taken up by our tissues very rapidly after we consume it. While it hasn’t been studied as carefully as MK-7, it may be less effective than MK-7 at reaching liver and bone but more effective at reaching most other tissues. This would make it better at protecting those tissues from calcium deposits and cancer development and supporting sex hormone production through its direct actions within our sex organs.
Overall, then, the collection of different vitamin K2 compounds better supports all the health benefits listed above than vitamin K1 because they better reach the tissues that matter.
These concepts are illustrated in the shareable infographic below.

The second reason the form of vitamin K matters is that MK-4 regulates gene expression in specific ways that no other form of vitamin K does. While we tend to think of our genes as the destiny we inherited from our parents, it’s actually how they are expressed — meaning, what our cells do with the information carried by those genes — that determines our health. MK-4 turns on some genes and turns others off. For example, in our sex organs, it turns on the genes involved in sex hormone production. In a wide variety of cells, it turns on the genes that keep cells healthy and turns off the genes that make cells become cancerous. Thus, MK-4 plays an exclusive role in cancer protection and sexual health.
This special role of MK-4 probably explains why all animals break down other forms of vitamin K and convert them to MK-4. By contrast, no animal synthesizes any other form of vitamin K. This explains why MK-4 is mostly found in animal foods, and why most unfermented animal foods contain little if any of the other forms.
As humans, we also convert other forms of vitamin K to MK-4. This raises the question, do we really need to consume MK-4 directly if we can make it ourselves? My answer is yes.
There are three reasons we shouldn’t rely on the conversion:
- First, we don’t actually know that much about how the conversion takes place, but it seems to be inefficient and highly variable according to genetics and health status, making it unreliable.
- Second, cholesterol-lowering statin drugs and certain osteoporosis drugs inhibit the conversion, making it even less reliable in people who are taking these drugs.
- Third, research shows vitamin K2 is better than vitamin K1 at supporting many different aspects of our health. If we easily converted as much K1 to K2 as we needed, we wouldn’t observe these superior benefits of K2.
These concepts are illustrated in the shareable infographic below.

The difference between K1 and K2 isn’t absolute. When we eat vitamin K1 some of it will reach tissues outside the liver and we will convert some of it to MK-4. But the real question is: what’s the best vitamin for the job? Vitamin K2 is clearly much better at supporting the health benefits discussed in this resource, so the resource is dedicated specifically to getting enough K2 in its diversity of forms.
The Many Forms of Vitamin K
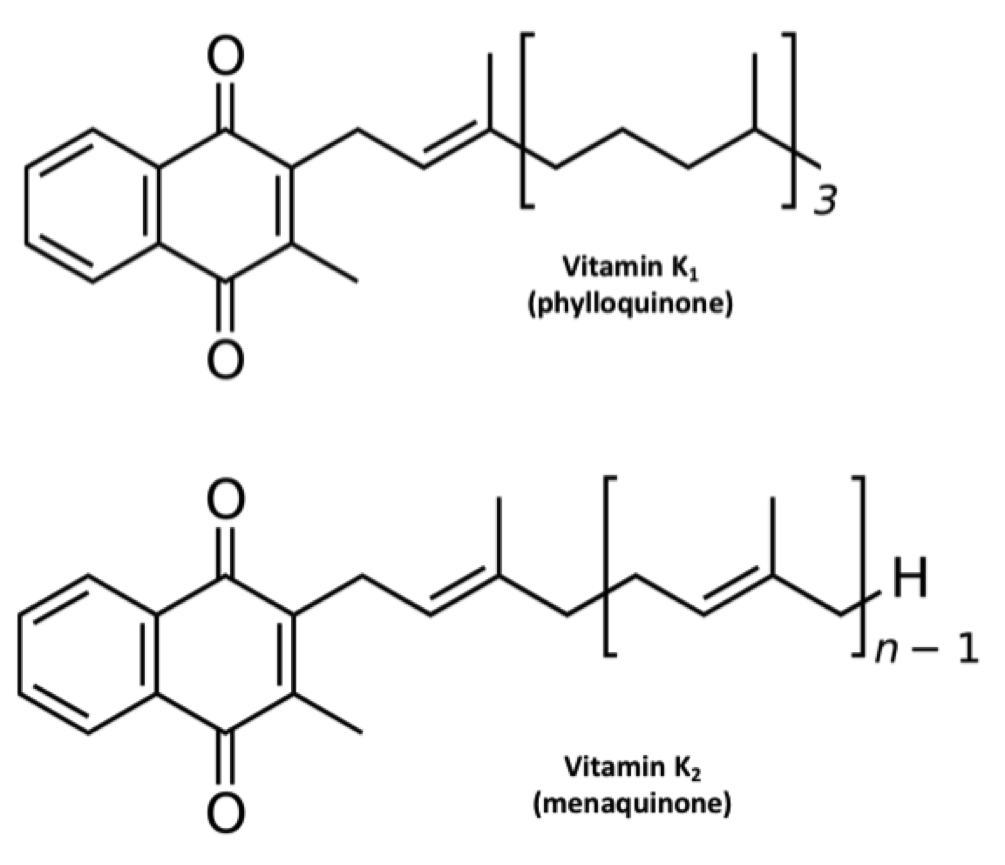
The names “vitamin K1” and “vitamin K2” are artifacts of history (Suttie, 2014). The first form of vitamin K was found in alfalfa, so it was named K1. The second form was found in rotten fish, so it was named K2. As shown in the figure below, they both have the same ring structure, but different tail structures. The tail structures are known formally as side chains. Vitamin K1, now known as phylloquinone, has a mostly saturated tail. Vitamin K2, now known as menaquinone, has an unsaturated tail. Menaquinones are actually a class of compounds with varying tail lengths, designated MK-n, where “n” indicates the number of repeating units in the tail. The specific form of vitamin K2 found in rotten fish was MK-7. When later MKs were discovered, they all had unsaturated tails, so scientists classified them as subforms of vitamin K2.
We now know that this is overly simplistic (Shearer, 2014). Some bacteria, such as those used to make Jarlsberg cheese, produce partially saturated menaquinones wherein some of the repeating subunits have double bonds and others don’t. For example, Jarlsberg is very rich in tetrahydromenaquinone-9, which is similar in structure to MK-9 except the second and third units of the tail are saturated. As Shearer (2014) pointed out, even phylloquinone has a double bond in the first unit of its tail and could be seen as a partially saturated form of MK-4. Thus, rather than forming two categories of K vitamins, it makes more sense to say that vitamin K comes in a wide diversity of forms that are distinguished by the length and saturation of their tails.
Side Chain Length and Saturation Determines Tissue Distribution
While the ring structure is what allows vitamin K to support the vitamin K carboxylase, the enzyme that activates vitamin K-dependent proteins, the tail structure determines how different forms of vitamin K reach different tissues in the body. This all begins with how they are incorporated into lipoproteins soon after we absorb them from food.
When we digest fat and fat-soluble nutrients, our intestines package them into lipoproteins known as chylomicrons, which take them through the lymph and into the bloodstream. This event critically distinguishes how water-soluble and fat-soluble nutrients are distributed through the body: water-soluble nutrients travel directly to the liver through the portal vein, while fat-soluble nutrients travel through the lymph in chylomicrons to bypass the liver and nourish the other tissues first.
Chylomicrons, like all other lipoproteins, have to transport fat-soluble things through the water-based environment of the blood. Therefore, they are fat-soluble on the inside and water-soluble on the outside.
While all K vitamins are fat-soluble, they are not all equally soluble in fat. Those with longer tails are more fat-soluble than those with shorter tails; for tails of equal length, saturated tails are more fat-soluble than unsaturated tails. K vitamins that are more fat-soluble are carried deeper in the core of chylomicrons, while those that are less fat-soluble are carried more toward the edges. Let’s take the three forms most commonly found in supplements as examples: K1, MK-4, and MK-7. We would expect to find MK-7 in the center of the chylomicron, MK-4 closer to the edges, and K1 in between the two (Schurgers and Vermeer, 2002).
Chylomicrons move in and out of the bloodstream rapidly, with a half-life of 15-20 minutes (César, 2006). This means that once we eat a meal, 95% of the chylomicrons that enter our blood are fully cleared in the first hour. Very few tissues actually take up the whole chylomicron. Instead, most tissues use the enzyme lipoprotein lipase (LPL) to siphon off its nutrients bit by bit. While LPL is best known for feeding the heart, skeletal muscle, and adipose tissue, it also feeds other tissues such as the lungs, kidneys, mammary glands, and brain (Kersten, 2014). LPL spreads across the capillary beds that feed our great diversity of tissues, allowing widespread access to the fat-soluble nutrients we ingest in a meal. Presumably, these tissues all have greater access to the nutrients carried closer to the edges of the chylomicrons, such as MK-4.
As these many tissues feast on the chylomicrons, the chylomicrons get smaller and smaller until they become chylomicron remnants. A small handful of tissues donate apolipoprotein E (ApoE) to the chylomicron remnants, and then use the LDL receptor and other related receptors to bind to the ApoE and take up the whole remnant. This allows them to score everything left in the particle right down to its chewy center. In this sense, ApoE is like the bait on a fishing line, and the receptor is like the hook. While the liver is best known for fishing out chylomicron remnants in this manner, our bones and spleen do as well. Our bones primarily derive nutrients through the uptake of whole lipoprotein particles, and take up about a fifth as many chylomicron remnants as our liver (Shearer, 2008). Thus, we should expect bone and liver to primarily have access to nutrients carried in the center of chylomicrons, including K1, but especially the MKs with longer tails, such as MK-7.
This whole stream of events takes place largely in the first hour after a meal. The liver then repackages the lipids it took in from chylomicron remnants into other lipoproteins, primarily VLDL, which are sent back out into the blood. Tissues continue to siphon off nutrients using LPL. Just like chylomicrons had been digested into chylomicron remnants, VLDL particles are then digested into LDL particles until our tissues take up the LDL particles themselves. Unlike the rapid clearance of chylomicrons, clearance of LDL particles takes place slowly over the course of two weeks (Langer, 1972). Although the liver is the main tissue that takes up LDL, bone is also important; in fact, bone takes up vitamin K more effectively from LDL than from any other lipoprotein (Shearer, 2012). Thus, K vitamins that get packaged into LDL particles will have a second opportunity to nourish bone.
Schurgers and Vermeer (2002) investigated how different K vitamins are transported using K1, MK-4, and MK-9. They fed six healthy males a mixture of one milligram of each form and took repeated blood measurements over four days, beginning at the two-hour mark. MK-4 had already peaked by the time the first blood draw was taken, when much of it was found in HDL, and disappeared most rapidly from the blood out of all the forms. K1 peaked at the four-hour mark, was mostly gone by eight hours, and disappeared by the end of the study. K1 was found almost exclusively in VLDL rather than in LDL or HDL. MK-9 peaked at the four-hour mark as well, but persisted in the blood for several days while carried in LDL particles.
The authors suggested that MK-4 was taken up so quickly because it was carried toward the edges of the chylomicrons, making it easily accessible for LPL-mediated extraction, with the excess spilling over into HDL particles. Notably, we should expect the extended circulation of MK-9 in LDL to provide better nourishment to bone.
Schurgers later collaborated with Sato (2012) to compare the bioavailability of MK-4 and MK-7 in healthy women. Compared to the 2002 study, they used less than half the dose of each vitamin and fed them separately rather than combined so that the total dose of vitamin K given at each point was over six times lower. Similar to the 2002 study, they took their first blood sample at two hours. They didn’t find MK-4 in the blood at any time point, whereas MK-7 remained elevated for two days.
MK-4 vs. MK-7: What Do We Really Know?
If we compare the results of the 2012 study to the earlier 2002 study, we can surmise that the dose of MK-4 in the 2012 study was low enough that the initial LPL feast in the first hour fully distributed it to a variety of tissues so that it was all gone by two hours, and that MK-7 circulated for such a long time because, like MK-9, it was redistributed in LDL particles. We should expect from this that MK-4 is good at nourishing most tissues, but not very good at nourishing liver or bone. By contrast, we should expect that MK-7 is good at nourishing the liver and even better at nourishing bone.
At the present time, there is no direct support for this, but there are hints that it may be the case. Sato (2012) cited a Japanese paper as finding that 1.5 milligrams of MK-4, but not 500 μg, improved the carboxylation of osteocalcin. Not even the abstract seems to be available in English, so it is difficult to evaluate the study. Later, Nakamura (2014) showed that only 600 μg of MK-4 is needed, but in this study the researchers simply gave the same people higher and higher doses each week and waited for osteocalcin carboxylation to improve. For all we know, their lowest dose, 300 μg, would have worked if they had given it longer than a week. In seeming contrast to MK-4, MK-7 improves osteocalcin carboxylation with as little as 100 μg (Knapen, 2012; Inaba, 2015).
Placing these studies side by side, they seem to suggest that improvements in osteocalcin carboxylation require much lower doses of MK-7 than of MK-4. However, the studies had different designs and were conducted in different populations that may have had different nutritional needs and different responses to vitamin K supplementation. In fact, Inaba (2015) fed MK-7 for four weeks while Nakamura (2014) only fed each dose of MK-4 for one week. This alone could explain the difference. To date, no one has compared the osteocalcin response to MK-4 and MK-7 head-to-head.
On the other hand, MK-7 has been compared to K1. At equal doses, MK-7 is three times more potent than K1 at carboxylating osteocalcin (Schurgers, 2007). Osteocalcin is made in bone, so its carboxylation reflects vitamin K status in that tissue. Presumably, MK-7 is better than K1 because its recirculation in LDL particles for days after it is first taken up by the liver gives it much more opportunity to nourish bone. Since MK-4 likely has even less opportunity to reach bone than K1, MK-7 is probably superior to MK-4 for this purpose as well.
What about other tissues? Unfortunately, we know even less about those. We know that large pharmacological doses of MK-4 given to rats (Konishi, 1973) or dogs (Sano, 1997) reach the lungs, liver, kidney, pancreas, spleen, adrenal gland, and bone very rapidly. Such large doses are also excreted into the feces in large amounts. More moderate nutritional doses could behave very differently, however, so it is difficult to form any conclusions from these studies. Until we have well designed trials comparing the ability of different MKs to support different health outcomes in humans, it makes sense to rely on what we know generally about how lipoproteins transport nutrients. This suggests K1 would best reach the liver, MKs 7-9 would best reach liver and bone, and MK-4 would best reach most other tissues.
MK-7 Supports Blood Clotting Better Than K1
MK-7 is not just three times better than K1 at reaching bone; it’s also five times better at supporting blood clotting (Schurgers, 2007). This may be because the greater fat-solubility of MK-7 makes it hold on more tightly to the membranes within liver cells, making it stay active in the liver much longer rather than being released and broken down (Shearer, 2008). The liver is where clotting proteins are made, so more extended activity in the liver would explain why MK-7 could better support blood clotting. If this is correct, other long-chain MKs such as MK-8 and MK-9 probably share this property as well.
MK-4 Plays a Unique Role in Gene Expression
MK-4 is unique among the K vitamins in its regulation of gene expression. It increases the expression of genes that regulate cell growth in osteoblasts (the cells responsible for bone growth), but MK-7 and K1 do not (Ichikawa, 2007). MK-4 increases testosterone production when fed to male rats. Cellular experiments show that MK-4, but not K1, increases testosterone by increasing the expression of the enzyme that converts cholesterol to pregnenolone, which is the first step in sex hormone synthesis (Ito, 2011).
MK-4 also inhibits the growth of various cancers of the liver, gut, and bone (Shearer, 2008). Remarkably, the gene that is now known to code for the enzyme that converts other K vitamins to MK-4, Ubiad1, was known years earlier as a tumor-suppressor gene (Shearer, 2014). Scientists observed that Ubiad1 was often silenced in tumors of the bladder, prostate, and kidney. Conversely, experimental overexpression of Ubiad1 inhibited the growth of prostate cancer cells. Since the enzyme that Ubiad1 codes for converts other K vitamins to MK-4, these results underscore that the anticancer properties of vitamin K belong specifically to MK-4.
Can We Rely on the Conversion of Other K Vitamins to MK-4?
When we consume any form of vitamin K, our intestinal cells break the side chains off of a small portion to yield the pure ring structure, known as menadione (Thijssen, 2006). Menadione then disperses through the body to many tissues that convert it to MK-4 for their own use by adding MK-4’s characteristic four-unit unsaturated side chain (Hirota, 2013).
We have known that animals synthesize MK-4 from other K vitamins for over a half century. It has been clear throughout that time, however, that the conversion varies widely. Early experiments, for example, showed that birds made the conversion better than rats and pigeons made it better than other birds (Billeter, 1960). Among rats, Wistar rats (Thijssen, 1994) seem to make the conversion better than Lewis rats (Ronden, 1998). Since the conversion varies between and within species, we should not assume that we as humans can make the conversion efficiently and consistently enough to meet our needs.
And just how good are we at this conversion? We really don’t know, but it stands to reason that it varies from person to person. Rare genetic defects in Ubiad1 have been identified (Yellore, 2007), and cancer is associated with epigenetic silencing of Ubiad1 (Woolston, 2015). Other genes involved in the conversion likely vary from person to person as well, but we don’t yet know what they are. One of them may be vitamin K epoxide oxidoreductase (VKOR), the target of warfarin. The normal role of VKOR is to reduce vitamin K that has been oxidized, and we know that menadione must be in a reduced state to undergo conversion to MK-4. Indeed, warfarin prevents the conversion of K1 to MK-4 in rats (Spronk, 2003). Genetic polymorphisms in VKOR are common (Shearer, 2012), and could hypothetically contribute to variation in MK-4 synthesis. We still do not know what enzyme is responsible for cleaving the side chain within our intestinal cells, and that could be polymorphic as well.
However good or bad humans may naturally be at the conversion, many people are taking medications that inhibit it (Hirota, 2015). Lipophilic statins such as lovastatin and simvastatin (and presumably atorvastatin, branded as Lipitor) inhibit the conversion. So do nitrogen-containing bisphosphonates such as alendronate (Fosamax) and zolendronate (Zometa), and presumably other nitrogenous bisphosphates as well. Ubiad1 expression depends on zinc (Funahashi, 2015) and its enzymatic activity depends on magnesium (Hirota, 2015), suggesting that deficiencies of either of these minerals could also compromise the conversion.
Finally, if we converted other K vitamins to MK-4 on a “however much we need to” basis, then it shouldn’t matter what type of vitamin K we consume at all. All forms of vitamin K generate some menadione in the intestine that can be converted to MK-4 in other tissues. Whether the menadione comes from K1, MK-4, MK-7, or any other form of vitamin K cannot make any difference in its tissue distribution. Humans accumulate MK-4 in multiple organs including the heart, lung, brain, liver, kidney, and pancreas (Thijssen, 1996). Thus, if there are no major limitations on the conversion besides our need for it, K1 should be perfectly capable of supplying these tissues with all the MK-4 they need, especially in populations that have high K1 intakes. Yet this does not seem to be what we find.
Consider the Dutch population, where this has been investigated most extensively. K1 intakes are eight times higher than K2 intakes, yet only K2 intake is inversely correlated with heart disease (Geleijnse, 2004; Gast, 2009; Buelens, 2009; Zwakenberg, 2016). In Germany, K1 intakes are about three times higher than K2 intakes, yet only K2 intake is inversely correlated with advanced prostate cancer (Nimptsch, 2008) and lung cancer (Nimptsch, 2010).
These observational studies don’t offer clear evidence of cause-and-effect relationships and they don’t show correlations with health endpoints that are specific to MK-4. However, they do add to the list of reasons to believe that our ability to synthesize MK-4 is limited by much more than our specific need for MK-4 itself, and by much more than our general need for vitamin K in the tissues that unconverted K1 has a hard time reaching. In other words, many of us probably need more MK-4 than we can make on our own, and that’s a good reason to eat foods that provide it.
Altogether, the evidence suggests that the form of vitamin K we consume matters, and that we are best served by a diversity of K vitamins from leafy greens, animal foods, and fermented foods.
Click here to close the detailed explanation.
How Much Vitamin K2 Do We Need?
Currently, there are no official recommendations about vitamin K2. In the United States, the current recommendation for total vitamin K is 90 μg per day for adults. In a typical diet, most of this would come from K2. These recommendations were last updated in 2001, before we learned about most of the benefits of K2. In fact, the USDA did not even develop a database of vitamin K2 in foods until 2006. My recommendation, therefore, does not rely on official sources and is meant for health-conscious people who wish to take advantage of cutting-edge research.
Based on the current state of that research, I recommend 100-200 μg per day of vitamin K2 for healthy adults. Although most of the benefit probably comes from the first 100 μg, 200 μg is harmless and may provide additional benefit. If your health is fantastic while maintaining a K2intake close to 100 μg, I would not worry about increasing your intake. But if you could stand to gain from the wide array of health benefits provided by the vitamin, I would use food or supplements to bring your intake closer to 200 μg.
Patients with chronic kidney disease may require doses as high as 480 μg per day and possibly much higher, but the use of high doses to treat a disease should always be done under medical supervision.
Patients using warfarin (Coumadin) or any other anticoagulant medications related to it should not make any changes to their vitamin K intake, regardless of the specific form of vitamin K, whether from food or supplements, except under the strict supervision of the prescribing physician (see below).
Vitamin K2: What is the Optimal Dose?
Another way to ask this question is as follows: what is the minimum effective dose to achieve the maximal desired effect? While there is no established toxicity for high doses, there are good reasons to be cautious before taking far more than we need (see below), hence the term “minimum effective dose.” At the same time, we don’t want to reap just some of the health benefit. We want to reap as much of the health benefit as we can in a safe and effective manner, hence the term “maximal desired effect.”
The only rigorous way to approach this is to look at dose-finding studies, which are studies where different doses were directly compared with one another. Ideally, the studies are randomized, controlled, long enough in duration to believe the dose was able to achieve its full effect, and conducted within a context where we would expect to see a benefit.
Pharmacological Doses of MK-4
A Japanese dose-finding study compared 15, 45, 90, and 135 milligrams per day (mg/d) of MK-4 to reduce fracture risk in postmenopausal women with osteoporosis and found 45 mg/d to be the minimal effective dose (Iwamoto, 2013). This is a pharmacological dose that is hundreds of times greater than what can be obtained from food. It probably works through mechanisms that are independent of the those seen for nutritional doses of vitamin K, such as overriding the body’s natural regulation of bone resorption. Thus, we should view MK-4 at these doses with the same type of cost-benefit analysis we would use for other osteoporosis drugs, like Fosamax, and we should not use these studies to determine the optimal nutritional dose of MK-4.
Nutritional Doses of MK-4
Unfortunately, there is a dearth of dose-response studies for nutritional doses of MK-4. Nakamura (2014) compared the effect of 0, 300, 600, 900, and 1500 micrograms per day (μg/d) on osteocalcin carboxylation, a marker of vitamin K status in bone. They fed everyone the same doses in the same order, increasing the dose from 0 one week at a time. The carboxylation status did not change with 300 μg/d, but improved with 600 μg/d. However, it is not at all clear that 300 μg/d would not have provided the same benefit if given for longer than one week. I do not consider this study to offer any clear insight about the optimal dose of MK-4.
MK-7 in Healthy Populations
Dalmeijer (2012) compared 180 and 360 μg/d MK-7 to a placebo given to healthy, non-obese men and postmenopausal women aged 40-65 years over the course of twelve weeks. The mean K2 intake from food was 25 μg/d, so these treatments effectively compared total K2 intakes of 25, 200, and 380 μg/d. Both treatment doses lowered desphospho-uncarboxylated MGP (dp-ucMGP), a marker of vitamin K deficiency in blood vessels, and improved the carboxylation status of osteocalcin. While 360 μg seemed to cause a slightly larger effect than 180 μg, the lion’s share of benefit came from 180 μg and the difference between the two doses was not statistically significant. Thus, the study hints at a possible benefit of doses higher than 200 μg that would have to be confirmed in future studies with greater statistical power, but provides rigorous evidence only that 200 μg is better than 25 μg.
Knapen (2012) reported a more extensive array of doses given to healthy men and premenopausal women aged 25-45 over the course of twelve weeks. The doses included 0, 10, 20, 45, 90, 180, and 360 μg/d MK-7 and the primary endpoint of interest reported was the carboxylation status of osteocalcin. Unfortunately, the sample size (n=42) was small for having so many groups, precluding a rigorous statistical analysis of the endpoints between each group. Additionally, while carboxylated osteocalcin levels were similar across groups at baseline, undercarboxylated osteocalcin levels were highly variable. The changes in undercarboxylated osteocalcin between baseline and the study’s end within any given group were generally about the same size as the difference in baseline values between groups. All of this makes it extremely difficult to know whether the the difference between groups for changes in undercarboxylated osteocalcin or its ratio to total osteocalcin are true biological differences or simply random variation resulting from noisy data.
Doses that were 90 μg/d or greater caused statistically significant decreases in undercarboxylated osteocalcin, but only the 180 μg and 360 μg doses increased the levels of carboxylated osteocalcin or improved the ratio. From among these measurements, the increase in carboxylated osteocalcin seen with the two higher doses is most convincing because the variation in baseline values for that measurement was so low. The ending values for this measurement were higher in the 180 and 360 μg groups than in any of the the others, but they were nearly identical between groups. K2 intake from food was not reported, but presumably would have added at least 20 μg/d to the doses. I therefore consider this study to offer limited support to 200 μg/d as the optimum dose for improving vitamin K status at bone.
Inaba (2015) compared 0, 50, 100, and 200μg/d MK-7 in postmenopausal women aged 50 to 69 years over the course of four weeks. The primary endpoint of interest was the carboxylation status of osteocalcin, reported as the ratio of the carboxylated to the undercarboxylated form. The study was conducted in Hokkaido, Japan, where natto is popular. The subjects were required to avoid all MK-7-rich foods and to consume prepared meals that provided 65 μg/d of total vitamin K as a combination of K1 and MK-4 in unspecified proportions. Whether intentional or not, this is effectively a study of how much MK-7 you need to preserve the carboxylation status of your osteocalcin when you stop eating natto. Indeed, the largest effect across all groups was for carboxylation status to significantly worsen in the 0 μg/d group. Carboxylation status was significantly different from that group in the 100 and 200 μg/d groups, but not in the 50 μg/d group. The authors did not report a statistical analysis for the difference between 100 and 200 μgd, but 200 μg/d was the only group in which carboxylation status actually improved over the course of the study. I therefore consider this study to offer limited support to 200 μg/d as the optimum dose for improving vitamin K status at bone.
In further support of this conclusion, Ikeda (2006) found that postmenopasual women who reported consuming enough natto to provide 200 μg/d K2 or more (mostly as mostly MK-7) suffered less bone loss over the course of three years than women who consumed less. Since all lower intakes of natto were grouped together for the statistical analysis, it is not clear exactly where the line of maximal benefit lies, and it may be less than 200 μg/d. As an observational study, we should also be more cautious about inferring cause and effect. Nevertheless, the fact that it measured an actual health endpoint (bone loss) instead of just a surrogate marker (osteocalcin carboxylation), and the fact that it was three years long instead of four to twelve weeks, makes it very worthy of consideration.
MK-7 in Hemodialysis Patients
Westenfeld (2012) and Caluwé (2014) both conducted dose-finding studies in hemodialysis patients. Patients with kidney disease have high levels of vascular calcification, which is a major contributor to mortality in this population. Since MGP protects blood vessels from calcification, dp-ucMGP was the major endpoint in both studies. Lower dp-ucMGP suggests better vitamin K status in blood vessels and a better defense against pathological calcification.
Westenfeld compared 45, 135, and 360 μg/d MK-7 over six weeks. MK-7 dose-dependently decreased dc-ucMGP, with the effect almost doubling in size for each increase in the dose from 18% to 37% to 61%. However, change from baseline analysis is vulnerable to regression to the mean and it is more rigorous to compare the absolute levels of dc-ucMGP after treatment. When looked at this way, 135 and 360 μg/d had equal benefit over 45 μg/d.
Nevertheless, Caluwé later tested even higher doses and provided evidence of benefit for more than 300 μg/d. They fed the patients 360, 720, or 1080 μg MK-7 three times per week for eight weeks, which equates to average daily doses of 154, 309, and 463 μg. MK-7 dose-dependently decreased dp-ucMGP by 17%, 33%, and 46%. The ending dp-ucMGP values were lower in the 463 μg/d group than in the 309 μg/d group and were lower than Westenfeld found after feeding 360 μg/d, but they were still about four times higher than that found in healthy controls. The average K2 intakes in the Caluwé paper were 16 μg/d, making the doses compared effectively 325 and and 479 μg/d. Future studies may clarify whether even higher doses can bring dp-ucMGP levels even closer to those found in healthy controls. Thus, there is strong evidence that the K2 requirement for kidney patients is higher than 325 μg, possibly as high as 480 μg, and may well be much higher than that.
Conclusions
For healthy populations, there is no smoking gun, but several studies converge towards the conclusion that 200 μg/d is the optimal dose. Most of the benefit probably comes from the first 100 μg, and the evidence for the superiority of 200 μg is limited. There may be benefits to higher doses, but there is no convincing evidence of that at this time. Thus, there is a high likelihood that I will revise my recommendation as new data comes in, but I currently recommend at least 100 μg/d and preferably 200 μg/d.
For kidney disease patients, there is good reason to see 480 μg/d as better than lower doses. Since 480 μg/d almost slashes dp-ucMGP in half yet leaves it four times higher than in healthy controls, the optimal dose may well be much higher than this. I suspect it is at least 1 mg/d. Nevertheless, K2 should only be used to augment treatment for kidney disease under medical supervision.
Click here to close the detailed explanation.
How to Get Enough Vitamin K2 From Food
You can use the searchable database we created to determine how much vitamin K2 is in your diet. In this section, I describe a few of the simplest ways to get 200 μg per day of K2 from foods. As noted above, most of the benefit comes from the first 100 μg, so any of the values below can be cut in half to obtain that amount.
The foods that are richest in K2 are natto and goose liver, both of which may be difficult-to-acquire tastes. Natto is a fermented soy food popular in eastern Japan. The source of K2 is the bacteria used in the fermentation, not the soy beans. As a result, any vegetable fermented with natto bacteria should be rich in K2. For example, 100 grams of traditional natto contains just under 950 μg, while 100 grams of natto made from black beans contains almost 800 μg. The value for black bean natto is a little lower than that for traditional natto, but both values are phenomenally high. Simply adding 18 grams of natto (about two-thirds of an ounce) to your diet each day would give you 200 μg, and just two ounces of goose liver would provide the same benefit.
Another excellent source of vitamin K2 is cheese. The K2 content of cheese varies widely according to the type of bacteria used to make it. To browse a full list of cheeses, search “cheese” in our database or leave the search box blank and select the category “Dairy Foods and Eggs.”
Jarlsberg cheese, which originates from Norway, is richest in K2. According to the value listed in our database, it would take nine ounces of Jarlsberg to provide 200 μg. Its true content of K2 has likely been underestimated, however, and it may actually take as little as 4.5 ounces.
Egg yolks and the dark meat (legs and thighs) of chicken are also good sources. For example, four whole eggs provides over 20 μg and 100 grams of dark chicken meat provides 60 μg.
Ultimately, it is the way these foods are combined in your diet that determines how much K2 you get. The first infographic provides some ideas of how to work these different foods into a meal to make a meaningful contribution to your daily K2 intake. You can figure out how much K2 other meals would provide by using our database.
Surprisingly, we recently learned that pork products are very high in MK-10 and MK-11. This is a newly discovered exception to the rule that fresh animal products mostly contain MK-4. Unfortunately, little is known about the bioavailability of these forms and there are some indications that we as humans largely store them in our livers rather than distributing them throughout our bodies like other forms of K2. However, if future research were to show that MK-10 and MK-11 have similar benefits as the other forms, that would mean most pork products are competitive sources. For example, only 4.5 ounces of baby back pork ribs would be needed to provide 200 μg, and just two ounces of pork sausage would provide the same amount.
Food quality is important. Egg yolk from The Netherlands is reported to have twice as much K2 as egg yolk from the United States. The reasons for this are unclear, but it may relate to the ways the chickens were raised. Wherever possible, I recommend using meat, eggs, and dairy from animals raised on pasture. For egg yolks, look for the most deeply colored yolks you can find.
Vitamin K2 in Foods: A Closer Look
Vitamin K2 in foods comes either from the conversion of other K vitamins to MK-4 in animals or from bacterial production of various MKs. A good example that ties these concepts together is cheese. A cow eats grass that contains K1. The cow converts a portion of that K1 to MK-4. Both K1 and MK-4 are found in the milk. Humans take the milk and ferment it into cheese. During the fermentation process, bacteria proliferate that synthesize a variety of MKs, mainly MK-7 through MK-10, and especially MK-8 and MK-9.
A comparison of different cheeses illustrates the importance of the specific type of bacteria used in the fermentation. For example, in each 100 gram serving, Jarlsberg contains 74 μg while blue cheese contains 36, cheddar contains 21, Swiss contains 8, and mozzarella only contains 4. This variation can also be seen among fermented plant foods. For example, sauerkraut has only 5 μg, compared to nearly 1000 for natto.
Within a particular type of cheese, ripening has little effect. For example, gamalost increases from 38 to 51 in the first ten days of ripening, but this level remains mostly stable over the course of 20, 30, and 60 days. This is probably because the bacteria that produced the K2 during the initial stage of fermentation die off during the ripening (Hojo, 2007).
The data for cheese also provide a window into the possibility that some of our current food data are gross underestimates. For example, most cheeses are made with lactic acid bacteria that produce mostly MK-8 and MK-9, but some cheeses are made with proprionibacteria that also produce tetrahydro-MK-9 (Hojo, 2007), which has a structure that is the same as MK-9 except it lacks some double bonds in its side chain. These include the Swiss cheeses Emmental and Gruyère, the French cheese Comté, and the Norwegian cheese Jarlsberg. Whether tetrahydro-MKs might be present in other foods is somewhat unclear because virtually all analyses of vitamin K in foods have ignored them. No analysis has yet evaluated both tetrahydro-MKs and all the regular MKs in any food at the same time, strongly suggesting that the total K2 in foods that contain tetrahydro-MKs is grossly underestimated. To take Jarlsberg as an example, Hojo (2007) showed that, per 100 grams, it contains 8 μg MK-4 and 65 μg tetrahydro-MK-9, and cited evidence that it also contains another ~50 μg of MK-8 and MK-9. In our database, we only report values that were measured in a single scientific paper for any given sample, so our data for Jarlsberg reflects what was actually measured in the Hojo paper, 74 μg, but the true value may be over 130 μg.
Our own gut microbiota also synthesize K2: Bacterioides synthesize MK-10 and MK-11, Enterobacteria synthesize MK-8, Veillonella synthesize MK-7, and Eubacterium lentum synthesizes MK-6 (Shearer, 2014). However, this probably makes little if any contribution to our own vitamin K status for two reasons: first, most of this occurs in the large intestine, which is well past the sites of vitamin K absorption in the small intestine, and all the K2 is stuck in bacterial membranes that would have to be digested to release it.
MKs produced during the fermentation of foods such as cheese or natto are also bound in bacterial membranes, but when we eat them we digest those membranes to release the K2 in the small intestine where it can be absorbed. Some animals eat their own feces, a practice known as coprophagia, and this allows the the microbiota-derived K2 to be released and absorbed in the same way as when we eat cheese or natto. This may explain the recent finding that pork products are extremely rich in MK-10 and MK-11 (Fu, 2016). The meat was obtained from supermarkets in Eastern Massachusetts, so it presumably came from commercial farms. Perhaps pigs on those farms whether by instinct, necessity, or accident, consume feces.The only other possibility would seem to be that the pigs are fed rotten or fermented food.
The question arises whether MK-10 and MK-11 provide similar bioavailability to the MKs in other foods, which are generally much richer in MK-4 (animal foods), MK-7 (natto) or MK-8 and MK-9 (cheese) than in MK-10 or MK-11. In humans, MK-10 and MK-11 tend to predominate in the liver rather than in other tissues, and in the mitochondria rather than in the endoplasmic reticulum where vitamin K-dependent carboxylation takes place (Thijssen, 1996). Thus, we should be cautious before making a conclusion about how interchangeable the MKs in pork products are with the MKs in most other foods. Ultimately this can be resolved with studies comparing the abilities of the different MKs to support different biological functions of vitamin K.
Click here to close the detailed explanation.
The Three Best Vitamin K2 Supplements
Supplements should never be used to replace a good diet. A well-rounded nutrient-dense diet not only provides vitamin K itself in a greater diversity of forms than can be found in any supplement, but it also provides a full spectrum of other nutrients that work together with vitamin K to produce good health. As such, a good diet provides the context needed for a supplement to be both safe and effective.
When evaluating K2 supplements, I look for the following things:
- Dose: I prefer a dose from which it is easy to obtain approximately 200 ug. While it is probably effective to take a larger dose less than once a day (for example, taking 1 mg every five days), it is easier to maintain the habit of taking a daily dose.
- Form: Since different forms of vitamin K2 are distributed differently in the body, it is best to obtain a diversity of forms. In supplements, the best diversity we can obtain is to combine MK-4 and MK-7. The only supplemental MK-4 available is synthetic, but it is bioidentical, meaning it has the same chemical structure as the natural form. MK-7 on the market can be natural or synthetic; some synthetic MK-7 is bioidentical and some is not. Out of caution, I would only choose bioidentical options. Those who wish to have an entirely natural supplement should opt for MK-7 derived from the fermentation of soybeans or chickpeas.
- Cost and convenience: For any two products that are substantially equivalent, I prefer lower cost, easy online ordering, quick delivery, and the opportunity for free shipping.
Here are my top three recommendations:
- Innovix Labs Full Spectrum Vitamin K2— This supplement wins on its diversity of forms (without going overboard on its total dose). It contains both MK-4 (500 μg) and MK-7 (100 μg). The MK-7 appears to be synthetic but bioidentical. It costs $21.97 on Amazon, is fulfilled by Amazon, and is eligible for Prime. Taken once a day, it costs 24 cents per day. Taken once every three days to achieve an average dose of 200 μg, it costs 9 cents per day.
- Thorne Research MK-4 — This supplement wins on cost. Its cost is nearly identical between Amazon and Iherb ($64.62 and $64.65), and if ordered on Amazon it is fulfilled by Amazon and eligible for Prime. It contains one milligram of MK-4 per drop. While the label recommends a daily dose of 45 drops, this is based on studies using pharmacological doses to treat osteoporosis. It is easy to instead take one drop per day to obtain a nutritional dose. Taken like that, it costs 5 cents per day. Taken once every five days to achieve an average dose of 200 μg, it costs one cent per day. They also make a combination of vitamin D and K2 that is more expensive but easier to get a consistent daily dose of 200 μg from. This is described in more detail in the comprehensive review below.
- Nested Naturals K2 — This is free of GMOs, soy, and other common allergens. It is made from fermented chickpeas. The MK-7 is made by another company, MenaQ7, whose MK-7 is sold under many different names and has also been used successfully in scientific research. This is the least expensive of all of the natural MK-7 products. It contains 100 μg of MK-7 and costs 12 cents per capsule. Taken twice per day to achieve 200 μg, it costs 24 cents per day.
An interesting runner-up is Nature’s Plus, which is an affordable MK-7 supplement that is interesting mostly for its long list of features, like its background blend of plant, mushroom, and algae extracts, and its substantial list of third party certifications. It is described in more detail in the comprehensive review below.
If you have the time for home fermentation, Dr. Mercola created a starter culture that is designed to generate K2 during the fermentation of vegetables. While I do not believe this will provide a standardized amount of K2 like a commercial supplement will, I would expect it to substantially augment the K2 content of your diet.
These are my top recommendations from a much more extensive review of over twenty supplements. If you want more details, click below for the comprehensive review.
Vitamin K2 Supplements: Quality, Convenience, and Price
Here is my comprehensive review of vitamin K2 supplements. It doesn’t cover every single supplement on the market, but it covers the supplements that provide singular doses of about one milligram or less and are easily accessible through the major online retailers Amazon and iHerb. If you would like me to review a supplement that didn’t make the list, please let me know in the comments.
I have broken the list into five categories according to whether they provide a combination of MK-4 and MK-7, only MK-4, only synthetic MK-7, only natural MK-7 from chickpeas, or only natural MK-7 from natto. Within each category, I have listed them from least expensive to most expensive.
One concern for synthetic MK-7 supplements is whether they are bioidentical. Natural MK-7 is all-trans (Bentley, 1982). If synthetic MK-7 is not guaranteed to be bioidentical, it may contain cis forms. While it is difficult to find reliable information on the biological activity of cis MK-7, cis phylloquinone fails to support vitamin K-dependent carboxylation in the rat (Knauer, 1975). Therefore, I recommend avoiding synthetic MK-7 supplements that do not guarantee the all-trans configuration. Notably, many of the MK-7 supplements use one of two products made by MenaQ7, either synthetic or from fermented chickpeas, both guaranteed to be all-trans. This MK-7 has the advantage of having been used in scientific studies and shown to be effective.
The prices listed were retrieved between December 4 and December 7, 2016 and are subject to change. Where I link to more than one way of obtaining a supplement, the cents per capsule and cents per 200 μg calculations are based on the least expensive option. Additions were made to this review on December 29, 2016. They are catalogued here.
Mixed MK-4 and MK-7 Supplements
Life Extension Super K With Advanced K2 Complex — 1 mg K1, 1 mg MK-4, 200 μg mK-7, with an additional 10 mg ascorbic acid from 25 mg ascorbyl palmitate. Sold by iHerb ($22.50) but cheaper at Amazon ($17.93). Eligible for Prime and Amazon Fresh. 20 cents per capsule, 3 cents per day to average 200 μg/d. Beware of the subscription button when buying on Amazon. The vitamins are synthetic. According to Life Extension, the MK-7 is synthesized in China and is bioidentical, but they could not verify for me that it is 100% all-trans, which is the natural form. The reason I do not advocate this supplement is because the high dose of K1 adds little value, and although there is no well characterized risk of high doses, it is possible that multiple milligrams per day of vitamin K (this supplement itself provides 2.2 mg per capsule) may unnecessarily tax the body’s antioxidant system.
Maxx Labs Vitamin K2 Complex — 500 μg MK-4, 100 μg MK-7, 100 mg calcium from calcium citrate. 20 cents per capsule, 7 cents per day to average 200 μg/d. $17.98 on Amazon, where it is fulfilled by Amazon and eligible for Prime. Be careful to avoid the subscription setting if you only want to order one bottle. Free of GMOs and allergens.
Innovix Full-Spectrum K2 — 500 μg MK-4, 100 μg MK-7. 24 cents per capsule, 8 cents per day to average 200 μg/d. $21.97 on Amazon, fulfilled by Amazon and eligible for Prime. Both forms of K2 in this product appear to be synthetic but bioidentical. It contains caramel coloring derived from non-GMO corn, a potential source of allergens. I consider this the best choice for a mixed MK-4/MK-7 supplement.
Country Life Vegan K2 Strawberry Smooth Melt — 500 μg total K2. MK-4 and MK-7 in unidentified proportions. 19 cents per smooth melt, 8 cents per day to average 200 μg/d. Almost identical prices on Amazon ($16.65) and iHerb ($16.67). On Amazon, it is fulfilled by Amazon and eligible for Prime. It is not clear where the vitamins come from or whether the MK-7 is bioidentical. It is free of GMOs, soy, and other common allergens.
Pure Encapsulations Synergy K — 1,000 IU Vitamin D3, 1 mg MK-4, 500 μg K1, 45 μg MK-7. 47 cents per capsule, 9 cents per day to average 200 μg/d. $56 on Amazon, where it is fulfilled by Amazon and eligible for Prime. Free of GMOs and allergens. Taken to yield an average close to 200 μg K2, the amounts of vitamin D (200 IU) and MK-7 (9 μg) are rather low compared to the Innovix Full-Spectrum K2 (20 μg MK-7) or the Thorne Research D/K2 (1,000 IU vitamin D), but the unique combination of the three vitamins may be optimal for some people whose nutritional needs fit it just right.
MK-4 Supplements
Thorne Research Vitamin K2 — 1 mg MK-4. 5 cents per drop, 1 cent per day to average 200 μg/d. Similarly priced at Amazon ($64.62) and iHerb ($64.65), and if ordered on Amazon it is fulfilled by Amazon and eligible for Prime. It is dissolved in a base of nothing but MCT oil and mixed tocopherolsd. This is the least expensive option in the list.
Thorne Research D/K2— 1000 IU vitamin D and 200 μg MK-4. 4 cents per day to obtain 200 μg from each two-drop serving. Although available on Amazon from third party shippers at prices ranging from $36-$70, it is not eligible for Prime and it is much less expensive ($23.70) through iHerb. This is a great option for someone who also needs to improve their vitamin D status. When compared to the Thorne Vitamin K2, it has the added benefit that the dose of MK-4 is smaller so it is easier to take a consistent dose of 200 μg every day. However, don’t be fooled by the price difference: the bottle costs less (hardly more than a third the price), but on a per 200 μg basis it is four times as expensive.
Superior Source Sublingual MK-4 Tablets — 500 μg MK-4. 29 cents per tablet and 12 cents per day to average 200 μg per day. Similar price from Amazon ($17.59), where it is shipped and sold by Amazon as well as eligible for Prime, and iHerb ($17.79). The company claims that the sublingual formulation offers superior absorption but I’m not aware of any specific evidence of this. It contains lactose, so should be avoided by people with lactose intolerance.
Synthetic MK-7 Supplements
Amazing Nutrition MenaQ7 — 100 μg MK-7. 12 cents per capsule, 25 cents per day for 200 μg . $14.99 on Amazon where it is fulfilled by Amazon and eligible for Prime free one-day shipping. Free of common allergens and bioidentical.
Young Life Research MenaQ7 and Organic Coconut Oil — 100 μg MK-7. 16 cents per capsule, 32 cents per day for 200 μg . $19.47 from Amazon, fulfilled by Amazon and eligible for Prime. Free of common allergens and bioidentical. Non-GMO. I consider this the best balance of quality and price from among the synthetic MK-7 supplements.
Superior Source Sublingual Vitamin K2-MK7 — 100 μg MK-7. 25 cents per tablet, 50 cents per day for 200 μg . Less expensive from Amazon ($14.99) than from iHerb ($16.06). On Amazon, it is sold by Amazon and eligible for Prime,. The company claims that the sublingual formulation offers superior absorption but I’m not aware of any specific evidence of this. It contains lactose, so should be avoided by people with lactose intolerance. The company does not claim this is bioidentical.
Life Extension Low-Dose Vitamin K2 (MK-7) — 45 μg MK-7. 14 cents per capsule, 56 cents per day for 180 μg and 69 cents per day for 225 μg . Less expensive from Amazon ($12.49) than from iHerb ($13.50). On Amazon, it is eligible for Prime free one-day shipping and Amazon Fresh. According to Life Extension, the MK-7 is manufactured in Poland, but any further information is proprietary. Presumably it is synthetic and not bioidentical.
K-Force — 5,000 IU vitamin D3, 180 μg MK-7. $1.13 per capsule, and $1.13 per day to yield 180 μg or $1.20 per day to yield an average of 200 μg/d. $67.95 on Amazon, where it can be obtained with free shipping but is not fulfilled by Amazon or eligible for Prime. The company lists the MK-7 as soy-free but does not clarify its origin. Presumably it is synthetic, but it may be derived from fermented chickpeas. This supplement is useful specifically to people who need to take 5,000 IU of vitamin D per day.
Natural MK-7 From Chickpeas
These all derive their MK-7 from MenaQ7. Everything in this section is the fermented chickpea product.
Nested Naturals K2 — 100 μg MK-7. 12 cents per capsule, 24 cents per day to take 200 μg. $21.95 on Amazon, where it is fulfilled by Amazon and eligible for free one-day shipping, but beware of the subscription button. Free of GMOs, soy, and other common allergens. This is the least expensive of the products derived from fermented chickpeas and remains the least expensive even when including those derived from natto.
Doctor’s Best Natural Vitamin K2 — 100 μg MK-7. 18 cents per capsule, 37 cents per day to take 200 μg . Almost identical prices on Amazon ($11.06) and iHerb ($11.25). On Amazon, it is sold by Amazon and eligible for Prime free one-day shipping and Amazon Fresh delivery, but beware of the subscription button. Free of GMOs, soy, and other common allergens. They also sell a 45 μg dose, but it is much more expensive if trying to achieve 200 μg per day.
Sports Research Vitamin K2 — 100 μg MK-7. 25 cents per capsule, 50 cents per day to take 200 μg . $14.95 on Amazon, where it is fulfilled by Amazon and eligible for free one-day shipping. The fermented chickpea product comes from MenaQ7, which distributes their MK-7 products under many names. Free of GMOs, soy, and other common allergens. It’s main special feature out of the fermented chickpea products is the snap-top that the company says maintains better freshness.
Dr. Mercola Vitamin K2 — 150 μg MK-7. 79 cents per capsule: 79 cents per day to take 150 μg , $1.58 per day to take 300 μg , or $1.05 per day to take an average of 200μg per day. The cost is nearly identical between iHerb ($71.37) and Amazon ($71.97) but slightly less expensive on iHerb. On Amazon, it ships from a third party and is not eligible for Prime. Free of GMOs, soy, and other common allergens.
Natural MK-7 From Natto
Healthy Origins Vitamin K2 as MK-7 — 100 μg MK-7. 14 cents per softgel, 28 cents per day to get 200 μg . Less expensive at iHerb ($24.99) than at Amazon ($29.50). On Amazon, it is sold by Amazon and eligible for Prime. Beware of the subscription button, and beware of the bottle containing 60 softgels rather than 180, which is much more expensive per softgel. The company says this product comes from natto but is free of soy. It contains non-GMO corn starch, a potential source of allergens. This is the least expensive option from among the natto-derived supplements.
Sonora Nutrition Vitamin K2 Natural MK-7 — 100 μg MK-7. 18 cents per capsule, 36 cents per day to get 200 μg. Available on Amazon, where it is fulfilled by Amazon and eligible for Prime free one-day shipping. Presumably made from soy.
Natural Factors K2 — 100 μg MK-7. 21 cents per capsule, 42 cents per day to achieve 200 μg. $12.57 from Amazon. Derived from non-GMO natto. The company has a unique farm-to-capsule model where it controls everything that goes into its supplements from the soil to the encapsulation.
Nature’s Plus Source of Life Garden Vitamin K2 — 120 μg MK-7. 22 cents per capsule. 43 cents per day to obtain 240 μg , 37 cents per day to take an average of 200 μg . Less expensive on Amazon ($12.95) than iHerb ($15.13). On Amazon, fulfilled by Amazon and eligible for Prime. Contains a blend of plant, mushroom, and algae extracts. Certified organic, certified non-GMO, certified allergen-free.
Now Foods MK-7 Vitamin K2 — 100 μg MK-7. 21 cents per capsule, 42 cents per day to get 200 μg . 19 cents per capsule, 38 cents per day to get 200 μg. Less expensive at Amazon ($11.46) than at iHerb ($12.73). On Amazon, it is sold by Amazon and eligible for Prime free one-day shipping and Amazon Fresh, but beware of the subscription button. From non-GMO natto. Contains soy. Does not contain other common allergens but processed in a facility where other allergens may be present.
Nutrigold Vitamin K2 MK-7 Gold — 100 μg MK-7. 23 cents per capsule, 45 cents per day to get 200 μg. $27.99 from Amazon. Sold by Amazon and eligible for Prime, but beware of the subscription button. Non-GMO. Made from soybeans, but free of allergenic soy protein. Free of other common allergens as well, verified by third party testing.
Natural Factors D3 & K2 — 1000 IU vitamin D, 120 μg MK-7. 35 cents per softgel, 58 cents per day taken to average 200 μg/d, or 70 cents per day to yield 240 μg. Identical in price ($20.97) between Amazon and iHerb. MK-7 is derived from non-GMO natto. The company has an unusual farm-to-capsule model where it controls everything that goes into its supplements from the soil to the encapsulation. Taken to yield an average daily dose of 200 μg K2/d, it yields 1,667 IU vitamin D; taken twice a day to yield 240 μg K2, it yields 2000 IU of vitamin D, both of which are more than the 1,000 IU of vitamin D in Thorne Research D/K2. However, the Thorne product contains MK-4 and this product contains MK-7. This is the only product that combines relatively high doses of vitamin D and MK-7.
Jarrow Formulas MK-7 Vitamin K2 — 90 μg MK-7. 20 cents per softgel. 42 cents per day to get 180 μg, 47 cents per day to average 200 μg. Less expensive at iHerb ($12.48) than at Amazon ($13.55). On Amazon, it is sold by Amazon and eligible for Prime free one-day shipping and Amazon Fresh, but beware of the subscription button. From non-GMO natto. Contains soy but free of most other common allergens.
Carlson Labs Vitamin K2 MK-7 — 45 μg. 13 cents per capsule, 53 cents per day to get 180 μg, 67 cents per day to get 225 μg. Less expensive buying a 180-capsule bottle from iHerb ($24) than the 90-capsule bottle sold on Amazon ($15.23). On Amazon, sold by Amazon and eligible for Prime free one-day shipping and Amazon Fresh, but beware of the subscription button. Made from natto and contains soy, though their own web site suggests they may have switched to chickpea.
Bluebonnet Nutrition Vitamin K2 — 100 μg. 32 cents per capsule, 64 cents per day to get 200 μg. Almost identical in price between Amazon ($32.39) and iHerb ($32.40). On Amazon, fulfilled by Amazon and eligible for Prime, but beware of the 2-bottle package that is more expensive and not eligible for Prime. Made from natto. Non-GMO, Kosher, contains soy but free of other common allergens.
Nature Made Vitamin K2 Softgel — 100 μg. 52 cents per softgel, $1.03 per day to get 200 μg. $15.45 on Amazon, where it is sold by Amazon and eligible for Prime. Made from “natto organism,” and contains soy.
High-Dose MK-4
Supplements where the lowest dose contains 5 mg or more of MK-4 are included in this section. It is impractical to use these supplements to reach an average dose of 200 μg/d. They are primarily useful as a means of reaching the pharmacological dose of 45 mg/d that has been used to treat osteoporosis, to prevent the occurrence of hepatocellular carcinoma in women with viral cirrhosis, and to prevent the recurrence of the same disease in people who have already been treated for it. Although high-dose MK-4 supplements are available over-the-counter and have a low risk of side effects, these treatments are pharmacological rather than nutritional in nature. Therefore, I recommend using them under the supervision of the physician who is overseeing treatment for one of these conditions.
Advanced Orthomolecular Research Peak K2 — 15 mg MK-4. 35 cents per capsule and $1.04 per day to reach 45 mg. Less expensive on Amazon ($31.30) than iHerb ($34.56). On Amazon, fulfilled by Amazon and eligible for Prime. Free of common allergens.
Note: This company also makes a low-dose supplement, but it can't be ordered online and the company is not transparent about its price, so I am not including it in this review.
Relentless Improvement Vitamin K2 — 15 mg MK-4, 60 μg MK-7. 39 cents per capsule and $1.17 per day to reach 45 mg. $34.95 per bottle on Amazon, where it is fulfilled by Amazon and eligible for Prime free one-day shipping. Taken to provide 45 mg/d MK-4, it also provides 180 μg/d MK-7. While research suggests that MK-4 and MK-7 have different tissue distributions at low doses, it is unclear whether there is any benefit to adding a low dose of MK-7 to a far higher dose of MK-4. The vitamins are synthetic and the company guarantees a low percentage of inactive cis isomers.
Carlson Labs Vitamin K2 — 5 mg MK-4. 18 cents per capsule and $1.66 per day to reach 45 mg. Less expensive on Amazon than on iHerb. On Amazon, the 60-capsule bottle ($10.99) and 180-capsule bottle ($33.26) are both equivalent in price per capsule. Both are fulfilled by Amazon and eligible for Prime, and the larger one is eligible for Prime free one-day shipping. Be careful of the subscribe and save button on the smaller bottle. iHerb only sells the 60-capsule bottle ($14.94).
Food-Based Supplements
Supplements included in this section are those that isolate a food oil itself or a major fraction thereof rather than specifically isolating one or more forms of vitamin K2. The nutrients in these supplements are less concentrated, but they are present in a broader network of synergists. While vitamin K2 supplements are a great way to optimize vitamin K status in someone whose diet is otherwise good, food-based supplements are likely to be better ways of compensating for an otherwise suboptimal diet.
Walkabout Australian Emu Oil — 40 cents per gram as a liquid oil, 52 cents per gram as capsules. Each capsule contains one gram of total oil and 4 μg MK-4. This product is not available on Amazon or iHerb. Its price is identical between Radiant Life, where the liquid oil ($45) and capsules ($52) can be ordered on the same page, and Corganic, where the oil and capsules are available on separate pages. Additional shipping charges apply to both sellers. Shipping charges for RadiantLife would be $7.95 for the liquid oil, $9.95 for the capsules, and free for a total order over $125. Corganic shipping charges depend on your address. Reaching 200 μg K2/d with this product would require 48 capsules or 3.5 tablespoons per day of the liquid oil and is obviously impractical. However, five capsules per day would yield 20 μg/d; added to a nutrient-poor diet containing only 15-20 μg/d on its own, this would double a person's K2 intake. The oil also naturally contains a blend of essential fatty acids and other fat-soluble vitamins.
Green Pastures X-Factor Butter Oil — 43 cents per capsule, with each capsule containing 0.5 grams of oil. Less expensive on Amazon ($43.20) than on the Green Pastures web site ($60). On Amazon, fulfilled by Amazon and eligible for Prime free one-day shipping. However, the Green Pastures web site offers liquid oils as well as capsules and offers a greater diversity of flavors than available on Amazon. Each capsule contains 0.4 μg of K2, mostly as MK-4. Reaching 200 μg/d would require 500 capsules per day and is obviously impractical. However, Green Pastures has in the past reported an unidentified set of quinones in the oil, which could upon further testing be shown to have additional vitamin K activity. For example, the fermentation of the oil could produce tetrahydromenaquinones, which are found in high concentrations in certain cheeses but have not been measured in the butter oil. The oil also naturally contains a blend of essential fatty acids and other fat-soluble vitamins.
Click here to close the comprehensive review.
Light and Heat Stability, and Proper Storage of Vitamin K2
Vitamin K is only slightly sensitive to heat, but is extremely sensitive to light. So much so that when we measure vitamin K in a laboratory we work under yellow lamps. In food oils exposed to daylight, 80 percent of the vitamin K disappears within two days. To make sure that your food and supplements retain their vitamin K content over time, keep them in the refrigerator, behind cabinets, or otherwise out of the light when not in use. If you keep them in plain daylight, they should be in amber glass or in opaque containers such as the white plastic used for most supplements.
How Much Fat to Eat With Vitamin K2 and What Kind
Vitamin K is fat-soluble so fat helps us absorb it from foods and supplements. If your fat intake varies from meal to meal, it makes sense to eat your K2-rich foods or take your K2 supplements with the meal that contains the most fat. The optimal amount of fat to maximize absorption of K2 from a single meal is probably about 35 grams. The true optimal amount of fat has not been precisely determined and may be higher than this, but I consider it adequate.
For the best effect, the fat should be low in polyunsaturated fatty acids, which means that butter and other animal fats, tropical oils, olive oil, avocado oil, macadamia nut oil, and the high-oleic varieties of sunflower and safflower oil would help the most. By contrast, soybean oil, canola oil, the regular varieties of sunflower and safflower oil, grape seed oil, and most other oils derived from nuts and seeds would help the least.
Notably, many of the foods richest in K2 like cheese, meat, and egg yolks are themselves rich in fat. The total fat content of the meal is what is important, so the more natural fats within the foods, the less you have to add.
Vitamin K Absorption and Fat: A Closer Look
Dietary fat is important for the absorption of all fat-soluble vitamins partly because it helps dissolve the vitamins and partly because it helps stimulate the machinery involved in fat digestion, such as bile acids and lipases. Studies have generally suggested the following rule: the more fat you eat, the more fat-soluble vitamins you absorb. For example, 28 grams of fat allows better absorption of carotenoids from a salad than 6 grams of fat (Brown, 2004), and 30 grams of fat allows better absorption of vitamin E from a supplement than 11 grams of fat (Bruno, 2006). Studies have also shown that oils lower in polyunsaturated fatty acids (PUFAs) promote better absorption of fat-soluble vitamins than high-PUFA oils. For example, beef tallow allows better absorption of beta-carotene from a standardized test meal than safflower oil (Hu, 2000).
These rules appear to apply to vitamin K just the same. For example, 35 grams of fat allows better absorption of MK-4 than 20 grams of fat (Uematsu, 1996), and more K1 is absorbed from spinach with 25 grams of butter than without butter (Gijsbers, 1996). More K1 was absorbed from a “cosmopolitan” meal or an “animal-oriented” meal than from a “convenience meal,” with one possible explanation being the two-fold greater PUFA content of the convenience meal (Jones, 2009).
None of these studies showed a ceiling to the fat effect, and none of them tested more than 35 grams of fat. So, there may not be any ceiling to the effect. What we can say with confidence is that 30-35 grams of fat will provide for better absorption than lower amounts. Even still, absorption will probably never reach 0% or 100%, and for any given percent absorption one can always absorb a greater total amount of a vitamin by consuming more of it. Therefore, there is no sense in chasing after complete absorption and there is no intrinsic danger of a low-fat diet. If you have a good reason to eat less than 35 grams of fat per meal, it just becomes more important to spend the fat you do eat wisely by allocating it to K2-rich foods. It is fine to be flexible about fat intake, but it is important to be aware that any given amount of K2 in the diet will provide more nutrition to our bodies if consumed with a good dose of healthy fat.
Click here to close the detailed explanation.
How to Test Your Vitamin K2 Status
Unfortunately, there are no useful tests for measuring vitamin K status that are available to the general public at this time. However, good tests are on the horizon. VitaK will be releasing innovative medical devices to allow health care practitioners to monitor vitamin K status in patients, and ImmunoDiagnostic Systems will be releasing a blood test for dp-ucMGP, a protein that circulates in the blood when blood vessels become deficient in vitamin K.
If you would like me to notify you when these tests become available in the United States, please join my newsletter.
Tests for Vitamin K Status: A Closer Look
Vitamin K travels through the blood almost entirely as a means of being delivered to our other tissues, so blood levels of vitamin K only reflect recent intake rather than long-term nutritional status. Red blood cells lack the organelles in which vitamin K function is important (the endoplasmic reticulum, mitochondria, and nucleus). Lymphocyte vitamin K concentrations could, perhaps, reflect long-term vitamin K status, but practically nothing is known about what vitamin K does in lymphocytes in the context of human nutrition, and such tests have never been validated to show anything important.
The appropriate way to test vitamin K status is to look at the carboxylation status of vitamin K-dependent proteins. These tests can be validated by showing that they respond to vitamin K depletion or supplementation and that they correlate with known health outcomes that respond in the same way. For example, the ability of the blood to clot reflects vitamin K status in the liver, where clotting factors are made; the carboxylation status of osteocalcin reflects vitamin K status in bone, where osteocalcin is made; and the carboxylation status of matrix Gla protein (MGP) reflects vitamin K status in blood vessels, where MGP is made.
Clotting disorders are life threatening and we have known about the role of vitamin K in this process for almost a century. As a result, a whole battery of tests for the different vitamin K-dependent clotting factors are readily available (for example, Ohishi, 2014). Vitamin K1 is perfectly good at supporting the production of clotting factors, and since hemorrhage can be life-threatening, clotting factors will always get priority over a limited pool of vitamin K. Thus, most people consume enough vitamin K for their clotting factors to be fully carboxylated and these tests are not useful measures of whether vitamin K status is adequate to support its other functions in other tissues.
The most common marker of vitamin K status in research studies is the carboxylation status of osteocalcin, which reflects vitamin K status in bone. This test is only useful if the proportion of osteocalcin in the carboxylated and undercarboxylated forms can be measured. Unfortunately, this is not available outside of research studies. Quest offers total osteocalcin, but doesn’t measure its carboxylation status; Genova offers undercarboxylated osteocalcin, but doesn’t measure the total. One could “hack” its carboxylation status by getting both, but this would require each “half” of the correct marker to be measured from separate blood samples analyzed by separate laboratories, making the interpretation highly questionable. Were it available, we would still have to interpret it with caution, because, independent of vitamin K status, bone resorption decarboxylates osteocalcin and releases the undercarboxylated form into the bloodstream where it has beneficial hormonal roles, so it isn’t a black-and-white marker of vitamin K status.
The most promising marker of vitamin K status on the horizon is desphospho-uncarboxylated matrix Gla protein (dc-ucMGP), which reflects vitamin K status in blood vessels and the risk of soft tissue calcification. It’s just a matter of time before it becomes available.
Click here to close the detailed explanation.
Is Vitamin K2 Dangerous?
Very high doses of vitamin K2 have proved remarkably safe in large clinical trials, but there are safety concerns for people taking prescription anticoagulants, and there are reasons to be cautious about high doses even for healthy people.
This is Critical If You Are Taking Prescription Anticoagulants
The most common anticoagulants used in medicine are warfarin and its relatives. As a class, they are known as 4-hydroxycoumarins. These go by a number of brand names, the most common of which is Coumadin. As a class, these drugs act as vitamin K antagonists, and it is absolutely critical that anyone taking them avoid making any changes to their diet or supplements that would be expected to change their vitamin K intake except under the strict supervision of the physician who prescribed the medication.
Hypothetical Side Effects of High Doses
Long-term use of 45 mg per day of MK-4 has not revealed any established toxicity syndrome or risk of serious side effects. This is 225 times the dose I recommend. Nevertheless, the biochemistry of vitamin K suggests that unnecessarily high doses could rob the body of antioxidants or interfere with blood sugar regulation, insulin sensitivity, and hormonal health. The real question, though, is at what dose these potential side effects kick in. Since 45 mg per day has not shown any clear syndrome of toxicity and the dose I recommend is more than 200 times lower than this, I think we have a very large window of safety to work within. The potential for hypothetical side effects, however, should lead us to avoid supplementing with doses that are much larger than those that provide clear benefits.
Hypothetical Side Effects of High-Dose Vitamin K
There are several aspects of vitamin K’s biochemistry that suggest high doses could have adverse effects on our health:
- Vitamins E and K are broken down in similar pathways (Shearer, 2008). High doses of either one elicit an increase in these catabolic pathways by activating a common receptor known as the steroid and xenobiotic receptor (SXR) or the pregnane X receptor (PXR). As a result, high doses of one will elicit the destruction of the other. Thus, high-dose vitamin K could contribute to vitamin E deficiency.
- Second, a small portion of vitamin K is broken down to a compound known as menadione (Thijssen, 2006). Some of the menadione is used to synthesize MK-4, but high concentrations are toxic. We therefore conjugate a portion of the menadione to glutathione, the master antioxidant and detoxifier of the cell, and excrete the complex into our urine. High doses of vitamin K could therefore deplete glutathione. This would impair detoxification, and along with vitamin E depletion it would hurt antioxidant activity.
- High doses of vitamin K can inhibit bone resorption, which is probably the mechanistic basis by which 45 mg/day reduce fracture risk (Iwamoto, 2013). While bone resorption sounds like a bad thing, we need to use it every day to help our bones remodel themselves and adapt their structures to our lifestyles, and to keep blood levels of calcium within a precisely controlled range. We also use bone resorption to release osteocalcin into the blood, where it acts on multiple tissues to improve our metabolic and hormonal health (Ferron, 2007; Oury, 2013). Ironically, one of the benefits of vitamin K2 is to support proper production of osteocalcin, but high doses of the vitamin could hypothetically prevent us from using it. That would be expected to hurt blood sugar control, insulin sensitivity, our metabolic rate, and, in males, testosterone production.
Japanese trials using 45 mg/day MK-4 to treat osteoporosis have not established any risk of severe side effects (Iwamoto, 2013). Most of them, however, had between 20 and 120 subjects per group. One very large two-year trial with over 2,000 subjects per group (Inoue, 2009) reported 23 percent more adverse drug reactions in the MK-4 group than in the control group. The report did not include any description of what those side effects were, but confirmed that there was no difference in “serious” adverse effects or deaths.
Such high doses are pharmacological in nature and not nutritional. We should look at their costs and benefits in the same way we look at other pharmaceutical drugs. In this light, high-dose MK-4 is remarkably safe and effective. We nevertheless have hints that negative side effects of some sort occur when using extended pharmacological doses and we have several biochemical rationales for why high doses would cause harm. This provides a basis for caution in using doses outside of the nutritional range.
Click here to close the detailed explanation.
Vitamin K2: A Critical Component of a Well Rounded Nutrient-Dense Diet
Vitamin K2 is something most of us could use a lot more of. The best way to obtain it is to consume K2-rich foods in the context of a well rounded, nutrient-dense diet. The many other nutrients contained in a good diet provide the context that makes vitamin K2 safe and effective. Supplements can be very helpful, as long as they are used as adjuncts to support a good diet rather than as replacements for a good diet.
From here, you can leave a comment, scroll on for my suggestions for further reading, or search for some K2 rich foods in our database to plan out your next K2-rich meal.
Suggestions for Further Reading
In spring of 2007, I wrote “On the Trail of the Elusive X Factor: Vitamin K2 Revealed.” This is an extensive article arguing that vitamin K2 was the “activator X” that Weston Price claimed to have discovered in 1945. Weston Price was one of the pioneers of nutritional anthropology, and many people had speculated about the identity of his “activator X” for decades. The article tells the history of that mystery and in the process extensively reviews the many roles of vitamin K and its interactions with other important nutrients like vitamins A and D.
For more about how vitamin K interacts with other nutrients in the diet, see my 2013 article, “Nutritional Adjuncts to the Fat-Soluble Vitamins.”
For my other writings on vitamin K2, see Start Here for Vitamin K2.
Some other sources that I recommend include Chris Kresser’s Vitamin K2: The Missing Nutrient, and Stephan Guyenet’s writings on the topic. Kate Rheaume-Bleue wrote a great book, Vitamin K2 and the Calcium Paradox: How a Little-Known Vitamin Could Save Your Life.
For a more advanced understanding of vitamin K, I would start with the vitamin K chapter by John Suttie in Modern Nutrition in Health and Disease. I consider this textbook so valuable as a general scientific reference that I buy it again every time there is a new edition. Reviews by important figures in the field such as Martin Shearer, John Suttie, Sarah Booth, Cees Vermeer, and Leon Schurgers are also highly valuable and can be found on pubmed. On the specific topic of the hormonal functions of osteocalcin, I recommend reviews by Gerard Karsenty, also found on pubmed. Finally, the expandable “detailed explanation” sections within this resource are rich in scientific references that provide additional opportunities for advanced learning.
I’d Like to Hear From You
I would like to make this a multi-purpose resource for all things related to vitamin K2 that can be constantly improved over time. Therefore, I’d like to hear from you: what is most useful? What can be improved? What topics would you like to see included in the future? What features would you like to see added to the searchable database? Please let me know in the comments.
The Database: Search for the Vitamin K2 Contents of Foods
Here’s the icing on the cake. We scoured the literature for data on the K2 contents of foods and found many publications that haven’t been included in databases elsewhere. There are almost 200 foods included. You can search by keyword, or you can submit a blank search to browse through everything. You can pick a food category and search it by keyword or submit a blank search to browse through just the foods in that category. Every food entry gives you the opportunity to click for more details, including a breakdown of its different vitamin K forms and the reference from which the data comes. Have fun searching!
This resource is continually updated so that it will remain the most useful resource on vitamin K2 over time. Click below for a list of updates.
Several people found the third row of the second infographic, “Why It Matters What Type of Vitamin K We Eat,” difficult to read. We changed the font from all-caps to regular capitalization and made the background darker, and it is now much easier to read. My site has, since it started, loaded rather slowly, and that's because I had a budget of near zero when I started it and got a deal of one year free hosting. Being free, it was nothing to complain about. However, The Ultimate Vitamin K2 Resource has a lot to load and is generating tons more traffic to the site, which means its time for an oil change. I migrated my site to WP Engine, which instantaneously cut the load times on my pages by 65%. WP Engine offers a lot of assistance in further optimizing your site for performance and speed. I have yet to take advantage of any of that, but hope to in January. Nevertheless, simply moving from one server to another has caused everything to operate at three times the speed. My choice to move to WP Engine happened after a failed migration to another company's servers. I'll keep them nameless for the time being, but my own hastiness combined with their inadequate technical assistance and customer service caused my site to temporarily crash worldwide. I apologize to any of you who experienced any frustration as a result of this during the transition. The WPEngine migration was smooth as a baby's bottom for two reasons: first, most of it is automated with a fantastic plugin; second, their customer service is off-the-charts, with unlimited continuous access to both phone and live chat. While the downtime the site experienced is embarrassing to me, I'm incredibly happy with the end result. It's pricey, but I intend this site to be awesome in every way in 2017, and awesome content is only as awesome as the speed and performance of the site that hosts it. Originally, the searchable database opened in the same tab. If you wanted to do more than one search, you had to hit the back button, which brought you all the way to the top of the article. All this was far more terrible than it sounds, because the slow site speed prior to the WPEngine migration was causing each of these events to take 10 seconds! Imagine doing five keyword searches, with each search taking 10 seconds, each time going back to the page taking 10 seconds, and then going back to the database with several more seconds, depending on your scrolling skills. A nightmare. Now, the database opens in a new tab, so you are never more than a tab-switch away from it for a new search. Plus, the site migration has made each keyword search load three times faster. Together, searching the database now offers a much better experience. Many people requested data on Walkabout Australian Emu Oil and Green Pastures Butter Oil. These have now been added to the database. The data for these products comes from a set of foods sent by the Weston A. Price Foundation to VitaK for independent analysis. Since the foundation has made the original lab report publicly available, I was able to add these foods to the database and be confident that I was maintaining the same level of rigor as before. To date, every single entry in the database has the exact source of information available to the user simply by clicking on “view more details” under the specific result, and the sources come either from the peer-reviewed scientific literature or independent analyses documented with original lab reports. Other foods added to the database include oysters, fish roe, shrimp, conventional and pastured chicken liver, cheeses and butters of different varieties with name brands or local farm sources listed, egg yolks, tallow, duck fat, lard, and cod liver oil. If you're salivating already, go on and search your heart out in the database. In response to audience requests, the following supplements have been added to the comprehensive review. I have not changed my top three recommendations in the main text. These include mixed MK-4 and MK-7 supplements, natto-derived MK-7 supplements, and an apparently synthetic MK-7 supplement. Additionally, I created two new categories: High-Dose MK-4, and Food-Based Supplements. Click Here to Close the Update Log.Improved Clarity to the Second Infographic
The Site Now Loads Three Times Faster
The Vitamin K2 Searchable Food Database Now Opens in a New Tab
Emu Oil, Green Pastures Butter Oil, and Over a Dozen Other Foods Have Been Added to the Database
10 Supplements Have Been Added to the Review
Mixed MK-4 and MK-7 Supplements
Natural MK-7 From Natto
Synthetic MK-7 Supplements
High-Dose MK-4
Food-Based Supplements
Join the Next Live Q&A
Have a question for me? Ask it at the next Q&A! Learn more here.
Subscribe
Subscribe or upgrade your subscription here.
Masterpass members get access to premium content (preview the premium posts here), all my ebook guides for free (see the collection of ebook guides here), monthly live Q&A sessions (see when the next session is here), all my courses for free (see the collection here), and exclusive access to massive discounts (see the specific discounts available by clicking here). Upgrade your subscription to include Masterpass membership with this link.
Learn more about the Masterpass here.
Take a Look at the Store
- At no extra cost to you, please consider buying products from one of my popular affiliates using these links: Paleovalley, Magic Spoon breakfast cereal, LMNT, Seeking Health, Ancestral Supplements. Find more affiliates here.
- For $2.99, you can purchase The Vitamins and Minerals 101 Cliff Notes, a bullet point summary of all the most important things I’ve learned in over 15 years of studying nutrition science.
- For $10, you can purchase The Food and Supplement Guide for the Coronavirus, my protocol for prevention and for what to do if you get sick.
- For $15, you can pre-order a single format of my Vitamins and Minerals 101 book, my complete guide to nutrition, which I am currently working full-time on finishing.
- For $25, you can pre-order a digital bundle of my Vitamins and Minerals 101 book.
- For $29.99, you can purchase a copy of my ebook, Testing Nutritional Status: The Ultimate Cheat Sheet, my complete system for managing your nutritional status using dietary analysis, a survey of just under 200 signs and symptoms, and a comprehensive guide to proper interpretation of labwork.
- For $35, you can pre-order a complete bundle of my Vitamins and Minerals 101 book.
- For $250-$1499.99, you can work one-on-one with me.


Hi Chris, I have osteoporosis, I am looking for a cheese that is high in MK-7, I am already supplementing with MK-4, I am taking 45mcg, I am sensitive to all fermented foods and would like to eat some cheese to get my MK-7, could you please help me? Thank you Lori
Hi, does cooking eggs destroy the Mk4 content? Is it better to consume yolks raw? Thanks.
No it does not kill the K2… usually high heat and other manipulations can do so, for example, in most cod liver oils. Consider that cheese is a fairy good source of K2 (MK-4) but it also contains some higher chain Mk’s (not-7_
some consume them raw and raw egg yolks from pastured chickens are the ultimate in nutrients; but they must be grown by a farmer you know and trust. Otherwise there may be risk of salmonella.
I ordered a vitacost brand of vitamin K2 MK7 with nattokinase. It stayed in the mailbox for the entire day at 99° temperatures outside. Do you think that this would damage the supplement?
Hello – I recently read an article about taking vitamin K supplements several hours apart from vitamin D supplements to avoid nutrient competition. Has anyone heard of this? I wish there was a test for vitamin K levels to check this out. I take most of my vitamin D along with other fat-soluble vitamins (including K) and my main meal, and my vitamin D levels are good, i.e. apparently not affected by taking it together with K, but do not know my vitamin K level to know if that is being affected.
I have a supplement where the D3 and K2 are in the same capsule. There is not a direct test for K2. It is hard to take too much K2, and the supplementation I have read is 180 mcg a day. You can get k2 from fermented foods. If you take them with some oil even fish oil , I think you are just fine to take together.
I really enjoyed the Vitamin K podcast, this article, and the searchable database. I was at first excited to see that natural emu oil appeared to be a great natural source of Vitamin K because I thought I could pop a couple of emu oil pills and be good. Then I considered that 50 g of emu oil is a lot harder to consume daily than 50 g of pork sausage, so I think I’ll try to get a combination, along with green leafies. Although kind of nasty to hear your insight about why pork may have higher MK-10 levels than other meat. Yuck. I agree – it would be interesting to hear if humanely-raised pigs in more spacious locations would have lower MK-10 levels.
Super cool to learn that biotin and Vitamin K are the only vitamins that handle carboxylation.
Also very interesting to hear that MK-4 helps turn off cancer-promoting genes and turn on sex-hormone related genes. Also interesting that statins downregulate the conversion of K1 to MK-4, which implies that statins can increase our cancer risk and decrease our sex hormone production. Considering also statin’s downregulation of the building blocks that make sex hormones, that’s a double whammy effect of statins having a potential negative impact on sex hormone production.
I loved learning from your site and a research article that Matrix GLA protein (MGP), is the most potent inhibitor of tissue calcification and is activated through 1) phosphorylation and 2) carboxylation, and the carboxylation status is the result of vitamin K levels. So interesting to realize that adequate Vitamin K levels help solve two common problems: soft tissue calcification and osteoporosis.
Finally, I’m a big fan of Weston Price, so fun to learn more about Activator X. Thanks so much for all your research!
Hi, Great info. I’d like to add to the supplement list a review of rnareset’s D3 K2. Thanks. Dr. Dean wrote The Magnesium Miracle and has formulated her own high quality supplement line. Thanks.
Interested in D3 and calcium and K2. As an older female….BUT…I have Alpha Gal Syndrome…everything that goes into my body must be mammal free…including by products
I am wondering about the K2 MK-7 made by Horhaach. It seems to be cheaper than a lot of the other K2 MK-7 you mentioned. it’s Vitamin K2 (as Menaquinone-7 MK-7) (from Bacillus subtillis ssp. natto)
https://horbaach.com/
My understanding is that pantaprozole interferes with absorption of K2. Thus one should take K2 before taking pantaprozole which takes about 30 minutes to take effect.. Is this correct? .Any other comments re K2 and pantaprozole will be appreciated.
I have been following this Activator X/vitamin K2 business ever since I read Price’s book about 30 years ago and your work identifying it as K2 in 2007 and Rheume-Blue’s book. I am a retired research biochemist with a background in blood clotting (I purified and characterized several of the vitamin K dependent clotting factors and their inhibitors) and also worked in the biotech industry developing viral diagnostics and vaccines using recombinant proteins. I wish that there were (more) studies identifying all of the places in the body where the various vitamin K2 types partition as well as their circulating lifetimes/halflives. I know K4 does get into the brain and I remember Price suggested that it can be found in the saliva. But it would be very useful to know if there is/are other organs that it has a preference for.
I tried k2 mk7 sports research and had chest pain. I’m going to try k2 from natto supplement. Thank you for guide for k2
I suggest you try another brand.I am using Life extension brand.
our product (vK2) contains both MK4 and MK7. Unlike most other formulas our ingredients are pharmaceutical grade (with NO Chinese sourced ingredients and with with a VERY high percent of the bioactive “trans” form).
Mk7 is known for side effects. Stick with mk4.
Which collaterals?
Hello Mr. Master John,
I have come upon a vitamin K supplement that isn’t into your list and looks intriguing! It is called Koncentrated K and contains high dosage MK-1, MK-4, MK-7 and astaxanthin. Being a WAP member and follower, I’m hesitant taking it without knowing more about it. The price is quite appealing. I do eat butter oil, natto, cheese and dessicated organ tablets along with astaxanthin, which of course isn’t cheap. I’d so appreciate it your input on this product
Thank you so much
Kindly,
Isabelle
I’m no expert on anything, just a layman; I’ll do what I can. I’ve been taking Kon-K for a year or two. I can assure you it’s a legitimate product and is safe. Whether it actually does anything is like all the other supplements I take–I can only hope something good metabolically is happening in my body.
The people at Innovix Labs will tell you that the MK-4 dosage is way too high without benefit, and maybe the MK-7 dosage as well. I spoke with the man at Kon-K about the astaxanthin dosage being low compared to a recommended dosage of 12mg (I think is the number) by True Health, and he gave me a technical answer I didn’t understand.
Your comment way below imbedded in comments from 2016 probably won’t be seen by many people. And Chris Masterjohn doesn’t seem to be active here anymore, so don’t expect to hear from him. Finally, clicking on the link in the email informing me of new comments here about managing my subscription now results in a page-not-found message. Not sure if this website is a “going concern” anymore.
Good luck.
Koncentrated K is 50%/50% trans/cis so the active dosage is inflated. Trans (active form) should be in the high 90s. Also, they claim natural source for the MK4. Not possible.
Whoa. Over 1200 comments, I can’t possibly find the answer I’m looking for, lol.
I have a D3/K2 liquid supplement I bought because calcium needs both for optimal absorption. Unless you said otherwise and I missed it.
Now I’m not sure I was providing enough dietary fat at the same time the D3/K2 was taken. I know fat is needed. I didn’t know how much until your article. Can D3/K2 be taken (with fat) separately from calcium? As long as they’re in the same day, it’s okay? Or do they all need to be in the same meal?
It is better in the same meal. It is better to talk D3/K2 with a meal that has some fat. It can be whole greek yogurt.
Is consuming Natto not recommended for individuals with an increased prothrombin gene mutation or would the fibrinolytic aspect balance out the K2 increased prothrombin?
Rarely find informative articles like this. Everyone ends up spending a lot of money on diseases nowadays. So better we know what actually makes us ill and try to avoid unnecessary things from our healthy life.
This was really good, I did study K2, and you gave so much more information on it all, Im glad to see my diet is spot on and I do take d3 k2. I also love it when an expert like you dont poo poo good healthy animal fats. I think that reducing your good fat intake is a disaster for your health
How long is Thorne k2 likely to last in fridge?
To have 1c per day it needs to last something like 20 years.
Doable?
I would think that is an expiration on the bottle. I would not go much beyond that because of the oxidation of K2. In the fridge. Are there other people in the family you can share with?
It says directly on the bottle “Do not refrigerate”
when i click on; “Carson Labs Vitamin K2 MK-7” link, at the beginning of the paragraph, it takes me to iHERB instead.
Hi Chris,
I am the author of the vitamin K chapter in teh Textbook of natural medicine 2020.
I think that your guide on vit K needs updating. I sent you a private e-mail to support@chrismasterjohnphd.com
Cristiana Paul, MS
Keen to see any updates.
Thank you for your comment! I found your video very informative!!! I’ll link it for others below. My husband has a huge jaw cyst (silver dollar) that will need to be decompressed with a drain over the course of a year while hopefully regrowing his jaw bone back. Right now it is eggshell thin. I bought the designs for health D supreme that has D3K1/K2/ GG. Would you recommend this or following the osteoporosis protocol? He’s 42.
https://www.drweitz.com/2023/01/controversies-on-vitamin-k-with-christina-paul-rational-wellness-podcast-290/?utm_source=rss&utm_medium=rss&utm_campaign=controversies-on-vitamin-k-with-christina-paul-rational-wellness-podcast-290
Thanks for such an informative document. I had been trying to find something like this. I have been living a pro metabolic lifestyle with food and avoiding stress, toxin, and following Dr Ray Peat. It had been suggested to take asprin daily as a anti inflammatory, to assist with health especially in our current times. I was also advised to take vitamin k with the asprin to assist with the blood thinning. Do you have any information on this? I bought Health Natura True K2 which has K2-Mk4 in mct oil, 1mg per drop. I am still trying to figure out how much to take with the asprin. I’m having trouble finding information that is in laments terms 😊 thanks again
I think more attention should be paid to K1 when it comes to coronary artery calcification:
“Research suggests that vitamin K1 supplementation does not have cardiovascular benefit in healthy people, but, in people with existing coronary artery calcification, it may help slow progression. For example, one study in Boston showed that people with pre-existing coronary artery calcification who took a multivitamin including vitamin K1 for three years had 6% less progression of calcification than those who received the multivitamin without K1. However, among people without pre-existing calcification, an equal percentage developed calcification regardless of whether or not they received vitamin K1 (Shea, Am J Clin Nutr 2009). A study in Australia investigated the effects of vitamin K1 supplementation in men and women (average age 66) with type 1 or type 2 diabetes and moderate coronary artery calcification, half of whom were also given the anti-inflammatory drug colchicine (which can reduce the risk of heart attack and stroke in people with coronary artery disease). The study found that 10 mg of vitamin K1 taken once daily for three months decreased the risk of developing new calcified lesions in the coronary arteries and aorta, respectively, by 65% and 73% compared to placebo. These decreases were similar for those taking or not taking colchicine (Bellinge, Am J Clin Nutr 2021).”
Any information or thoughts on K for DISH (Diffuse Idiopathic Skeletal Hyperostosis)? Also, NAFLD with multiple liver cysts?
If so, what forms would be most beneficial?
feel better than never. I have more energy in bed and I am not ashamed to take off my pants. It is certainly due to getting rid of the stress of having to deal with a small penis. I can screw for 20 or 30 minutes, my penis doesn’t get soft and it has grown 5.2 inches more. My penis has grown, so far, up to 8.5 inches in 2 weeks, Having a bigger penis and satisfying your partner is really amazing and appreciative. Finally, I feel pleasure in doing it and I can satisfy the girl I’m with. Thank You Dr zubby for your trusted product, Contact Doctor Zubby for Penis Enlargement Product via WhatsApp Number: (+2348070673249 or email via dr.zubbysolutionhome@gmail.comfor Penis Enlargement Natural Herbal Product Visit his fb pages and website https://www.facebook.com/dr.zubby1/https://www.facebook.com/ZUBBYherbsproducts/
Chris what do you make of this study. It appears there is a U shaped curve for Vitamin K2, with 60-75uG being the optimum for atherosclerosis, which seems to worsen with rising intake beyond this dosage.
https://michaellustgarten.com/2021/08/20/vitamins-k1-and-k2-are-associated-with-cardiovascular-disease-related-hospitalization-risk/
video at 3m 18s
The main source of K2 in this study was hard cheese, which is high in saturated fat. Saturated fat has been shown to be associated with increased cardiovascular risk, so unfortunately this introduces a confounding variable that is proportional to the variable of interest (K2), making the study’s association difficult to interpret.
Howard, that is a persistent and debunked myth lingering from a very flawed study the 50’s. The truth is that saturated fats are the healthiest fats . . .it is the vegetable/seeds fats that are very harmful . . . and of course trans fats are the worst things you could put in your body
Hi Chris!!
I’m pretty new to all of this but I’m working on my dental gum health and am trying to incorporate more ADK vitamins into my mostly carnivore diet. I’m doing my best with food but I’m trying to supplement with Rosita Cod liver oil and was wondering what you think of Green Pastures x-factor High vitamin butter oil? Also, any thoughts on K2 dosages for children? Thanks!
A great resource and so well set out, thank you for making it available.
I remain unclear though on the bodies synergy between D3 and K2. Does K2 rob the body of D3 or otherwise affect absorption of D3. Can they both be taken together? I see that some of your recommended supplements contain both D3 and K2 which would suggest there is no conflict between the two vitamins?
Thank you,. This is the most explicit in depth article I have seen
.
Would you be able to expand on the origin of the various ‘High Dose MK4 supplements’ and whether they are natural, synthetic or synthetic/bio-identical ?
I need to take K2 MK7 as I have high level osteopenia but I also take an 81 mg aspirin a day as the hole in the heart that usually closes at birth left a very small hole. None of my doctors can tell me if there is risk in taking K2 MK7 while also taking low dose aspirin. Help!
Kim, I assume the aspirin you take is to counter blood clotting. That being the case, Vitamin K2 would not be contraindicated, as it has nothing to do with blood clotting (vitamin K1 would be contraindicated).
Is it safe to take K2 if you have Factor V Leiden? ( more prone to clotting)
Kathy, Vitamin K1 is involved with blood clotting,Vitamin K2 is not
I am 65 and have osteoporosis. In December 2019 I broke a vertebrae. That wasn’t diagnosed until the following February, which led to the OP diagnosis in March, followed of course by the pandemic. Tried Fosomax for 4 weeks. Never again. Since then I’ve used a natural approach, diet exercise and supplements, mixed results. I’ve started having really bad reflux this past year. I just now realize the supplements may have chick peas in them, which I have reacted to quite severely in the past. So now I’m taking a break from any supplements with K-2. Any suggestions? Thank you.
Hello! I read with interest your information on vitamin K in it’s myriad forms, and I think it is helpful, thank you very much! I am looking for a dose to treat a patient with recurring kidney stones. If that is a higher dose than the 100-200mcg/day, how long should the higher dose be maintained?
What do you think of HumanN D3.K2 supplement. I just ordered 1 jar but concerned its not what I need.
I had Pulmonary Sarcoidosis in the past and it is now in remission (after 2.5 years). I was advised by my pulmonologist to not take Vitamin D because of this illness as it can create hypercalcimia. When I read about K2, it’s always in conjunction with D3. My question is, can I take K2 alone without taking Vit D3?
Would you please help me with this confusing information about Vit. K, 1 and 2? One nutrition website I saw recently (run by a chemist marketing her own line of supplements) says they won’t sell a vit. d supplement with vit k added, because the two together will increase the amount of calcium in the body and vitamin k thickens the blood, because of the clotting factor. Another forum of hypothroid sufferers were sharing with each other that one of them was supplementing with K and she got a clot in her right coronary artery. Her cardiologist blamed the vit K. She said, “If you look it up you will find any form vitamin K causes clotting. It increases the fibrinogen level in your body and if you are prone to clotting it can be dangerous. I would suggest having your fibrinogen level checked. Mine was high with taking the K2..” After reading this, I asked a pharmacist about vit. K and he said he “doesn’t like it, because it thins the blood” (I guess he means it interferes with people on blood thinners).
Would you please clarify these confusing and contradictory claims? Clotting? Thinning? Are any of them at least partly true? I’ve been taking a D supplement with vit. K2, but it is only 10 mcg per capsule. I’ve been wanting to increase to at least 100 mcg, but these contradictory notions made me pause. Thank you very much.
Kristen, I can certainly understand you being confused, as there is so much conflicting “info” out there.
One point, I hope to clarify is that, vitamin k1 is involved in blood clotting not vitamin K2. Another point I want to make is that the popular chemist who has her own vitamin line says she won’t market a D3 supplement with added K vitamins, because “it would increase the amount of calcium”, it would “thicken blood”, “cause kidney stones”, Is not correct.
I suggest you take a look at out site (yes we sell our own Vitamin K2 product too)
https://www.v-k2.com/
I think you will find lots of very useful info
I found your site after becoming confused by lots of conflicting information about vit. D3 supplementation along with Vit. k2 MK7. I wrote out my questions and posted my comment, when I wanted to add another comment correcting something I said. Then my first comment, being moderated, had disappeared. I’m sorry.
I meant to say I have been using a 5,000 iu D3 supplement with 10 mcg of Mk7.
I found your site today because I was trying to resolve the confusion I have now about vit.K after reading so many contrasting opinions and information. I am chronically low in vit. d, so I had been supplementing with a 500 iu D3 / 10 mcg K2 mk7 capsule. Trying to understand how the two work together, and interested in preventing calcium from ending up in my arteries, I was about to increase my K2 to 100 mcg, when I found a few different sites saying contrary info. A popular chemist who has her own vitamin line says she won’t market a D3 supplement with added K vitamins, because “it would increase the amount of calcium”, it would “thicken blood”, “cause kidney stones”, etc. “you only need D to increase D”. A thyroid forum had several people sharing that vitamin k causes blood clots, because of fibrinogen levels. Another author talked about carboxylating MGP. A Portugese doctor treating patients with high dose Vit. D therapy and vit. K stipulates avoiding all calcium foods while taking vit. D and closely monitoring calcium levels with blood and urine tests… Others wrote horror stories about damaging their kidneys from high doeses of vit. d, but they didn’t mention if they had taken vit. k.. I am paralyzed now and afraid to eat or take a supplement. Was any of the above true? How can I know? Every person who writes on the internet writes with authority yet completely contradict each other.
When doctors or nutritionists advised me to supplement with vit. D, most of them said nothing about K, and other than measuring my D levels to see if the supplementation had worked to improve that level, none of them told me to monitor calcium levels.
I would dearly appreciate some clarity here. Thank you.
Thank you for all the challenging questions. Yes, between promotion of commercial vitamins, medical opposition to vitamin use, and simplistic thinking there is more confusion over the science of the vitamin K & K2 forms than just stupidity, it is driven at times by diverging fiscal interests. You literally have to be a better scientist than the people you are reading or talking to. You have my every compassion in this.
First, vitamin supplements are safe. Most years NO deaths are accorded to vitamins in toxicology data reports with vitamins being ten times safer than the risk of being hit by lightening and a thousand times safer than taking acetomeniphen.
The medical references on vitamin D are blazingly unscientific with Institute Of Medicine pronouncements of 600 IU daily doses being without scientific credit when compared with calculated 8895 IU and 9122 IU daily doses from the SAME Institute Of Medicine data that were published in two peer reviewed Journals. The IOM has been asked multiple times to review their numbers by research scientists. If you get your blood level for vitamin D tested, aim for a 50 to 70 ng/ml blood level for normal health, up to 200 ng/ml for reducing autoimmune symptoms. Generally start with the 10,000 IU and then adjust as needed. Doses under 30,000 IU are generally safe especially if some Retinol vitamin A is taken as low Retinol is a cause of kidney stones, not vitamin D. Doses above 30,000 IU should be managed by a physician who is trained in the Coimbra Protocol for high dose vitamin D used to suppress autoimmune conditions.
Cofactors that work with vitamin D are 200-600 mg magnesium, 12-30 mg boron, 15,000 IU Retinol vitamin A, 20-30 mg zinc, and MK4 vitamin K2.
There is NO optimal dose of vitamins D and K2. Why? Personal doses of vitamin D vary by a factor of ten, making proportioning of the K2 impossible. The need for vitamin K2 varies from zero to 45 mg a day for serious cases of artery calcification and bone loss. The body makes MK4 vitamin K2 by converting vitamin K1 with MK4 production falling off with age. Those under 30 don’t need MK4 unless they are medical cases, but above 40 or 50 years an MK4 supplement is very useful. The MK7 form of vitamin K2 is made by bacteria, not the human body so we are badly adapted to use MK7 and it is much less effective than the MK4 vitamin K2 which is identical to what all animals make. The 100 mcg of MK7 vitamin K2 is ok as long as you are not part of the 10% of people who get anxiety, sleeplessness, and a thumping heart beat from taking it. Doses of the MK4 form are 1 to 5 mg for healthy people. The MK4 helps the body make its Matrix GLA protein work to remove calcification from the arteries and makes the Calcitonin with to rebuild bones with more tissue strength and better microstructure.
Taking MK4 and MK7 is completely safe, no extra clotting has been reported at up to 135 mg per day. The same for regular vitamin K, it can potentiate fibrogen clotting protein up to 100%, but no increase past 100% is possible.
For information on taking calcium, only 500 to 800 mg of calcium is needed with higher blood levels of vitamin D. The Coimbra Protocol calls for strong calcium reductions but only at medically high vitamin D intakes.
So now you know that doctors have only a few hours of nutritional training and much of that is obsolete or even unscientific in places. Look up Life Extension magazine which works hard to get good references in its articles and treats Nutrition with the good science it deserves. Dr Andrew Saul at doctoryourself.com is a good source as is vitamin D wiki.
Hi David, your reply is by far the best and easiest to understand. I too have been confused about what to do about taking Vit D and K2. Thank you again.
Presently, I am taking Synergy from Pure Encapsulations.
It has K1 500 mcg, K2- 1000 mcg MK-4, MK-7. 45 mcg and the mfr just added to this formula D3 1000 in it.
I am also taking Dr. Mercola’s Vit D3, 1000.
So a total of 2,000 of Vit D3.
I am curious do you have a K2 that you may prefer and can suggest? I always try to look for clean vitamins with good fillers or no fillers.
I have High Fibrinogen, which was over 600, and brought down to 346 with taking Inflamazyme.
Your help would be greatly appreciated.
Thank you so much,
This comment is a general one for this topic and not necessarily directed at David. I interjected here only because I couldn’t figure out where/how to post an independent post on this page, although there is a statement by David as well as others that I wanted to comment to and seek alternate opinions of, specifically regarding to mk7 being converted to mk4 and one other note.
Per a number of http://www.ncbi.nlm.nih.gov/pmc/articles as well as this one (https://nutritionj.biomedcentral.com/articles/10.1186/1475-2891-11-93) they state that mk7 is indeed converted to mk4 and that mk4 supplementation had no effect or increase in blood levels of mk4. This article (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8483258/) also directly mentions MenaQ7 which is supposed to be a 100 percent Trans form of K2 and derived from chickpeas vs natto eliminating any soy or Cis form concerns. It’s also been noted several places that mk4 is the form most used and accessible by the bacteria h.pylori and that those with h.pylori overgrowth would do best not to use mk4.
I, like many others am very confused by all of this and curious if mk7 actually causes palpitations and insomnia or are those due to other factors and where is the scientific data vs the subjective users’ statements? There is so much speculation and so many financially incentivised and biased articles that I tend to lend my belief to the scientific based organizations and data.
There’s a warning to avoid K2 supplements if on anti-coagulants, specifically cumadin/warfarin, but I was unable to find any specifics with respect to Apixaban/Eliquis. which is an anti-coagulant but works differently. (I take it for paroxysmal AFib.) I stated taking the one Innovix 100/500 soft gel 10 days before a PT-INR test and the result was within range (14.3 sec PT and 1.1 INR), but do not know if that means K@ is safe for it. I assume the concern is that K@ might adversely affect coagulation times or is there some other concern?. Can you point me to any specifics for Eliquis and K2? (My nutritionist and my nephrologist are unfamiliar with K2..) I see my cardiologist on 3/19 and would like to discuss. Also regarding the Innovix, your recommendation implies taking one pill every 3 days. to get to your recommended standard daily amount. With this regimen, do both MK’s linger long enough to last three days?
Jarrow Formulas makes the MK-7 softgels in 180 mcg per softgel (MCT and olive oil) as well.
https://www.iherb.com/pr/Jarrow-Formulas-MK-7-Most-Active-Form-of-Vitamin-K2-180-mcg-60-Softgels/86135
I’m getting those for my mom, who seems to have a severe K2 deficiency at present since taking calcium is apparently giving her hypercalcemia where she can’t keep her balance when walking.
some other interesting options to consider are
Doctor’s Best Natural Vitamin K2 Mena Q7® plus D3 — 180 mcg – 60 Veggie Caps (1000 IU D3 + 180 MK-7)
https://www.vitacost.com/doctors-best-natural-vitamin-k2-mena-q7-plus-d3
and
TrueVantage Vitamin k2 MK-7 Supplement 180mcg (which is cheaper but comes in dry capsules)
https://www.amazon.com/Strength-Supplement-Cardiovascular-Absorption-Arteries/dp/B01FIR33FS
am trying to find out more about sourcing and form of the MK-7 in Bronson Vitamin K2 (100 mcg MK-7)
https://www.amazon.com/Vitamin-MK-7-Menaquinone-100-Serving/dp/B07S417XN6
Lastly, if you need extra D3 and prefer liquid drops (I sure do, except maybe for travel, swallowing lots of pills gets tiresome) there’s
NOW Supplements, Liquid D-3 & MK-7 with 2,500 IU Vitamin D-3 & 100 mcg Vitamin K-2 per 5 drops
https://www.amazon.com/gp/product/B07H1V2KM3/
[another vendor, Protocol for Life Balance, offers an identical product at slightly higher price in Fullscript (if you’re a Masterpass subscriber)]
Taking 5 drops of that plus a drop of the Thorne D/K2 (with MK-4) provides 200 mcg of K2/day + 3,000 IU of D3, which should be perfect for my needs and provides half of the K2 as MK-4 and half as MK-7.
none of the products in those links contain BOTH mk7 and Mk4.
I would suggest vK2, which contains pharmaceutical grade MK4 (5mg) and MK7 (100mcg).
Margaret, I apologise for my seemingly late reply to this post of yours, as it was from Feb, 2021, and just appeared in my mailbox, being now Sept. 2021.
You wrote “I’m getting those for my mom, who seems to have a severe K2 deficiency at present since taking calcium is apparently giving her hypercalcemia where she can’t keep her balance when walking. ” referring to a form/product of k2 in that post. Since I don’t know the actual context for your comment, please forgive me if I’ve missed any details previously or consequently presented about your mother.
FIrst, if I were you, I’d ask, (not a doctor or even as medical professional), has your mother’s hypercalcemia been documented as consistently over a level of 10 mg/dl for serum blood calcium, assuming that she is at least 40 years old? If this is the case, then I’d recommend looking at websites about hyperparathryoidism. parathyroid dot com is comprehensive.
Since excess vitamin d has been known to boost calcium levels too high in some people (perhaps vitamin k2 deficient, but not necessarily!), you’d want to rule that out also (vitamin d being known to enhance absorption of calcium from our guts) as a possibility. I’d carefully the assumption that her problem is a deficiency of vitamin k2 (although a deficiency might be true, esp. if much older and with some issues in converting vitamin k1 into vitamin k2, as is probably more common than accepted due to high levels of potential environmental complicators such as glyphosates that are difficult if not impossible to measure in our bodies and our food and water, and yet might have a detrimental impact on the necessary bacteria in our bodies, and other nutritional factors that could interfere with that conversion).
If the usage of vitamin k2 has reversed your mothers hypercalcemia, please let us know.
I make sourdough bread and natto at home but my kids won’t touch the the natto. Might it be possible to mix some natto into the dough, let it ferment/prove and the bacteria replicate (usually I prove for 8-12h) and then bake it? Would the K2 be destroyed by baking?
also it’s “YoungGlo Research” not “Young Life Research” and while those are the cheapest per mcg of MK-7 when bought in 4-packs and the other brands aren’t on sale, I don’t like that it comes in a translucent blue bottle, when because K2 is very light-sensitive it should be packaged in an amber or opaque bottle.
I am pretty confused. In your opinion what brands of K2 have the best balance? I am most concerned with quality and taking the right balance of MK4 & Mk 7. I especially take it for my bones. I was taking the Synergy K, but now I will stop after you explained why it is not a good balance and that K1 is not suggested. I truly appreciate your help.
Aside from vK2 containing an optimal amount of both MK4 and Mk7, it is also pharmaceutical grade, characterized by its yellow color. Unlike most other vitamin K2 products, the ingredients for vK2 are NOT sourced from China (they come from Europe).
Janel, please search for the section above titled “The Three Best Vitamin K2 Supplements”. At the bottom of that section you’ll see a green outline button thingy with lighter green print “Click here for a comprehensive review of supplements” [I wish that Chris would make these solid color with white lettering, so that these are easier to see/read and harder to miss].
That section will expand to show a bunch of additional text. Read what Chris has to say about the Life Extension Vitamin K supplement in that expanded section and too much K possibly overtaxing the antioxidant system.
Also look at the section titled “Hypothetical Side Effects of High Doses” and read the expansion/detailed explanation for that. Then you will understand.
The Synergy supplement might be good for someone who won’t eat many green and yellow vegetables and doesn’t get much vitamin K1. That’s probably not you. I logged all the foods I eat into the daily diary in the Cronometer app, and discovered that on average, I get more than enough K1 from my diet (the app doesn’t break it down between the two types of K, but I know that generally speaking except for natto the plant foods are providing K1 and the animal foods are providing K2). I do eat natto, but getting the organic natto is expensive and I don’t eat enough animal food (and am on a diet that restricts dairy for the time being), hence I’ve chosen to get much of my K2 from supplements and will plan to continue to supplement MK-7 even after I hopefully can resume eating dairy.
Unless you have some kind of identified genetic dysfunction that you have to compensate for, generally speaking, everything in moderation, eat a wide variety of foods, not overdoing any one thing is best and safest.
Thank you. Do you like any particular brand of K2? I do have to avoid some veggies, due to oxalate issues. I do eat Brocolli & Cauliflower but that is about it in veggies. Your opinion is appreciated and your help in understanding how to navigate the info here is extremely helpful.
See my comment posted down a ways earlier on this topic. After I posted that I also saw that some other companies make MK-7 capsules sold on Amazon. You want to look for one that says it consists of the product made by Menaq7. Anyway, since Chris recommends 200 mcg total of K2 per day, and a mix of MK-4 and MK-7 as they seem to act somewhat differently in the body (though some people seem to be sensitive to MK-7 for some unknown reason), I’m supplementing with 100 mcg of each and that should be good enough. There are also supplements with 180 mcg of MK-7 as well that claim that 180 mcg is what’s been studied to work well.
There are cooking techniques you can use to reduce oxalates in veggies. For example, in traditional Japanese cooking some green veggies are parboiled in salted water and the water is then drained. You can search online to research how much that helps for things like spinach etc. It helps a lot with taro.
I recommend you track your food intake for at least 3 days in the Cronometer app, to get a sense of how much K1 you get through diet. But if you don’t have any issues with blood not clotting well you may be fine as well as K1 is concerned.
The ultimate proof is how your next bone density test comes out (while keeping in mind that K2 is just one factor in increasing bone density).
I am guessing that future studies will find that the MK-10 and MK-11 in pork does get converted to the other forms, because the long-lived Ogimi people in Okinawa eat moderate amounts of pork, but it doesn’t look like they eat much natto.
There is a lot of speculation regarding optimal K2 dosage. Obviously more studies are needed. However, I think its safe to say that Mk4 and MK7 are NOT dose equivalent. I do not consider it reasonable to split the numeric value of a recommended dose of mk7 into MK4 and MK7 components to that value. They are NOT dose equivalent. Their respective doses differ by an order of magnitude. MK7 dosage are generally expressed in mcg’s, while MK4 dosages are generally expressed in mg’s.
It seems that the Nested Naturals K2 product is discontinued, and now they only offer a K2 product that is combined with 5,000 IU vitamin D unfortunately.
I use Synergy K2, which combines MK4 & MK7. Not sure if this will help you.
thanks but that one looks way too imbalanced. Way too much MK4 (1 mg) and not enough MK7 (45 mcg), plus it has a lot of K1 which I get plenty of from my diet, and Chris Masterjohn cautioned getting unnecessarily high amounts of Vitamin K may be harmful.
thanks Jan but that one looks way too imbalanced. Way too much MK4 (1 mg) and not enough MK7 (45 mcg), plus it has a lot of K1 which I get plenty of from my diet, and Chris Masterjohn cautioned getting unnecessarily high amounts of Vitamin K may be harmful.
I had good results in reducing artery calcification with the similar Vitacost advanced K complex with 1.3 mg of MK4 vitamin K2. That is actually a small amount, optimal doses for MK4 in research run up to 45 mg per day. I’ve seen research with lower doses of 5 mg to 15 mg daily giving good results with bone or artery health improvements.
The use of MK4 is safe because the body discards what it doesn’t need, so doses up to 135 mg per day have shown little in side effects. In youth the body makes enough MK4 from vitamin K that supplements are not needed.
The MK7 is generally used in much smaller amounts. It is made by bacteria so is not a natural part of body chemistry like MK4 is.
I just had a coronary calcium San with score of 60. Previous ones had been 302 and 319! I’ve been taking 30mg the last two years of relentless bit k2-4. Is that really possible ??I don’t understand how it went down that much. Happy if it’s right.
what I settled on was one drop of Thorne K/D2 and one tablet of Source Naturals Vitamin K2+D3, plus one drop of Now Extra Strength Liquid Vitamin D-3 to get sufficient D3 as needed. This gets me 100 mcg of MK4 and 100 mcg MK7 each day. I see that the Doctor’s Best, Natural Vitamin K2 MK-7 with MenaQ7 is a slightly better buy for MK7, as is the Sonora Nutrition Vitamin K2 that Chris lists in the expanded Comprehensive Review section.
though at this very moment iHerb seems to be having a sale on the Source Naturals so that it is actually cheaper at present than the Doctor’s Best
100 mcg of MK4 is wowfully inadequate. Our product (vK2) has 5mg MK4 and 100mcg of MK7, which is a much more reasonable dose
I tried to read through the whole post but it’s quite long. Is there a suitable Vegan MK-4 / MK – 7 supplement please? I am kind of overwhelmed with choice and opinions and have no way of measuring validity. Thank you so much.
vK2 is a good option, contains both MK4 and MK7 (pharmaceutical grade) in a vegetable capsule
My severe shortness of breath, dry cough, low energy, fatigue, chest tightness and others gradually disappeared. Visit Akanni herbs clinic official web page Akanniherbalcentre com. This COPD treatment has improved the quality of my life greatly, i breath much better and It feels comfortable!
k2 180 mcg, together with d3 5000 iu ,together with angstrom ionized magnesium ,or magnesium malate/glycinater 800-1600 mg,
I’m reading that D3 and K2 should not be taken at the same time. Have you researched this issue? Conclusions?
Where did you read that Bonnie? I’ve never seen that anywhere and given the different actions of D3 and K2 I can’t see why it would be a problem. I think that’s probably one of the myths that float around the internet such as “don’t shower after sun exposure ‘cos you’ll wash off the Vitamin D”.
Bonnie . . . Where did you read vitamins D3 and K2 should NOT be taken at the same time? I’ve never seen any studies that suggest that. Quite to the contrary, they SHOULD be taken together. Vitamin D stimulates the production of gla proteins, which do not do anything, unless activated by vitamin K2. In fact, as the dose of vitamin D3 is increased, the demand for Vitamin K2 increases proportionally.
Hi. I have read the SAME. Not that D3 should not be taken, it definitely should, but to not take it at the same time as the K2. I believe I read it in a book called REBUILD YOUR BONES, The 12-week Osteoporosis Protocol by Mira and Jayson Calton, PHD. I, too, would love more insight into the issue.
I’ve also read the same….NOT to take D3 at same time as K2, though one should be taking both of them…just not at same time. I think I read that in a book by Mira and Jason Calton, PHD. Book is Rebuild Your Bones, the 12-week Osteoporosis protocol.
Dicksie . . . I have not read “Rebuild Your Bones”, but i did look it up on amazon, and the preview and/or table of contents makes no mention of thesis you have asserted. I have also searched the authors in pubmed, but came up empty. They have not published any clinical trials on this topic. I am not going to say authoritatively that this thesis is wrong, but Ive not seen anything to make me believe it. I can not imagine, what the rational might be, considering a) vitamin D3 needs to go through 2 hydroxylations before it becomes active and b) vitamin K2 does not interfere with those processes, which take care in the liver and kidneys respectively c) Vitamin K2 has a relatively short half life. So If not taken at the same time how else would they able to work in tandem. If you find any studies to substantiate this thesis, I would be very interested to know of it, but as I already said, I’ve never seen any such studies
Thanks, Eric! I have not read it elsewhere, either, but did see it in that book…I think that is where, anyhow. I will dig the book out and see if, indeed, that is the case. I, too, TRIED to search farther on it, but found nothing. Appreciate your input. Apparently Bonnie must have also read it somewhere….though that does not make it ‘so’ just because someone (though he is a doctor if it is from that book) is stating it. Sorry about my double post. I could not tell the first one went through 🙂 It absolutely is a ‘pain’ to TRY to take them separately since I take supplements both morning and night…. Appreciate your response.
Yes, the Calton’s are promoting this concept. They suggest that both K2 and D3 are competing for the same receptor sites, so they should be taken separately over the course of the day. Happy to see it disproven, but I see this idea popping up all over the place online.
See the webpage for the reference #16
https://www.caltonnutrition.com/vitamin-k-the-right-way/
which brings you to the following:
https://pubmed.ncbi.nlm.nih.gov/25442537/
Fat-soluble vitamin intestinal absorption: absorption sites in the intestine and interactions for absorption.
Abstract
The interactions occurring at the intestinal level between the fat-soluble vitamins A, D, E and K (FSVs) are poorly documented. We first determined each FSV absorption profile along the duodenal–colonic axis of mouse intestine to clarify their respective absorption sites. We then investigated the interactions between FSVs during their uptake by Caco-2 cells. Our data show that vitamin A was mostly absorbed in the mouse proximal intestine, while vitamin D was absorbed in the median intestine, and vitamin E and K in the distal intestine. Significant competitive interactions for uptake were then elucidated among vitamin D, E and K, supporting the hypothesis of common absorption pathways. Vitamin A also significantly decreased the uptake of the other FSVs but, conversely, its uptake was not impaired by vitamins D and K and even promoted by vitamin E. These results should be taken into account, especially for supplement formulation, to optimise FSV absorption.
Unfortunately, the full article is available online at ScienceDirect only if you have some sort of institutional access. Perhaps it is for sale too, and I’ve missed the link.
I am taking 50mcg of Vit D3 every other day, and a daily dose of 200 mcg of K2-7 to avoid my blood pressure to go up. It seems that Vit D3 accumulates over time and affects my blood preassure. Also, eat some almonds along with Vit D3 for magnesium.
When my K2-7 and Vit D3 are “balanced” I do not need to take my blood pressure medicine. That is my challenge on how to keep this balance. Any Comments or suggestions?
Bonnie . . . What receptor sites are they referring to? The receptor sites for vitamin K2 are on the gla proteins (VKDPs) themselves. That is where they the VKDP activation takes place. Vitamin D3 is involved in production of these gla proteins and as far as i know, this production is not at all hampered by vitamin k2. Furthermore, vitamin D3 is hydroxylated (to become the biologically active form of vitamin D) in the liver and kidney. I am unfamiliar with any research that suggests vitamin K2 competes with vitamin D3 for receptor sites in the liver and kidney.
In other words vitamin D and vitamin K do not have common receptors, so they do not compete for receptors. If you find any info that refutes my point, please share it. I could be wrong, but i do not think I am
Let us look at this logically. Vitamin K2 and Vitamin D3 are both fat soluble vitamins found together along with Preformed Vitamin A as well as minerals like magnesium and calcium in healthy animal fats that have sustained the healthy bodies of traditional cultures for generation upon generation.
Butter, lard, tallow, cream, cheese ghee all have K2 and D3 together. If one consumes too much fat soluble vitamins the body stores them in the body fat for use later.
Conclusion: Logical Retroductive Reasoning shows that there are no issues taking D3 and K2 together.
If one consumes too much fat soluble vitamins the body stores them in the body fat for use later.
I don’t have a clue what retroductive reasoning is, logical or otherwise, but you 2 sound like you know what you’re talking about.
All I can say is that the product in question, nutreince, has a miniscule amount of K: 40mcg each of V1, 4, & 7. I’m not qualified in anything, but based on everything else I’m reading, that sounds just about meaningless to me, whatever other qualities the product might have.
Can I take Vit D3, K2 with Vit A? Do I need to take Magnesium the same time as D3 and K2? Can I use Magnesium L-Theronate?
https://www.youtube.com/watch?v=6TilqdPb-FI
many interesting comments on this video such as….
“I take vitamin D3 with K2- I heard you need that combination for absorption”
It is the other way around. They should be taken together which is why some supplement of D3 are combine with K2
Thanks so much for this comprehensive article! What are your thoughts on Jarrow’s K-Right supplement?
Jarrow’s K-Right contains Mk4 and MK7, but only contains 1500 mcg MK4 (not nearly enough). It also has vitamin K1, but it is not needed so I’m not sure why its included.
Vk2® which contains 100 mcg (.1 mg) of Mk7 and 5,000 mcg (5 mg) of MK4. Most importantly both are pharmaceutical grade (with the characteristic yellow color) and sourced from Europe. If the brand of Vitamin K2 you take is white, then it is not pharmaceutical grade and is likely sourced from China.
This really made me pay attention. The writing skill alone kept my interest. Thank you for sharing!
Obrigado!
Aprecio muito a generosidade e frontalidade.
Especialmente em tempos de Covid, os teus escritos são uma luz abençoada para muita gente atónita que se desviou do equilíbrio da natureza. Eles estão aterrados com as comorbidades, mas sem o saber, vão destruindo a ‘tua’ vitamina K.
Como eu te entendo! Obrigado.
Hi Chris–Can’t thank you enough for your exhaustive and trustworthy research. You’ve been an invaluable resource! I was diagnosed a couple years ago with histamine intolerance (history of migraines, hives, rashes, other symptoms). LOTS of research and staying as low-histamine as possible with diet, meds (no NSAIDS, for example), has helped. I’ve been taking K2MK-4 daily to address healthy calcium absorption, but have avoided MK-7 because it’s from fermented sources. Fermented foods are a known histamine trigger. So does that make K2MK-7 supplements off limits? If so, what to do? It’s a very important vitamin.
So, question: I have a hereditary clotting disorder, “heterozygous prothrombin G20210A” if you know what that means, which gives me slightly higher risk for abnormal clotting.
Is K2 of any description safe to take with this? I already take D3 along with magnesium and would like to add K2 but am afraid of causing arterial or venous thrombosis/thromboembolism. I’ve already had one PE with apparently no precipitating DVT, and do not want to go through that again.
can you review tri-k made by designs for health?
Melodei, tri-k has vitamin K1 (which you do not need) it does have some vitamin k2 (MK4) but only a small amount (500 mcg, which is .5mg). It has no MK7 at all. Its very expensive too. vK2 contains both MK4 (5 mg, which is 10x more than what tri-k contains) and MK7 (100 mcg)
I wish you could replace or add measurement symbols that are used in the United States so I could better understand it in context of your information. I am retired and have hard enough time when I read it the U.S. weight symbols. Thank You
I agree! Always causes confusion, hope the book will be in US format.
Has anyone has taken vitamin K2-7 along with garlic that could share his experience? Also what is the optimal doses for K2-7 to unclog arteries?
I started taking K2 (Carlson MK-4 5mg/day) about 3 weeks ago, along with magnesium glycinate (360 mg/day — broken up 3x/day), vitamin D3 (2000 iu) and also I will take some of the fermented cod liver oil/butter oil mixture (maybe 2-3 capsules a day).
I was having trouble with my teeth chipping or developing white spots; this still seems to be going on (I notice new chips or spots everyday). I even had some gum bleeding when flossing (I’m a regular flosser and that hasn’t happened in years!) I’m not sure of course if those problems would have developed anyway. Could I be doing more harm than good? Maybe it’s too much K2?
By the way, for diet, I do eat milk and yogurt, also cheese (I even focus on Jarlsberg, Muenster and Gouda to try to get the MK-7). It’s possible it’s still not enough calcium compared to the supplements though.
I’m no expert on nuthin’, but . . . I don’t think 5 mg is too much. I’ve been taking 25 mg/day for about 2 1/2 months, and nothing bad has happened. Also, I’m not sure 3 weeks is long enough for anything bad to happen, although in a world of uncertainty I guess just about anything is possible. Have you asked your dentist what could cause your symptoms?
I did ask, the best thing we could come up with was I was grinding my teeth and chewing on my nightguard, putting pressure on the teeth. I’m going to get Invisalign to fix the bite and help with the grinding.
I had my blood levels checked as well, calcium is okay (9.7 mg/dL), vitamin D is borderline low (29.3 ng/ml). I think I need to raise my vitamin D a little and if I’m taking vitamin D, then I need to also continue with K2. Hopefully that helps with my teeth issues over time, since I’ve heard so many anecdotes about how much it helps.
Again, I’m no expert . . . but I don’t think 29.3 is borderline–it’s low. I read some supplement seller’s comment once that a good target range is 50-80, so I wouldn’t be shy about getting it up. And you said ‘D;’ I assume you mean D3.
Chris has written before that levels maybe should be more like 30-35, and that it could also depend on your race.
https://www.westonaprice.org/are-some-people-pushing-their-vitamin-d-levels-too-high/
Of course, these things are all in balance with each other. I feel like I’m still trying to figure out a good balance of K2, D, and A with each other. I hope to find it soon, and also to experience some of the improved health benefits that other people have seen.
I’ve continued on with the K2 as well as the other supplements. I also added some occasional vitamin C hoping to deal with the gums. It’s been nearly two months now.
Yet I noticed another white spot on one of my teeth and there even seemed to be some brown next to it.
I don’t know if I’m just noticing things that were already there from before, or if new problems are really cropping up. I even contemplated that the spots were a sign of healing — maybe my teeth are changing color as they absorb minerals. Then I notice it because it changed.
I feel like the only thing to do is to continue with the protocol, which seems pretty balanced in terms of getting all the fat soluble vitamins. Diet-wise it seems pretty good, with yogurt and beef liver and a variety of vegetables, and I’ve been getting more sun.
It might be the case that it just needs a good 6 months before the positive changes become noticeable. I don’t know because a lot of people reported whiter teeth and no tartar after only a week or two, but so far I haven’t seen this happen.
Abby, I’m replying to your comment of 7-16 below my comment since there’s no ‘Reply’ option below your comment. (But it’s looking like this comment might end up in the right place anyway.)
It’s not clear from your initial comment if your teeth problem began before or after you started taking K2. If you stop taking K2 and the problem goes away, I guess that settles the issue.
You might want to get an opinion from a second dentist. My dentist’s receptionist is pretty knowledgeable, so you might find a similar situation where you don’t even have to visit the 2nd dentist.
Good luck since nobody here seems to be able to be real helpful.
Not sure where the reply will go 🙂
I had teeth problems before– I chipped a tooth back in January and noticed a decalcified spot. I started to try to fix these issues in March but didn’t learn about K2 until May. I did start on cod liver oil in March though.
I also started feeling like my bite was bad, and that I kept tapping my teeth against each other when eating or talking. I felt extremely uncomfortable and a sense of something being wrong.
Anyway, I thought taking K2 would help me with these issues. I started examining my teeth more thoroughly with a flashlight after I started taking the K2. I noticed a white spot a few days after I started. Then a few days after that I noticed some chips. Now a few weeks later I notice the new white/brown spot.
I was hurting before, which is why I started the K2 in the first place, so it’s possible these problems were already there/already in development and only noticed by me later. It’s impossible to say.
It does seem like maybe I should pause the large dose K2, and only take what I get from my cod liver oil/butter oil mixture and also from food. I think part of the reason I haven’t stopped yet is because I was concerned about vitamin D3 — but since my levels are still low, perhaps it is okay to pause for a few weeks, anyway.
Thanks for your help vanp, I think it is just a confusing problem. I have an appointment on Monday (regular doctor, not dentist) so I might ask then as well
You should ask the doctor, of course, but don’t be surprised if he don’t know squat about any of this. I’ve been taking Green Pasture’s butter oil and cod liver oil pills for years with no problems.
29ng/ml is not “borderline low” regardless of what your doctor or dentist tells you, it is VERY low. This is just another example of where mainstream medicine has set the bar for vitamins and minerals way too low. I suggest you look at this blog post by the late Dr Robert Heaney, one of the foremost researchers on Vit D and osteoporosis:
http://blogs.creighton.edu/heaney/2013/04/08/defining-normal-part-two/
When your body is not getting enough calcium from the diet it needs to increase the supply NOW or you die. Consequently a signal is sent to the parathyroid gland to increase the release of parathyroid hormone (PTH) to break down bone (and presumably teeth) to provide the calcium necessary. Chronic Ca deficiency and elevated PTH causes osteoporosis. I’d think it’d also weaken your teeth. In order to absorb Ca from your diet you need adequate Vit D.
Look at the graph of PTH vs 25(OH)D (the active form of D). Each circle is an individual patient’s result and the red line is a mathematically calculated “line of best fit” to the data. The point where the line flattens indicates where on average a further increase in D levels does not provide further benefit in terms of PTH and bone loss, though obviously there is a lot of individual variation. Dr Heaney writes:
“The figure shows clearly the expected high levels of PTH at low vitamin D status values, with PTH concentration falling and becoming essentially flat as vitamin D status rises to levels in the range of 125 nmol/L (50 ng/mL). Exactly the same relationship is exhibited in a report from the National Health and Nutrition Examination Survey, involving a population-based sample of over 14,000 individuals. Both data sets found almost exactly the same vitamin D status level, above which PTH fell no further.
Because there are many factors that influence PTH concentration beyond vitamin D status, this approach will not work very well in determining individual requirements of calcium or vitamin D. However, it does work at a population level, as the graph shows. The point at which further increases in vitamin D status produce no further decreases in PTH concentration [i.e., a plot of PTH on 25(OH)D is flat] defines the PTH set point for both calcium and vitamin D. This is the point around which the body can exercise its regulatory control of serum calcium concentration with optimal capacity in both directions. The need to compensate, and the duration of adaptation are minimized. Such a value would seem to be a reasonable estimate of optimal vitamin D status, and therefore an indicator of the vitamin D requirement.” Dr Heaney’s average optimal D level of 50ng/ml compares with Dr William Davis’s recommendation of 60ng/ml for heart health.
To ensure adequate health of your bones and teeth you need:
1) a calcium-rich diet
2) enough vit D to absorb that calcium
3) vit K2 to direct Ca to bones and teeth
4) weight bearing exercise to build bone
It sounds like you have 1 and 3 covered but possibly are not getting enough D.
Check that your results actually are in ng/ml and not nmol/L – 29nmol/L is severe deficiency- and that they are measuring 25(OH)D the active form. Your level of 29ng/ml equates to about 75nmol/L. As you can see from the graph 75nmol could be either high or low depending on the individual. Get a PTH test to determine your levels. A bone density scan will determine whether you have a degree of osteoporosis. If so DO NOT allow your doctor to prescribe bisphosphonates (eg Fosamax or another brand name). These drugs show better scan results but don’t reduce fractures. Instead, make sure your C, D, K2, magnesium and protein levels are high and walk, run or skip rope. All of Dr Heaney’s blog posts are well worth reading.
I want to make a correction to Stuart’s post.
25(OH)D is NOT the active form of vitamin D3.
Actually it is 1,25(OH)D which is the active form
25(OH)D (calcidiol) is however, used to measure vitamin D status, even though 1,25(OH)D (calcitriol) is the active form.
I think it’s important to remember that your optimal level of vitamin D3 intake depends on your vitamin K2 status because if that is insufficient, high levels of vitamin D3 intake, which would otherwise be healthy and provide enhanced immune system function, are likely to cause abnormal calcifications in your arteries and other soft tissues.
Yes, your D3 is too lower. I would double what you are taking and have your D3 tested again in three months. So if you are taking D3 1000 IU, I would take 2000 IU. I see wrote this in June so I hope your levels are tested again and then go from there.
James Kantor, Raleigh, North Carolina.
I posted a lengthy reply to this post several days ago and it still hasn’t appeared. System admin please check your Spam folder. Thanks
Has anyone ever notice facial difference taking vitamin k2 mk4. I have read on forum peoples faces change from taking it. they notice are more prominent cheek and jaw development. This from megadosing it. Unfortunately no one ever post photos so its hard to tell if its true or not.
Never heard of that. What would be considered “megadosing?”
I read that mk4 can affect jaw development in embryos and infants, so that the jaw actually accommodates all of our teeth. Wisdom teeth pulling would be unnecessary if we were given adequate amounts of mk4. EMU OIL for the win.
Awesome post! I so learned a lot from this especially about vitamin k2. Thanks a lot for posting!
Sure, Emma, Vegans are also deficient in Vitamin K. You will probably not feel any signs, even though the arterial linings and heart valves are likely to build up calcium. VK2 is shippable to Australia. I hope this knowledge will be of use to you
Thanks so much for this information. I have to let you know I concur on several of the points you make here and others may require some further review, but I can see your viewpoint.
Hey, what do you think about Pure Therapro? https://purethera.com/products/vegan-d3-k2-liquid
I want to start supplementing my 4 year old’s diet with K2, but can’t find any full spectrum except this one and the Innovix – not sure I can give him that because of dosage and difficulty swallowing. Not sure about the reputability of Pure Therpro but I was happy to see a full spectrum K2 in liquid format.
I’d appreciate any insight at all 🙂
Holly
Pure Therpro only has .5mg of MK4, while vK2 has 5 mg (10x more).
Right, but vK2 is a capsule, which my 4 year old can’t down. So I just wasn’t sure if you had any opinions on the brand, Pure Therapro! Thanks!
what do u think of this supplement?
https://www.amazon.com/Advanced-Peak-Performance-Supplement-Vegetable/dp/B075R56QCQ/ref=as_li_ss_tl?s=hpc&ie=UTF8&qid=1540949878&sr=1-1&keywords=peak+performance+a+k&linkCode=sl1&tag=lab02-20&linkId=29895908fbd5dbc90b338666b6252e8c&language=en_US
i have a low vitamin D (13ng/ml)
Thanks,
Shalom
I’m no expert on this stuff, but the MK-4 dosage is miniscule–probably not worth taking. Also, I may have missed it, but it doesn’t seem to say “no soy.” Not sure how big a deal this is.
Like Vanp suggested, the amount of MK4 contained in that product is so small as to be useless. It also contains Vitamin K1, which most people do not need at all
I have a very low vitamin D (13ng/ml ) and im overweight (150kg)
what would be the best K+D supplement for me?
Shalom,
NHS Global Distributors, Inc sells 2 products that may be of interest to you.
vK2 contains 5mg of MK4 and 100mcg of MK7 (both are pharmaceutical grade)
Dmax contains 5,000 iu of Vitamin D3
The fact that it helps prevent kidney stones, is motivation enough for me to start consuming more! Thanks for the very informative run down
I would be so grateful if you could review this K2 supplement from Gundry MD https://gundrymd.com/supplements/essential-k2/
Is it non GMO and soy free?
How is it sourced? If synthetic, is it bioidentical?
Thank you SO much for your expertise and guidance.
Their website does not provide much info. I see that it contains both MK4 and MK7 but only 100mcg of MK4, which is a tiny amount. (Our Vk2 product contains 100 MG of MK4)
I also see that it contains magnesium stearate, which I consider a substance to avoid
“Our Vk2 product contains 100 MG of MK4”
Shouldn’t that be 5MG?
Yes, Vamp . . . my Bad . . .The MK4 amount in Vk2 is 5 mg of MK-4 (not 100 mg as previously posted). I’m so sorry for the mistake. It’s also worth noting that it is pharmaceutical grade (unlike the ingredients of most others Vitamin K2 products).
I see MK 4 at some very high doses, do you know who has it a a lower dose more like 500 mcg or 1000 mcg, which is SOY Free ( Menaquionine) and also has MK-7 in it?
Innovix Labs (www.innnovixlabs.com). Full Spectrum Vitamin K2’s MK-4 is 500 mcg, MK-7 is 100 mcg, no soy. Eric’s vk2 product above is 5 mg of MK-4 according to the website, not 100 mg.
Yes, my Bad . . .The MK4 amount in Vk2 is 5 mg of MK-4 (not 100 mg as previously posted). I’m so sorry for the mistake. It’s also worth noting that it is pharmaceutical grade (unlike the ingredients of most others Vitamin K2 products).
Overpriced at $35 for 60 capsules and the doses are minuscule. I can buy 30x180mcg of MK-7 at retail for $AUS15 = $US10 ie roughly the same dose of K2 for one-third the price. iHerb will sell you 250x100mcg of MK-4 for $US17.27.
https://www.iherb.com/pr/Now-Foods-Vitamin-K-2-100-mcg-250-Veg-Capsules/80111
Another comparison is with Koncentrated K
https://www.k-vitamins.com/index.php?page=Product_-_Buy_Now
This is $45 for 60 capsules each containing 30.5 mg of K – 25 mg of MK-4, 0.5 mg of MK-7, 5 mg of K1 and 2 mg of Astaxanthin.
If you’re trying to reverse atherosclerosis or osteoporosis IMO you need to be taking K in milligram doses not micrograms (200mcg = 0.2mg). In Japan they give 45mg/day of MK-4 to treat osteoporosis. I’d buy Koncentrated K.
Re the natural vs synthetic issue AFAIK all MK-4 supplements are synthetic whereas MK-7 is almost always extracted from natto. I don’t see either as an issue unless you are allergic to the soya in natto.
I presume “GundryMD” is the vegan quack Steven Gundry. He’s basically having a contract manufacturer make it up for him and slapping on his label and a hefty markup. None of the brands you see for sale make the active ingredients – they buy them in bulk and package them in pills or capsules. For any given active ingredient there are a handful of original manufacturers (sometimes only 1) that supply all the retail brands. So one brand’s MK-4 probably came from the same source as another’s. Buy based on dosage and price.
I agree with most of what Stuart’s post, but disagree with his assertion that “one brand’s MK-4 probably came from the same source as another’s. Buy based on dosage and price.”
Most are sourced from China. Both the MK4 and MK7 contained in Vk2 are European sourced and have a yellow color characteristic of pharmaceutical grade, as opposed to the white Chinese materials, which are certainly NOT pharmaceutical grade.
I had estrogen receptor positive breast cancer and will not take anything that includes soy.
I am not trying to reverse osteoporosis or atherosclerosis. I just want a good non GMO soy free low dose K-2 supplement.
Thank you SOOOOO much for taking the time to share your expertise.
I assume the Innovix Labs product I mention above will fill the need. Not sure about the vk2 product.
Innovix Labs product only has 500 mcg of MK4. VK2 has 5 mg (10x more)
Stuart, You mention that Japan uses 45 mg per day of MK-4 for reversal of osteoporosis. I actually read that study…or a couple of them…a couple years ago, but have been unable to locate it online to review it again. I had ‘thought’ that in the study they actually used 45 mg given 3x per day! Would love to know which it was…45 mg. total, or x3. Maybe it was 15 mg x 3? Thanks so much.
Awesome article. Very informative. Is there any well researched article or studies confirming amounts of k2 is high vitamin butter oil the type recommended by weston price to augment benefits of cod liver oil and provide k2? Would you consider vit oil like this a real source of vit k2? Ty. Jennifer Corgan
Input “butter” into the database above to find K2 analysis results for Green Pastures butter oil.
Very easy to read, thank you!
I’m very interested in how to ensure I have absorption of k2 after my gallbladder removal.
I was diagnosed through a CT scan with heavy atherosclerosis. I’m wondering if vitamin K can reverse the arterial plaques? Also, my brand of supplement is in milligrams so I don’t know if it falls into line with your recommendation. Here is the breakdown:
MK7 = 100 mg
MK4 = 1,300 mg
MK1 = 1,000 mg
These are in a base of MCT and rosemary oil. Is one a day adequate? I take it with 5,000 it of vitaminD and also with fish oil supplement. The only prescription meds I take are 2 blood pressure meds and Metformin. Thank you for access to this wonderful resource!
The reversal would need two things, a reduction in insulin levels by any means and the addition of the MK4 vitamin K2 along with 5000 IU vitamins D3 and A to the diet.
The first would be done by getting carbs under 50 mg a day, avoiding fast or starchy carbohydrates, taking 50 mg of Niacin with each meal, then increasing it about every two weeks, taking a 500 mcg chromium supplement. These will all reduce triglycerides.
Second, take an MK4 supplement of 1 to 15 mg, higher if the condition is serious. The vitamins D3 and A will make the calcium removal in arteries more effective.
Beyond this coenzyme Q10 and alpha lipoic acid are popular cardiac health supplements. You might look up NO More Heart Disease by Dr Louis Ignarro who tells hoe nitric oxide protects the arteries from heart disease.
I used the Ultra K supplement with 1.3 mg of MK4 and was startled when over 12 months it got rid of artery calcification and the symptoms I’d had for twenty years. Good luck.
Tumeric, found a video on u tube from a woman in Hawaii who said something about there being more than one pathway to absorption of nutrients. News to me. Dr berg probably has videos there on that subject, possibly supplements too.
more than one pathway to absorption of nutrients,and supplements ….
can one elaborate right here on this ?
Hi! I have CAD (plaque in my arteries) and osteoporosis. I think I need K2, MK4 and MK7! I also have one positive and one negative for Factor V Leiden and recently began Eliquis. What kind of doctor would manage my supplementing with Vit k? Is K2 involved with clotting or just or more so K1? I really think K is the answer but need guidance. I would appreciate your advice! Thank you!
El, Please check out v-k2.com. There you will find several video clips that answer all your questions
Thanks so much for this comprehensive article! What are your thoughts on Jarrow’s K-Right supplement?
Are there any research articles addressing the effect of vitamin K2 in the treatment of kidney stone?
I have been taking K2D3 at the recommendation of my naturopath. My nephrologist is looking for clinical studies.
Any recommendation?
Thank You!
Comments needed on Koncentrated-K from P. Theut. Is this the best therapeutical dose product going? Any success stories with valve calcification? I have it, ready to give to mom. Please, thank you. Daniel
Usage of Artifical intelligence technology in Agriculture and how to use in futuer in agriculture
and its benefits futuer work and discussion.
Does anyone know about K2 claims of spirulina / chlorella product companies?
For example: https://www.energybits.com/about-algae/nutritional-info.html . I was surprised to hear people from one company choosing K2 as a major selling point, while meanwhile I rarely notice algae emphasized on any K2 educational resource. Also, if from algae, can I assume this would be mostly MK-7?
Please add Greek Yogurt to you data. A common one I use is Fage, whole or 2%. Now I am beginning to see why whole fat is better, I would guess K2 , D3, and A vitamins would be higher.
You say take 30+ grams of fat with K2 MK7 , a tablespoon of oils less than 15 gram. Can you share your thoughts.
Thank you for answering and for the time it took to write this article, and database. I hope you will do more YouTube on K2 and diabetes and cardiovascular health.
James Kantor, Raleigh, North Carolina
Important vitamin k2 source that we should know. This would be a huge help.
I am a vegan with low bone density. I would like to eat Natto (only available near me in the frozen form) . My question: Does freezing reduce the Vitamin K2 content?
I have Natto in powder form, and I am wondering about the K2 in that. Unfortunately the bottle doesn’t say. I bought it from Amazon.
My name is Jeff Mindrup. I am working on a db to track CAC regression strategies and openly publish the data to all who want it.
I am on Twitter as MexicoBluePaleoKetoGuy @jeffmindrup
Today, I found some interesting research that shows bioavailability of MK7 is significantly enhanced by taking MY7 with EVOO (~ 4 tsp or 12.5 grams)
https://www.ncbi.nlm.nih.gov/pubmed/21736837
By doing so, under carboxolation of osteocalcin is decreased and carboxolation increased. By proxy, it is safe to assume the same for matrix GLA protein.
This means the standard regression of ~ 50% per 18 months can be easily sped up and made more affordable.
I highly recommend Saint Patrick’s Kon K, reading Kate’s book and ratios of A and D3 to MK7 and now the addition of EVOO when taking.
I also rec eating frozen chunks of natto daily if you have a high CAC score. It is by far the best source of MKn’s (all of them) as well as fibrin breaking nattokinase. See Malcolm Kendrick’s tree ring explanation with Ivor Cummings.
Hi Jeff, I am trying to understand what you are saying in your post. I truly do not know anything about Carboxolation. I have heard hundreds of seminars about K2, MK 7 & MK4, Vitamin D 3, Vitamin A, but never has this term been used. I know about Fibrin as well; due to my own blood work. What is MY 7? What is EVOO? What are the benefits? Are their any toxins in liquid EVOO? Where is it from (manufactured)? I never heard of a CAC score when doing any of my bloodwork. Thank you for clarifying.
Hi Jan, I can’t answer all of your questions, but CAC is coronary artery calcium score…an indicator of plaque build-up in the arteries for those using K2 for arterial health. EVOO is Extra Virgin Olive Oil…it can actually be a ‘grade’ or designation given to olive oil to indicate the quality of said oil. As I recall, the author of Vitamin K2 and the Calcium Paradox gets into the deffinition and explanation of carboxolation…I don’t recall enough of the details to explain. Lastly, I’m ‘guessing’ that when Jeff said MY-7, it was a typo and he meant MK-7. Hope this helps. I found his comments fascinating and will do more research 🙂
Yes – apologies for any typos. EVOO = olive oil. See study for more info but this is critical because bio-availability and absorption are significantly increased. We also know that not all fats are the same from another study comparing corn oil and EVOO w/sunflower oil. Again the EVOO, despite being a blend was superior for carboxolation.
Jan, I’d really like to speak with you as well as get your help in getting your following to input into the db I am building which will be focused on CAC regression strategies.
The end goal is to freely distribute the best practices for CAC regression and improve upon what appears to be the standard (for APOe3/3s anyway) of about 50% every 18 months.
Kind regards,
Jeff
@jeffmindrup on Twitter
Looks guys. There are some crazy uninformed and un-researched ideas in here and they are confusing the crap out of even me that spent last 6 months studying this subject. Bottom line.
# 1. Get Patricks Kon K – best formula – full stop. Best value, strongest, etc. From looking at the label and using the value tool Carlsons is waste of money once you understand it’s all about the MK7. (Exo Mk4 does not show in serum, MK7 converts to MK4 in vivo) Alternatively/additionally eat natto. I do everyday.
# 2. Read Kate’s book. Just buy it and read it. Don’t be cheap.
# 3. Yes – A, D, and EVOO to get full benefit of K and especially MK7
# 4. Don’t get lost in the weeds – way too many unknowns with K and will be for some time because it’s can’t be patented and there’s little research on it. New study expected any day now. (but not well formed IMHO)
#5. K2 shows zero toxicity in every study ever conducted. Half-life of about 36 hours, peaks at 4-6. If Lance Armstrong has tingling fingers, it’s more than likely from the dozens of other illegal drugs he cheated with. The guy gave himself cancer and is an admitted fraud and liar. Why give a POS any credit? PS his LiveStrong was a grift to benefit him. Not to help others. Corrupt through and through. Do your research.
Responding to Jeff’s points:
#1. Agreed that Patrick Theut’s Koncentrated K is the best value per gm, but I base that on its MK-4 content. I don’t agree “it’s all about the MK-7”. The Rotterdam group maintain that MK-7 is best based on it having a longer persistence in the blood. I’ve never found that argument convincing. If the body prefers MK-7 why does it make MK-4 instead and why is MK-4 found in human breast milk? What does the body do with the MK-4 from your supplement? Chris answers that in the article above – the cells preferentially absorb the MK-4 so that it is rapidly depleted in the blood. That says to me that MK-4 is the optimal form, but I also take 180mcg of MK-7 as insurance.
#2 I can’t find a copy of Kate’s book here in Australia and I would have to order it sight unseen from the US. International postage would more than double the cost. To illustrate, I recently bought an out-of-print book from a US bookseller. That $US30 book cost another $US30 in postage plus 10% import tax and the conversion to Australian dollars makes it $AUS100. That ain’t pocket change.
#3. As Chris outlines here:
https://www.westonaprice.org/health-topics/abcs-of-nutrition/nutritional-adjuncts-to-the-fat-soluble-vitamins/
the body also requires magnesium and zinc to manufacture those vitamin- dependent proteins as well as dietary fat to absorb the vitamins in the first place.
#4. Got a reference to that forthcoming study so we can look out for it? Why don’t you regard it as well formed?
#5. Agreed I wouldn’t put much credence in Lance Armstrong. His main nutritional supplement was Vitamin S – S as in steroids.
Curious…. How important do you consider the role of resistance training to up-regulate osteoblastic flux to signal “hey… the bones need more calcium and phosphorus… can anyone spare any?”.
Thank you so much. I will be going for my first Calcium Scan. Trying to keep the heart healthy; I was able to bring down my Fibrinogen due to a vitamin supplement. So I certainly know the benefits of supplementation. I am trying to figure out a good balance when taking 3000 iu of Vit D3, How much K2 & A should I take? Because I don’t take 5000 iu of D3, it is hard to calculate how much of the other vitamins to take when it appears everything is based on 5000 of Vit D3.
Jeff said “its all about MK7” which demonstrates that is clearly in the MK7 camp. I have not seen any studies that confirm MK7 is converted to MK4 in an efficient way. What about for older people? Does the age related conversion inefficiency of K1 to K2 also apply to any MK7-MK4 conversion? I would certainly not be surprised if it did.
Clearly more research needs to be conducted on this important topic before any conclussions can be drawn
My intention is not to bash Jeff or the product he is promoting, Rather I would just suggest that MK4 has many important qualities that distinguish it from MK7 and since there is no harm in taking MK4, so why not take it?
I am not promoting a product. Even the maker sells at a LOSS. It’s about helping people. ZERO AFFILIATION. ZERO GREED.
Even the db I am doing at time and expense is on me.
Read the research.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3502319/
https://www.ncbi.nlm.nih.gov/pubmed/19949269
I’ve used both MK7 and MK4 products, (not concurrently) together with D, and A and EVOO as well as a compliment of other synergistic nutrients/foods. Natto is not on my plate, yet, but that’s primarily as I don’t eat breakfast and that’s how it seems to have been used traditionally, and secondarily because I had cardiac rhythmic irregularities that were simultaneous with MK7 supplementation (about 9 years ago) and that have never reoccurred since ceasing MK7. At 64 yo, I’ve not had a CaC done or any known problems with blood vessels or symptoms suggesting the need for such a scan, although I’ve been tempted to do so just to find out (not a big fan of CAT/CT scans unless warranted) . The rhythmic irregularities also corresponded with unrefined organic Coconut Oil usage so I can’t be definitive as to the actual cause of the symptoms (possibly glycerine related and with low RBC magnesium level possibly related to chronic mercury toxicity possibly made much worse by 40 yo amalgam being removed by a dentist that took no precautions for his patient (and I’ve had 13 others of similar age since removed with the best precautions and thankfully without any problems since)), but in any case, the avoidance of both CO and MK7 eliminated the problem (together with judicious supplementation of Magnesium, Taurine and Arginine.
It’s possible that by my age (or earlier, say early 50’s, when I first experienced problems mentioned above) conversion of the K’s has decreased considerably, both from k1 to k2, and from MK7 to M4. Low serum levels of MK4 after supplementation might be indicative of the nutrient being effectively used (rather than excreted; not sure if ever measured); high levels of MK7 persisting for days in the serum might be indicative of a problem with utilization ( a half-life of 36 hrs!).
Just saying tho: a lot of people have reported problems with taking MK7 besides me. I’ve never had any problems with MK4 and I’ve taken upwards of 15-30 mg daily, although I’ve settled back on about 5 mg daily for a while now.
https://www.k-vitamins.com/
This is a very significant resource on the subject!
Another great resource with video.
I responded to this post days ago but it has not been published. Why?
Carboxylation is the last st that turns calcitonin and Matrix GLA proteins into functional chemistry in the body. This is done by MK4 vitamin K2 and to a lesser extent by the MK7 form. Both of these are needed for calcium metabolism, calcitonin works to build new bone and Matrix GLA reverses calcification of the arteries.
The body turns vitamin K into MK4 vitamin K2 for this purpose. With age or high cortisol levels, MK4 production declines and patients experience bone loss and artery calcification. A supplement of MK4 is then needed. Several trials from Japan show a 60% to 80% reduction in bone breakage rates for the elderly with 45 mg of MK4 daily.
Yes, MK4 works for bones, but there are no studies that show a benefit for calcification of the arteries. Only MK-7 works to reduce arterial calcification, as shown in studies.
I just corresponded with a physician overseas undergoing a study on 1000 micrograms of MK-7 to decalcify the aorta. He advised me to use 720+ micrograms MK7 daily. While I greatly appreciated his advice, I have to ask others what they think, because I have been giving my mom (with severe mitral valve stenosis) 10mg MK4 Carlson brand and 360 micrograms MK7 Utzy Naturals brand daily for 9 months. I just want to make sure we are doing the best thing for her. Please, if you have any input we would appreciate hearing from you. Thank you, Daniel
Any thoughts on supplement versions? Trying to determine MenaQ7 vs. Menaquin Gold products. Any of these better than the other? Using Kon K now, I just don’t see a lot about it. Important to be giving mom something that is very effective with her heart issue. Thanks for input.
I don’t know who wrote the K2 article. It is incomplete the way it is now. The author mentions the book, Vitamin K2 and the Calcium Paradox: How a Little-Known Vitamin Could Save Your Life, by Kate Rheaume-Bleue, but he or she apparently didn’t read it, because it is necessary for Vit A (retinol) and Vit D3 to be present for Vit K2 to do its job of keeping out of the arteries and other soft tissues, and to put it into bones and teeth. A paraphrased sub-title in the Calcium Paradox book is: Vit D, Vit K 2 and Vit A: Better Together.
I encourage everyone to read the Calcium Paradox book.
Albinka – agreed 100%
Way too many miss the A-D-MK7 ratio and provide harmful advice that could lead to hypervitaminosis. I have found supporting research for Kate’s ratio and sent it directly to her.
Jeff
Albinos and Jeff: Chris has written elsewhere about the synergy between vitamins A, D & K. See
https://chrismasterjohnphd.com/blog/2016/12/03/start-here-for-vitamin-k2/
https://www.westonaprice.org/health-topics/abcs-of-nutrition/nutritional-adjuncts-to-the-fat-soluble-vitamins/
It’s interesting that the necessity for both A and D was known in 1941 but the medical profession today has forgotten it.
If a person is taking 3000 mg of D3, how much K MK-7, MK-4, Vitamin A should they be taking? Thank you for your help. I have severe dry eyes from Sjogrens so I can’t read allot of books & I have a limited ability on the computer as well. If you can help me it would be appreciated. Ty
I am not an MD and have one concern, the regression of CAC scores via MK7. Please see an ophthalmologist. I do 2x a year.
56 and 20/10 vision – no glasses required other than for reading very small print.
Awesome article… I’m interested in increasing my k2 and was thinking about taking it in a tablet to increas my dose. But Im on xeljanz ( tofacitinib) to treat my ulcerative colitis and one of the side effects is it can increase cholesterol levels. So was wondering if you may now if I can take a supplement of K2 whilst I’m on xeljanz especially if xeljanz my affect my cholesterol.
Is there a sortable list of the Vit K2 database?
Thank you for all of your work
BIG question here, as everyone talks about calcification of arteries. Can we assume that K2 will ALSO improve calcified heart VALVES? Mom has severe mitral valve stenosis, started her on daily 5mg MK4 (Carlson brand) and 180 mcg MK7 (Utzy naturals). Mitral valve area started as severe (Area = 0.96 cm2) to now at moderate (1.12 cm2) six months later. I am thinking we want to increase the dosage (basically double it) as progress seems slow. Can anyone offer comments please thank you so much. Daniel
It may take 12 to 18 months for fully reverse this although you should hve good progress by 6 months. The MK4 form will work for calcified valves as well.
You might increase the dosage, but also consider including a vitamin D supplement and a retinol vitamin A supplement. Both of these contribute to calcium control. The vitamin D3 increases the supply of the Matrix GLA protein that prevents calcium in the arteries and the retinol vitamin A makes the Matrix GLA more effective and reduces the rate of kidney stones. Best of luck with this!
David thanks. Gave Mom 5000 i u D3 for years without K2 which we think contributed to this problem. She is taking so many heart pills we are trying not to add more. terrible. We have doubled the k2 dosages and now blood pressure is coming down which I believe should be expected side effect?
What is MatrixGLA, and does it help to supplement with liquid GLA?
David has a solid understanding of this. Well done David.
Other’s get the book by Kate – no affiliation.
Folks you have been very helpful. Do you have any consensus on Koncentrated K capsules which contain 25mg of K2 MK4 and .5 mg of K2 Mk7? Looks great, Thinking of trying this out on Mom valve stenosis. I bought it just seeing if others have experience using it.
Appreciate your thoughts.
Dan, the man behind Koncentrated-K is Patrick Theut. Pat was diagnosed with extensive heart disease by the Mayo Clinic and was a patient of Dr William Davis of Wheat Belly fame. Pat reversed his heart disease with high doses of K2 and other supplements and a Low-Carb-High-Fat diet. Google his name and you’ll get lots of hits where he’s been interviewed. He also gave some talks to the Wausau Wellness Centre that you can find on YouTube.
I don’t have any personal experience with Koncentrated-K as I’d just bought a large supply of Carlson MK-4 before I came aware of Pat’s product, but I will order it once I use up my Carlson stock. On a cost/mg of MK-4 basis Koncentrated-K is the most cost-effective way of getting a large dose that I can find.
Daniel I’ve just found this site and was interested in your post as I have severe aortic stenosis and have been researching the use of vitamin k to help. Would be very interested to know what your mum is using and if it’s helping ? Thank you
Hello!
I have a A1298C mutation. I would like to take k2 but I am a bit worried about the rick of clotting. I take daily 75 mg aspirin to prevent and my blod tests are normal.
I have been searching for info regarding k2 and blod clotting but I can only find people who take warfarin. Could you please tell me if it’s ok to take k2 and if so, how much?
Thank you!
Hi 🙂 thanks so much for this article. I am vegan and have recently learned that it is not uncommon for vegans to lack K2 (although I don’t know what symptoms I should be looking for, or tests that could be done to determine this)
I have tried buying the three recommended K2 products but none deliver to Australia. Could you please recommend one that does?
Thankyou
Often there are K2 dosage restrictions related to vitamin K that get applied to imports which are totally unrealistic. You may be able to order the Thorne liquid K2 which doesn’t come in a specific dose. iherb also supplies to a number of countries with import restrictions. See if you can find nearby discussion groups on the MK4 vitamin K2 and ask there about suppliers.
Emma, the major problem with buying from the US is the extortionate postage charges by the United States Postal Service. They regard those of us who post internationally as a cash cow that they can milk without a political backlash. (so just like Australia Post then) To make it affordable you generally need to buy from someone like iHerb who’ve organised alternative shipping arrangements to bypass USPS.
I’ve bought Carlson’s 5mg MK-4 from iHerb
https://au.iherb.com/pr/Carlson-Labs-Vitamin-K2-MK-4-Menatetrenone-5-mg-180-Capsules/14812
iHerb seems to charge Australian customers 12% more than US customers and then there’s 10% GST on top. OTOH they don’t charge freight if you order $US40 or more.
I also take 180mcg MK-7. This brand which I buy at Chemist Warehouse
https://www.chemistwarehouse.com.au/buy/73731/nature-s-way-osteo-k-vitamin-k2-180mcg-30-soft-capsules
The US products all seem to be 100mcg and work out more expensive on a per mcg basis.
An interesting product is Patrick Theut’s Koncentrated K
https://www.k-vitamins.com/index.php?page=Home
It’s expensive but offers a high dose of MK-4 and MK-7 at the lowest per-dose cost I’ve seen. Pat says he hasn’t made a profit on the product and I believe it. Pat is a small operator so has to use USPS. You need to buy 2 at a time to amortise the postage cost.
BTW it’s well worth reading Pat’s “My Story” on the Koncentrated K website and watching some of his video talks and interviews. Ivor Cummins interviewed Pat for his Fat Emperor series and Pat gave some talks to the Wausau Wellness Center, all of which you can find on YouTube.
Unless you are a regular consumer of natto, as a vegan you are almost certainly deficient in K2 since the principal sources of K2 are animal products or fermented foods like cheese. The human body has very little ability to convert K1 to K2. In regard to the consequences of Vitamin K2 deficiency they are principally osteoporosis and calcification of the arteries which are in effect two sides of the same coin. Your body needs K2 to make the hormone that deposits calcium in your bones and prevents the Ca being deposited in your soft tissues. To determine whether you have those conditions requires a bone density scan for osteoporosis and a Coronary Artery Calcification scan will indicate the degree of calcification of your soft tissues.
If the bone density scan indicates osteoporosis your doctor will probably want to prescribe a bisphosphonate drug such as Fosamax. This will improve your bone density scores which will make the doctor happy but not prevent fractures because it results in brittle bone that can fracture in normal walking. It also has a nasty side effect known as Osteonecrosis of the Jaw whereby the bone in your jaw dies following dental work, causing disfigurement and requiring facial reconstruction surgery. So refuse to take it
To recover from osteoporosis you need:
1) Adequate levels of Vitamin D either from sun exposure or supplements, in the region of 50-60 Ng/ml. Get tested. You need Vitamin D to absorb the calcium from your diet
2) Adequate calcium and phosphate in your diet, since bones are composed of calcium phosphate in a protein matrix. The best source of calcium phosphate is milk and dairy products (another strike against vegans)
3) Vitamin K2 from diet and/or supplements. Because there isn’t an easy way to test Vit K2 status it’s prudent to take supplements
4) You have to ensure adequate protein in your diet, 1.2 grams of more of protein per kg of body weight. Note that this is 50% more than the Recommended Daily Allowance of 0.8gm/kg, which tells you how much reliance you can place on the RDAs and the dietitians who regard them as holy writ.
5) Last but certainly not least, you have to undergo load-bearing exercise to stress the bones and provoke bone deposition. Both bedridden patients and astronauts lose bone mass through lack of stress on the bones. The exercise can be walking or lifting weights or something as simple as skipping rope.
For more on osteoporosis read the blog of Robert Heaney
http://blogs.creighton.edu/heaney/
Until his recent death Heaney was probably the preeminent researcher into osteoporosis.
I’ll write more about the implications of a CAC score later.
Yes Emma, Vegans are often Vitamin K deficient. You would not likely notice any symptoms, even though you are likely building up calcium in your arterial linings and heart valves. VK2 can be shipped to Australia. I hope this info is helpful to you
Hi Emma,
Vegans will be deficient in vitamin K2, MK-4, because it is only found in animal foods. Too bad you couldn’t take advantage of the wonderful source of K2 -MK-4 -found in Australian emu oil, such as Emu Tracks, which is in a food matrix and well-absorbed by humans. MK-4 is the ONLY bio-active form of vitamin K2 for humans. We are not bacteria. However, there is much controversy about bioavailability and absorption of supplements in general, which are most often made in a lab and not from natural food substances, nor are they located in a food matrix as are nutrients in food. You may absorb a limited amount of MK-4 from an artificial supplement but who knows how much? I recommend a natural source which is much more bioavailable.
Hi Dr Sylvia, I thought our gut was full of bacteria…?
I’m not sure why so many have complained about the cost of shipping to Australia. The cost of shipping 1 or 2 bottles of vK2 is $16.25 (First-Class Mail International)
3 bottles ship for $25.50
Hi, I’d like to know about vitamin K2 supplementation for a person with coronary artery disease. Does it help?
Yes, it is helpful for improving artery calcification and has been listed so by the Health Ministry of Japan since 1995. Calcification level is one of the best predictors of cardiac disease so controlling it is vital. The K2 enables an MGP protein to work well. Taking 5000 IU of vitamin D3 boosts production of MGP and 10,000 IU of Retinol vitamin A helps control calcium by improving MGP production and lowering kidney stone formation.
Don’t skip the other paths to cardiac health such as adopting a low carbohydrate diet, improving nitric oxide function with daily arginine between meals, reducing triglycerides with 100 mg of plain Niacin several times a day, and taking the gamma form of vitamin E to reduce clotting.
Thank you so much! These comments are so helpful. The mainstream medical community does not have much to offer.
Yes Susan, Vitamin K2 is helpful in improving arterial calcification. MK4 is the form most useful for that, while MK7 is the form most useful for improving bone density.
VK2® provides both MK4 and MK7
Please advise how much Vit D should be taken with Vit K2-7. Thanks
Take the vitamin D3 for its own benefit, usually blood levels of 50 to 80 ng/ml in American units are optimal for best health. This tends to be a dose of 10,000 IU of D3 for those with normal fat absorption. The vitamin K2 works with the MGP proteins that are boosted by taking more vitamin D3.
Have a look at taking the MK4 form of vitamin K2 which is ,what the body makes for its own use. The MK4 functions in many more places than the MK7 form does.
Jeronimo,
The idea is to have sufficient Vitamin K2 to activate all of the Vitamin K2 Dependent proteins (VKDP) in your body.
That exact amount has not been exactly determined.
Certainly, taking Vitamin D3, which stimulates the production of VKDPs, increases the demand for Vitamin K2.
Numerous factors which might impact how much Vitamin K2 is needed include: how much Vitamin D is being taken, what medications are being taken, overall health status etc.
Each capsule of VK2® contains 5mg of MK4 and 100 mcg of MK7. Its recommended to take one capsule of VK2® for every 5000iu of vitamin D3
I have a hereditary stroke possibility, from the female line. Have you heard of this and do you think Vit K is involved?
While improving general circulation health will help prevent strokes, the next thing is to figure out if these are strokes due to clotting or due to bleeding, then address the specific cause. Strokes can be caused either due to clotting or due to bleeding.
The MK4 vitamin K2 would help with general circulation health and if there is artery calcification present, it improves this and the condition of the blood vessels. This should help both kinds of strokes. There can still be problems with artery narrowing or excessive clotting that need to be addressed by lowering insulin levels with a low carbohydrate diet, taking plain Niacin (see doctoryourself.com) and looking up a variety of actors like alpha lipoid acid. Dr Louis Ignarro has an interesting book out on heart disease. The gamma form of vitamin E is effective for lowing INR and blood clotting.
For bleeding strokes the important thing is blood vessel wall integrity. This emphasizes building the connective tissue in the blood vessels with enough protein, vitamin C, and copper.
Don’t let the doctor tell you to not take vitamin K2, it doesn’t function strongly in clotting, has been shown in extensive readership trials to not induce clotting and has been safe even at high doses. Do have a talk with a qualified health professional on your particular stroke type. Just remember that doctors are not trained in nutrition and the medical references are decades out of date on vitamins.
Youtube is a phenomenal resource because of poorly educated health professionals… if prescription drugs are not involved then they are out of the loop! I believe strokes are about blockages and if your lucky bleeding will be followed by clotting. We have moved forward much faster by sharing! L
Still seeking a one dose, 300 to 360 microgram mk7 pill for mom, as she takes so many heart pills. The kicker- we prefer no soy but rather chickpea based. Can anyone help us? Thanks so much
Daniel,
If your mom has heart issues, perhaps mk4 may be a better choice . VK2 has both MK4 and MK7.
If you visit the site, you can watch videos that explain in details
Daniel —
I came across this K2 MK-7 on Amazon: Rejuvenation Therapeutics Vitamin K2 MK-7 has 300 mcg capsules almost double the strength of any other brand on Amazon. All natural and derived from natto beans. Here’s a link:
amazon.com/Rejuvenation-Therapeutics-Clinically-Powerful-Capsules/dp/B0765NLPR3/ref=pd_ybh_a_1?_encoding=UTF8&psc=1&refRID=S2S79QMHZ51HJTB552N0
Yes I have a bottle of this in my possession but it is natto based. Mom has a soy sensitivity will this affect her? Also, the manufacture date was 2017? What do you think about that?
Hi Daniel,
Have you tried Andrew Lessman vitamins? I order all of my vitamins from him. The products contain no soy, and are all 100 percent guaranteed. He has several VK2-MK7 products. All ingredients are the best available. My mom and I have been taking his vitamins for the past 20 years and we will only use his products. He will be appearing on HSN network next month in Oct. if you want to check him out. Good luck and best wishes!
Hi Chris
I am an 85 year old female.
I have been on the diet for at least 10 years.
I just discovered the vit. K2.
I have severe dizziness and am hoping that the vit K2 will help.
I take vitamins from constantin they are very good..
I am so happy that I am on your list
Yours very sincerely
Elisabeth
Sorry, I should have asked about the D3 dosage also. There are tons of 5000 IU products. That would be the easiest thing to buy. I’ve read widely varying opinions about safe dosage levels. Two commenters elsewhere said that dose caused them to fall down a lot, one person breaking an elbow. When they dialed back the amount they stopped falling down. There are other concerns as well. How do we know what to believe here? Thanks again.
I’m thinking of taking a D3/MK7 supplement that would give me 360 mcg of MK7 per day. This is more than all daily dosages I’ve seen, but based on the reading I’ve done, it’s probably OK. Is this correct? Thank you.
Van,
Research has not determined the maximum safe amount to take, but there are certainly many factors that need to be considered. The more vitamin D you take, the greater the demand for vitamin K2. For a very informative video on topic, please visit http://www. v-k2.com
Hello!
Have you heard of the supplement Mega-Quinone K2-7 from Microbiome Labs? I didn’t see it in your reviews and I am wondering what your thoughts are on it?
I’m asking in regards to someone who has Osteopenia. In the “Calcium Paradox” book you mentioned in your recommended reading, the author recommends 240mg MK-7 for those who have Osteopenia or Osteoporosis, and it also mentions K2 supplements with K1 included in them are not necessary. The Mega-Quinone K2-7 supplement actually has 320mg of MK-7 from fermented chickpeas and includes 100mg K1 and Magnesium “for absorbability” purposes. Do you believe this dose is too high? What if that person is taking a high dose of Vitamin D3 in conjunction? Would they then be ok as long as they up their Vit. A intake?
Stephanie, you may want to consider both MK4 and MK7. Please check out http://www.v-k2.com
There is a video clip which explains why
What about MK7 re estrogen production related to potential breast cancer reoccurrence in women treated for breast cancer?
I ordered a bottle of Ultra K2 from Stop Aging Now. The K is listed as menatetrenone. One capsule has 15,000 mcg and they recommend 1 capsule per day. Is this amount too much? The bottle says that is 12,500% of the daily dose!
That is a reasonable dose for the MK4 form of vitamin K2. Doses used in research have ranged from 1.5 mg to 135 mg daily with 15 mg three times a day (45 mg) being the most typical research dose. This gives the best results in research trials but lower doses have been tested successfully.
I had great success in taking 1.3 mg for 12 months with artery calcification. I notice a few improvements in going to a 6.5 mg daily dose so many people can be helped with a 1 mg to 10 mg dose. If you have hazardous medical concerns with bone loss or artery calcification, taking the 45 mg per day dose can be justified as this requires the best possible results.
Medical references have been very conservative on qualifying MK4 vitamin K2 with a traditional 120 mcg dose for Vitamin K. This dose ignores all the many research papers on MK4 and that the Japan Ministry of Health has listed MK4 vitamin K2 as a treatment for cardiac disease and bone loss since 1995. Th eMK4 form has been tested as low in side effects even at doses of 135 mg (135,000 mcg) per day, so the 22.5 mg is safe.
Which mk4 or mk7 dosage is most important?
is it ok to take k2 with D3 or it should separate?
Tamer,
I suggest you visit http://wwwv-k2.com
There is a ton of info that you can read and there is also 2 videos that you can watch.
The short answer is that both mk4 and mk7are important as they each have different qualities. Yes vitamin K2 can (and should) be taken at the same time as Vitamin D3
Just came back from the hospital where moms Echo showed mitral valve area going up from 0.96 cm squared to 1.12 cm squared in 6 months. Using daily five mg MK4 Carlson brand and 180 MCG mk7 utzy Naturals brand. I think we’re going to double the dose of both. Please comment!
What are your thoughts on K2 while thru hiking or long distance hiking?
I have heart disease , 3 vessel stenosis, I believe statins help to stabilise the plaque by calcification, I want to take K2 MK7, will this destabilise the atherosclerotic plaques and make them more prone to rupture, when K2 MK7 starts to remove the calcium build up , I am struggling to find a suitable answer to this question.
Regards
Gary
I hope someone can provide some insight on this for Gary….thank you.
In 2007 I had three vessels calcified to 90% plugged. Went on statins , cholesterol down to 131 in 2015. In 2016 learn of K2’s. started on MK7 and MK4 back and forth. Cholesterol shot up to 281 last year. went back on statins for a month plus B3 till my net test, Cholesterol down to 181. two months ago started on thoren vitamin D3 1000IU/mk4 . 2 drops 200mcg , vitamin d3 5000IU, Boron 3mg, Vitamin A 2662 IU, Mega COCQ 10, Astaxanthin 12mg. Had particle test two weeks ago–cholesterol 198, partial size and number in range. I’m still standing upright.
Watch this. Will explain about K2 and statins driving up cholesterol.
Hope this helps. https://www.youtube.com/watch?v=X4RipKub_Y8
you may also want to check out these clips:
https://www.youtube.com/watch?v=nfy8Gmbj14c&t=1s
and
https://www.youtube.com/watch?v=zjOsDL1dhJE
This is not an in-depth answer but it does come from the website of Dr. Kate Who wrote the book… Vitamin K2 and the calcium paradox…
Since K2 reduces plaque, won’t it increase the risk of a clot or heart attack as pieces of the plaque break off?
This is a FAQ since as we understand K2 helps reduce arterial plaque it is easy to imagine it being chipped away or breaking off in chunks. That is not the way K2 shrinks plaque and K2 supplementation has never been associated with a cardiovascular event. In fact, vitamin K2-dependent proteins make plaque more stable and less prone to rupture. Recent clinical trials for reducing plaque in a group known to be at high risk for calcifications used MK-7 in does of around 360 mcg per day with no significant adverse effects (a few participants experienced stomach upset at this dose).
I don’t know if this would help but it might be worth reading:
https://www.lifeextension.com/Magazine/2016/2/Slow-the-Progression-of-Atherosclerotic-Plaque/Page-01
I have been taking this Arterial product 2X per day which is twice their article recommendation and I take additional 100 mg. Pycnogenol at 2X per day since some studies seemed to have some stabilization effects at high doses. This is a fairly expensive treatment at these doses.
I also take K2, D3 and A.
Won’t really know if this is working for me until my next scan in Nov 2019. but it looked like something to try since I have 2 blockages at around 90% as of last Nov scan.
This is not a recommendation for you, but I felt that in my case it seemed worth a try.
Have you had an update scan? How are you doing?
Gary, I have some stenosis in 2 vessels and a calcium score of 579 3 years ago, probably a little higher now.
The thing is to stop focus on removing or stabilizing plaque, but on stopping depositing it. To do that I went on a whole food plant-based diet with no added oils, per Dr. Esselsstyn. Great results, not as hard as I had thought. But it does take grit and determination at first. It has a good track record, and you can find out more by watching the movie “Forks Over Knives”.
It works for me, my doctor agrees, and I’m on zero statins, BP went from 140/90 to 110/70, not bad for 73 years old. No meds at all, no stents, nothing. I climb long flights of stairs several times a week and workout with weights.
I believe that so long as you are providing dietary building blocks for plaque, the body will use them and to hell with all your vitamins and drugs, the disease will progress anyway. By not putting in things which damage your endothelium (inner layer of cells inside the artery walls) it works to stop and reverse the disease. I would advise this diet for a few months, then start program of exercise to reverse the disease WHILE on the diet. Don’t exercise prior to the diet, it can raise risk a lot. besta luck, pal Bob
..BTW, coronary calcium scores may vary and there’s no really good studies on them responding to diets and other things, however, it is known that when plaque begins to go away on whole food plant-based diets, calcium scores at first rise. This is the body throwing in some extra calcium to stabilize the softening plaque and prevent ruptures and lessen clot risk. It knows, it’s been there before in the millions of years of our evolution. This data is per Dr. William Castelli, former director of Framingham Heart Study. Calcium is about 20-25 percent of plaque volume, so if you lose 10 percent soft plaque and gain 10 percent calcium, you’re way ahead. Exercise will drive collateral artery formation around the blockages, but is risky if the diet is atherogenic (sat fat, cholesterol) since it weakens the fibrous cap over the plaque. The whole food plant-based diet strengthens this cap and makes you heart attack proof from plaque ruptures, which is 90 percent of heart attacks right there. Dr. Esselstyn says it takes about 3 weeks for this to happen on the diet. I’d say give it 2-3 months before exercising in earnest. I have seen 2 people taken out from my gym on gurneys in the same week, they probably thought if they exercised, they could eat whatever they wanted. This is backwards!! If you eat right you can exercise all you want is more like it.
Well, from my understanding, artery calcification is mostly caused by chronic inflammation not high cholesterol per se. A low carb/sugar diet along with avoiding Veg/Seed oils (PUFAS) at all costs. A whole foods, Ketogenic diet along w/ a targeted D3, K2 (MK4 & MK7), Magnesium, Zinc, Vit A. , etc. I’d check out Ivor Cummins interviews/lectures/vids on YT for starters. I try to keep updated & take in as much info as I can. It’s been said recently (not in any mainstream media way mind you) that Diabetes IS Pre-Heart Disease. A Ketogenic diet (or some cases simply a low-carb diet) reverses T2 Diabetes & Pre-T2 Diabetes. So, it stands to reason.
PUFAs aren’t bad for you. Let’s not demonize another nutrient. The problem with some PUFAs, specifically the omega-6s, is not keeping them in balance with the omega-3s. See https://www.diagnosisdiet.com/arachidonic-acid/ for one example of an important and necessary omega-6 PUFA.
Still, don’t use seed oils to get them—maybe try some lard—because throwing off your fatty acid ratio is hardly the only problem with industrial oils. They go rancid, oxidize, and are apt to contain residues of solvents and other noxious chemicals used in their processing.
Not for nothing, but when I said PUFAs, I did in fact mean Seed Oils/Veg Oils, kinda goes without saying. Every lecture or interview I’ve ever watched or read on this subject, everyone typically using the term PUFAs for Seed Oils. I thought it safe to assume you knew what I was talking about when I used the term PUFAs. However, your critique is duly noted.
Are you talking about Flaxseed Oil? I just ordered a bottle to help with my dry eyes. Please let me know, TY
If i may chime in…PUFA has been used a lot in health circles to refer to industrialized oils (corn, peanut, soybean, canola) and we as an audience tend to get a bit robotic with the term. Not all PUFAs are bad, but my understanding is that they all turn bad once heated. I mean, look at cod liver oil (high quality ones like Rosita or Dropi), they have omega-3 DHA and EPA which are PUFAs (to my knowledge). Even oils like walnut have their place in our diet according to Sarah Pope, a member of the Weston Price Foundation.
I would love to know the K2 content of Liver and bone marrow. I hear both are good sources of K2.
http://wholehealthsource.blogspot.com/2008/11/vitamin-k2-in-marrow.html
Natural Vitamin K2-7 is very important for healthy life e.g. Bone health, Diabetes management and Muscle health etc.
MenaquinGold is the most researched natural vitamin k2.
This is properly explained in this page.
https://www.synergialifesciences.com/natural-vitamin-k2-menaquingold.html
Is mk7 safe in a kidney transplant recipient?
Is there any way to counteract the insomnia caused by mk-7? I need to take it but I need my sleep!
Do you take magnesium? Perhaps take K2 in the morning and Magnesium citrate in the afternoon? I’ve found K2 and Mg work in unison for me (but I don’t have to take them at the exact same time)…
Hi Michelle,
You have the classic symptoms of being sensitive to the MK7 form of vitamin K2. There are anxiety, sleeplessness, a thumping heart beat, and possibly raised blood pressure. The solution is to stop taking the MK7 vitamin K2 and switch to the MK4 form which is native to all mammals and has few side effects in the human body. Typical doses for the MK4 form are 1 mg to 5 mg, and higher if there is a serious medical risk. Carlson makes a good 5 mg MK4 only tablet and Thorne makes a liquid MK4.
The MK7 has a half life of 3.5 days in the body so I may take a while to clear out. Know that natto is a fermented bean that contains very large amounts of MK7. The MK7 is made by bacteria and it is only partly functional in the dozen tissues that MK4 works in.
If the MK4 is being taken to improve bone strength or reduce artery calcification, note that 5000 to 10,000 IU of vitamin D3 and a similar amount of Retinol vitamin A will help by boosting production of the calcium handling proteins that MK4 activates. Taking 200-400 mg magnesium and 12 mg boron will also be helpful.
In my case I resolved a 20 year case of artery calcification in 12-18 months by taking 1.3 mg of MK4 daily. So the MK4 form will be more effective and and work better than the MK7 form.
David,
Do you have a blog where you talk about the details of your journey of resolving the calcification? I am very interested….thank you.
Hi Mr. Sander:
When you resolved your 20 year problem did you get a calcium CT score before and after.
If so, can you please share with us what the scores were?
I used similar amounts Boron at the 12 mg and magnesium citrate at 800 mg per day (the Carlson Mk4 2x day) same D and A plus 360 micro’s of MK 7 and a strict Mediterranean diet and my CT score increased at 35% per year.
Boom! Great answer, David. Another reason why I’m a fan of mk4 over mk7 👌🏼
Hello, please help me. I took Mk7 by Jarrow for about a year and added coral calcium to the mix and my head started to grow. Im not sure why I continued to use it but I ended even getting vitamin d3 and k2 drops after and it grew more. Now I can barely stand my appearance because I feel it made me look worse. Is there any possibility it can reverse?
Have you asked any guys? I’d find that kind of hot, myself, brainy lady with cute face wow. I think if you stopped doing the calcium it should stop happening, though, just my opinion, I would do that. I’m bald, so my head bigger, probably not good. Best of luck,
Heather, more likely your eyes got smaller or your brain got smaller so your head looks bigger. The only documented head growth is among bald headed men. That’s why bald headed men like Robert Luhrs are smarter.
Heather,
All kidding aside you may ask your physician to test you for acromegaly, excess growth hormone. There are good reasons to believe that K2 and calcium supplements would contribute to acromegaly skull growth. The cure is pituitary brain surgery.
Well, actually my head got smaller since taking vitamin K2., then again I lost 40lbs. So if the weight is the same then the head size should be the same. My dad at work played a trick on a guy who just got a raise and told everyone else. He put a one inchstrip of newspaper inside his hatband every day, then had everyone come around and watch while he put on his hat. Really freaked him out.
similar amount of Retinol vitamin A will help by boosting production of the calcium handling proteins that MK4 activates. Taking 200-400 mg magnesium and 12 mg boron will also be helpful.
In my case I resolved a 20 year case of artery calcification in 12-18 months by taking 1.3 mg of MK4 daily. So the MK4 form will be more effective and and work better than the MK7 form
such huge dose of retinol “am concerned for side effects ‘are we deficient nowadays in vitamin a at all ?
your great results with mk4 doesn’t tell me anything about mk7 would miss to give you same results “
12 mg boron? What’s your experience with boron? What form do you use?
The solution to this is to stop taking the MK7 and replace it with an equivalent 1 mg to 5 mg dose of an MK4 only form of vitamin K2. Virtually all of the time this solves the problem.
Hi Chris. Thx for great info on K-2. Perhaps you might be able to add clarity on blood thinners and K-2. You mentioned anti-coagulant coumadin. What about Plavix/clopidogrel, which differs somewhat is I believe anti-platelet. I’ve read that K-2 and Plavix will not interact. Perhaps you can address?!…
I know, I should contact my doc, but my cardiologist is useless (MI last year at 56, 2 stents, am now solidly LCHF and endeavoring to prolong life, excited about K-2’s reported mortality reduction….
Hi, I have same question. I take Plavix, aspirin and i’m not sure if it is okay to take K2. My cardio did not say anything about it when i asked. Bro, did u get answer for this ? Thanks.
I’m trying to find a supplement for mom who has very high valve calcification, specifically in the mitral valve. I’ve had her on MK-7 150mcg daily (“Solaray triple strength K2”) for two months and not sure if this is helping. Thinking we need the MK-4 as well. Is this better for valve calcification? The ones recommended may require two dosages to get where she needs and she is already taking so many pills for her heart. Thanks so much for your input. Daniel
I’m no doctor but I’ve experienced better outcomes from switching to mk4, as in the calcification on the rear of lower front teeth chips away by itself/more easily, and my skin improves. I can’t speak of valve/soft tissue calcification but it makes sense evolutionarily to me that mk4 would be more necessary and effective than mk7. I think Thorne Research drops are a good brand and they come along with D3. Add some vitamin A (or consume liver regularly). I would also suggest taking Magnesium citrate 100-200mg as well – I’ve noticed that K2 and Magnesium work better together for me. These are the only supplements I take. The book, The Calcium Paradox, explains well how these vitamins interplay with each other.
Thanks, I found Jarrow K-Right which has 1500 mcg of MK-4 and 180 mcg of MK-7, plus 2000 IU D3 along with K1 (not sure if important or problematic). Anyone seen this one?
I’ve also heard vitamin A. Can she take beta-carotene or does it need to be A and how much? Thanks again for your advice.
Hi there,
Beta-carotene is the plant version of vitamin A and nowhere near as bio-available to humans as the animal-sourced version of vitamin A (Retinyl palmitate or acetate). Liver or pâté is best, but if not consuming those things, a good supplement may help. I take 5000iu retinyl palmitate per day or sometimes just 25,000iu per week instead…
marrow is a good brand too 👍🏼
In all my reading I’ve never heard about the vitamin A importance can you please elaborate on that. Thank you Katy!
This is quoted directly from Kate Rheaume-Bleue’s book: ‘Vitamin A plays a valuable role in managing the body’s need for vitamin K2. On a molecular level, it is precisely this misunderstood role that gave vitamin A an undeserved bad rap. Vitamin D stimulates the production of vitamin K2–dependent gla proteins, thereby increasing the body’s demand for vitamin K2 and the potential to benefit from K2. That makes vitamin D a superstar because the more vitamin K2–dependent proteins you make, the more calcium you can direct into bones and away from arteries, if you have the K2 to activate those proteins. So vitamin D looks good. Here’s where things get tricky. Working together, A and D synergistically improve osteocalcin production.’
This is only a fraction of the info she goes into in her book. I can’t recommend it enough.
And this:
‘Vitamin A has a K2-sparing action; having adequate amounts of retinol reduces the demand for K2, allowing your body to get by on less menaquinone.’
Jarrow 😄
Although eating marrow (from bones) is awesome for health, too 👌🏼
Adding the Retinol vitamin A results in the formation of more Matrix GLA proteins which are activated by MK4 vitamin K2. This was used in one trial to reduce the number of kidney stones some patients were getting from high dose vitamin D3 treatment. So vitamins K2 and A work synergistically to control calcium metabolism to good ends.
Note that vitamins A and D3 are needed in a balanced proportion or ratio and there is little specific research on this. I found that an optimal amount of each was 10,000 IU of D3 and 30,000 IU of Retinol vitamin A.
There is no harm in taking Vitamin K1, but it is not needed. Vitamin K1 deficiency is very rare. Vitamin A is a good to take, but taking beta-carotene is not such a good idea.
I recommend vK2 which contains both MK-4 and MK-7. Each capsule is intended to be taken with each capsule of 5000 iu Vitamin D3
Does anyone know the best ratio of D3 to K2? For years my mom was taking 5000 iu D3 without K2 at all. I now have her on 1500 mcg MK4, 180 mcg MK7, and this is combined with 2000 iu D3 daily. Since I am concerned about not overloading her again with D3, is this balance, combined with magnesium, safe? Is 2000 id D3 daily going to put her back in dangerous territory? Thank you, Daniel
Its not an easy answer. In general the idea is to have enough vitamin K2 to activate all the Vitamin K Dependent Proteins (VKDP).
Vitamin D stimulates the production of VKDP, which is why vitamin D increases the demand for Vitamin K. That being said, there is no harm to take more vitamin D3 (up to a limit) but it wont provide additional benefits w/o having sufficient vitamin K to activated all the VKDP that the additional vitamin D3 would stimulate. Thats for vitamin D3. Vitamin D2 on the hand can be toxic if taken too much.
Another point to consider is that MK4 is more suitable for activating MGP, while MK7 is more suitable for activating OC.
That’s why its important to supplement with both MK4 and MK7.
The bottom line is that the exact ratio of vitamin K2: Vitamin D to achieve activation of all VKDP has not been determined yet and would depend on if we are talking about MK4 or MK7.
vK2 contains 5mg of MK4 and 100 mcg of MK7. We estimate this to be an optimal amount to take with 5,000 iu of vitamin D3
Eric summarizes in this post what I learned by studying the literature and Dr. Masterjohn’s summary.
One addition is that Vitamin K2 substitutes more efficiently than ubiquinol in the mitochondrial electron transport chain. Cross comparison of bicycle teams showed 7% improved aerobic performance with 200 mcg of K2 in the diet. 7% is enough to win a bicycle race. Lance Armstrong commented on his web site that a high dose of K2 causes finger tips to tingle. Mine do because I supplement with my own fermented Bacillus subtilis/liver/limburger pate. I guarantee you Lance Armstrong was taking more than 200 mcg K2 per day. I find it amusing that he was sanctioned for blood doping and testosterone when perfectly legal K2 gave him >25% aerobic advantage. ☺☺
I’m still struggling with a decision that will affect mom’s hypercalcemia outcome: She dosed 5000iu without k2 for years. Has valve stenosis. Now on mk4 and mk7 but do I even need D3? I don’t want any additional calcium in the bloodstream but rather to stabilize or remove it. Please let me know if this is correct thinking. Thank you.
Daniel, check out this YouTube interview:
https://thefatemperor.com/want-to-reverse-your-calcification-and-heart-disease-heres-how-podcast-ep21/
Might have some useful info…
The most sensitive and numerical test for progress reversing calcification and stenosis is pulse wave velocity. Accurate home testing devices were offered by Nokia for $1000 until FDA demanded an approval. Nokia no longer offers the device in USA. Smuggle one in from Europe. FDA approved devices cost $10,000. Find a clinic.
My dr recommended D3 2500 IU, how much V K2 MK 7/ Mk 4 should I take?
Best way to know, and perhaps the only way to really know is a D3 blood test. They are not very expensive and seem to be accurate.
For my clients, I look for a value of 60 ng/ml or above – I prefer 80 ng/ml as an excellent value. I have some clients in the 90’s.
I go with 5000 mcg MK4 2xDay and 400 mcg MK7 along with 5000 up to 10000 vitamin A pre-formed.
I can’t give you medical advice for your mother (or you) but these are the values I use for myself and clients. Your mother may have different goals/values.
Thank you for this great information. I am trying to stabilize or hopefully improve her stenosis and calcification without doing something that would worsen it. Mom is a bit heavy and her D3 is low, 40. I had her on 5000 iu for years without K2. Now only 2000 iu as I am afraid to bump it up again.
it seems like my values are on the low side, but she is taking so many heart pills. I hope what I am doing will be helpful, comments appreciated.
Additionally….how important is vitamin “A” for this, as I read hardly anything about it. More pills for mom…trying to avoid it.
My MK7 supplement we prefer is sourced from soy. I know there are other options but we are using this one right now because we like the other ingredients. How critical is this if you have a possible sensitivity to soy? It seems like such a small amount. Thank you. Daniel
For artery calcification several things are involved. The MK4 vitamin K2 is essential to carboxylate the Matrix GLA protein that reverses calcification. Taking the vitamin D3 is fine as this boosts the levels of calcium handling proteins. In addition, taking the Retinol form of vitamin A also results in better Matrix GLA production and this is reflected in how Retinol is able to reduce rates of kidney stones. She should also get magnesium daily.
My best guess for this series would be.
5000 IU of vitamin D3
15,000 IU of Retinol vitamin A
5 mg of MK4 vitamin K2 three times a day. More would be acceptable.
200-400 mg of magnesium citrate or a more gentle taurate.
Thank you so much all. I’m wishing I had some test feedback to determine if the vitamin regimen is working. Those scans and such are not readily available here in Pittsburgh PA. I’m wondering if I can assess mom by checking her on a monthly basis with regard to activity tolerance. I have no other way to know. Should I expect to see a change within months, or years? She was supposed to have mitral valve surgery a few months ago, and we decided too risky. Thus the vitamin and lifestyle changes.
See if you can get her eating a few carrots each week for the A. 2 average carrots/day is a nice amount to load up on, then maybe one a day would be good. My own remedy for my calcium is a whole food plant-based diet. Not for everyone, but the ones who do it, never have any more heart problems, strokes, even diabetes is eased off. The study participants who didn’t do it, most of then either had heart attack, stroke, or death in a few years’ time. But they were only 10 percent of the group, the rest had zero of those things. So it is do-able. Dr. Caldwell Esselstyn did the studies on this.
Animal-derived vitamin A is far more bioavailable than beta-carotene from carrots. A significant percentage of people can not even convert it at all! I’m a big fan of animal-based diets for being far more nutrient dense. But you must do your own research and decide for yourself.
Hi Daniel…there is a product from Forefront Health that combines these three fat soluble vitamins in one convenient bottle. It’s liquid, so no more pills to take. The ratios are good too, each serving size is 7 drops and you can take a dose with each meal if you prefer more than one serving per day. I’m not affiliated with this company, I simply think it’s a very convenient and SUPER CLEAN product that is very easy to take.
Ingredients: retinyl palmitate (Vitamin A), cholecalciferol (Vitamin D3), and MK-4 menaquinone (Vitamin K2), MCT (coconut oil)
Other Ingredients: None
One serving provides 5,000 i.u. vitamin A, 1500 i.u. vitamin D and 2 mg. vitamin K2 as Mk4.
I try to purchase when it goes on sale for extra savings.
Thank you very much, I see much information about MK-7 but not much about vitamin A in my studies. We will try to get the vitamin “A” in as well. I am wanting to have MK-7 in the mix as well based about my research. I will look into it but right now we are using Jarrow K-right. Daniel
Kind of annoying that I can’t reply to nested comments, so this is the most relevant one.
Look to nature to find correct ratios of vitamins. For example, cod liver oil (Rosita or Dropi) list their oils as having 10 times more vitamin A than vitamin D. I also heard from Dr. Shiva that we should be getting ten times more vitamin A than vitamin D. I don’t know why that is the case, but reading some of the comments here suggests that vitamin A spares vitamin K2 so that we would needs less k2 to trigger the synergy between A and D.
Dr. Weston Price referred to vitamin K2 as the x-factor, and most of his research involved native population and their diets, rich in K2, and how they’ve never seen a dentist in their lives and never developed dental issues until some of them were introduced to grains or industrialized foods.
To quote my favorite clothing brand Icebreaker:
LOOK DEEP INTO NATURE AND YOU WILL UNDERSTAND EVERYTHING.
There is no specific proportion of vitamins D3 and K2. Below a healthy age 40 we generally make enough K2 from vitamin K1 to have an adequate supply. Above the age of 40, production of MK4 vitamin K2 drops off gradually resulting in lowered calcium metabolism where bonevloss occurs and artery calcification starts. Giving vitamin K2 to young people is not likely to show an effect.
So the basis for dosing vitamin K2 would be in proportion to the symptoms of low vitamin K2. 1 or 2 mg will do a lot over time for healthy people. A 5 to 15 mg dose would be good for those with more serious health problems. If the patient is in immediate danger from bone loss or artery calcification, the most effective dose used in research was 15 mg with each meal containing some fat for a total of 45 mg a day.
David,
Would you happen to have a link for that research with that 45 mg of MK4 Per day?
Thank you!
‘Michael
Hi David,
“So the basis for dosing vitamin K2 would be in proportion to the symptoms of low vitamin K2. ”
AFAIK the symptoms of Vit K2 deficiency are osteoporosis, soft tissue calcification and kidney stones. All requiring scans to determine. How do you know how much K2 is required to reverse these? Were you getting repeated scans and adjusting based on the results?
Similarly, in another comment you said that you found the optimum amount for you was 10,000IU D3 and
30,000IU of A (seems a lot of A). How did you determine that? Does the form of A make a difference? I can only buy retynil palmitate here.
Lastly, do you have a reference for the study that used 45mg/day K2 for arterial calcification? I know they use 45mg in Japan for osteoporosis but wasn’t aware anyone had treated calcified arteries with it in a formal study.
Re: young people. I would guess from historical and almost lifelong symptoms of acne resolved in recent years by supplementing K2mk4 and Magnesium that I am genetically a poor converter of K1 to K2. I’ve been giving K2mk4 and Mg to my kids and have noticed whiter teeth and resolution of blocked pores on my tween. They may have inherited my poor ability to convert K1 to K2.
Basically, the only supplements I take are a replacement for eating liver, which I can’t abide (pity).
BTW regarding osteoporosis and bone health generally I strongly recommend the late Robert Heaney’s articles at
http://blogs.creighton.edu/heaney/
If you are not familiar with Dr Heaney he was the initiator of the long-running Omaha Nuns Study into osteoporosis and a leading authority on bone health, calcium metabolism and Vitamin C. This obituary outlines his achievements
https://academic.oup.com/jn/article/147/5/720/4584763
If I can summarise Heaney’s articles on correcting osteoporosis you need:
– adequate calcium in your diet
– adequate Vitamin D to absorb that calcium
– adequate protein to rebuild bone (bone is 50% protein and only 20% calcium)
– phosphorus since the calcium in bone is calcium phosphate. Hence the best source of Ca is dairy which already contains the calcium phosphate.
– Vit K2 to direct the calcium to your bones.
He points out that calcium is so essential to your body that it is tightly regulated and if your calcium intake today is inadequate then your body will tear down some of your bone today to get that calcium, but in the process also destroys the protein matrix. In order to rebuild that bone in osteoporosis patients you need more than 150% of the RDA of 0.8grams of protein per Kg of body weight. (So much for the RDA!)
The way that the body increases that bone teardown is through the release of parathyroid hormone (PTH). To quote Heaney:
“The concentration of PTH circulating in our blood stream is, thus, a reflection of how close our serum calcium level is to the set point, or how hard the body has to work to keep it there. When calcium intakes are low (either because the food contains little calcium or because, with vitamin D deficiency, we’re not absorbing efficiently), PTH levels will typically be elevated. And, accordingly, when absorbed calcium intakes rise, PTH levels fall, until they reach some minimum value below which they drop no further, no matter how much additional calcium we may consume. Other things being equal, a low PTH level is an indication of calcium adequacy.” Conversely high PTH implies either low VitD, low dietary calcium or both together. Heaney then goes on to show that PTH flattens out at a serum Vit D level of 125nmol/L or 50ng/ml, although with a degree of individual variation.
I mention this because when my mother’s blood test showed high PTH her GP suggested referring her to a surgeon to get her parathyroid gland removed! No mention of calcium or Vit D status. It appears that modern medicine’s motto is “when in doubt, cut it out!” Sheesh.
EXCELLENT post Stuart!!! I agree 100% and think everyone should have their PTH tested.
Thanks so much!
Tell your mom to back up forty years and eat properly. Every day should include liver, fresh greens, strong flavored fermented foods such as kefir, buttermilk, labneh, brie, feta, Swiss, Limburger, saurkraut, natto, miso, tempeh, kunjukjian, ambrosia, pickled fish, liverwurst, salami, molasses, pate, reheated leftover vegetables, hummus, kimche, pickled beets, pickled cucumbers, salsa,….
KGB, those foods would KILL anyone with histamine intolerance. Please educate yourself before posting such ignorance.
@Kelly
I know this is a really old thread but maybe someone will see my reply. You CAN eat fermented foods with histamine intolerance. Supplement with DAO with such a meal. It neutralizes histamine in foods. I also recommend supplementing with digestive enzymes to make sure.
I highly recommend vK2, which contains pharmaceutical grade MK-4 (5mg , 100% trans form) AND MK-7 (100 mcg, 70% trans form)
isent emu oil the best absorbable and bio avaialble vitamin k2 ?
Wondering what is the optimum amount of Vitamin D3 to take with 200 mcg of Vitamin K2MK7? I am on a ketogenic/keto-carnivore WOE. I live in Saskatoon, SK, Canada and am a red-headed, 62 year old woman. I have heard that red-heads make their own Vitamin D but not sure what kind. Am taking 200 K2MK7 with 1000 mcg Vitamin D3, presently.
Personally, I would stay away from D supplements.
Hi Chris,
Love your work. My own experience with K2 has been an interesting one. I’ve been using it for 3 years after stumbling into both your information online and Dr Kate Rheueme-Bleaue’s book. It coincided with when I first started eating low carb, healthy fat. At first I noticed improvement in my nails when consuming significantly more grass fed butter and that’s when the whole K2 a-ha moment occurred.
I’ve experimented with both K2 MK4 and MK7 and found the effects of using mk4 far superior, measurably so. I think it lines up well from a evolutionary standpoint and is probably why mk4 is used up so quickly by the body.
I would also bet money on me being a super-lousy genetic converter of K1 to K2.
Benefits of mk4 vs mk7:
No dental calcification – the stuff literally chips away once I change to mk4.
Significantly improved skin – back and facial acne disappears.
As long as I take K2 *with* daily Magnesium, my 40+ yr nail biting habit literally stops. I’ve tested this a number of times, if I stop taking either K2 (either mk7 or mk4 do the job) or Mg, the urge to nibble my nails creeps in over about a 10-14 days. Once I resume taking both supplements, the urge to chew goes after about 2-4 days.
The only supplements I take daily are:
K2(mk4)/D3 Thorne drops (5-10 drops twice a day)
Magnesium citrate (100mg)
Vitamin A (5000iu)
I probably won’t bother with K2 mk7 supplements anymore as I eat plenty of the relevant cheeses and/or sauerkraut, and I’m convinced they’re less important than mk4 anyway….
If only I enjoyed eating liver, I could drop the supplements altogether 😆
Oh, I forgot to add…
I’ve been giving my kids the same K2 as me for the past 3yrs so : 6-9mths of mk4, then a switch to mk7 for about 18mths and now a recent switch back to mk4.
They’re teeth are measurably whiter when taking mk4 compared to the mk7 (which made zero difference). Takes about a month to see difference.
My 8yo son recently had to see a maxillo-facial surgeon regarding an underbite, and we’re going to leave it a year and have another look in 12mths time. I’m very interested (and hopeful) that switching back recently to K2mk4 will contribute to an improvement (although we’ll never know for sure if it was the K2 that made the difference or just normal growth correction – fingers crossed, I’ve heard of adults online claiming improvements of jaw structure using K2… we’ll see…).
Regarding underbite and jaw structure, look up an Orofacial Myofunctional Therapist in your area. Exercises are very effective at correcting jaw structure in young children!
You could also looking into mike mew or mewing /oral posture for facial development
So interesting about your nail biting, because I’ve also noticed magnesium affects that for me but lately it hasn’t been helping. Do you take all 3 supplements at the same time? Have you ever taken them on the same day but at different times to see how that affects? Also, what time of day do you take them? I’ve noticed timing can have a big impact for my sensitive body. Thank you so much in advance!
The fact that other than a few specific naturally occurring foods have high levels of K2 leads me to believe that an assumption that 100mcg a day is needed or 200mcg is not based in reality. The reality is that it seems you would be lucky to be able to get more than 50mcg a day without actively trying to consume multiple foods on this list, which I am sure people historically did not have access to all of these foods at any given moment like we do today. If you get to page 12 you see that the levels in foods vary widely. Given that Weston Price had such great results when adding in small amounts of butter oil and the levels vary widely from one butter to the next leads me to believe only small amounts of vitamin K2 are needed.
Sir,
Humans evolved over more than a million years. During that period the bulk foods were fresh vegetables. High K2 bacillus subtilis are swimmers moving up plants toward oxygen during rain. Green leaves and fresh vegetables are high in Vitamin Kf2.
In addition the primitive food over a million years was a community porridge recooked day by day. Bacillus subtilis are heat resistant spore former not toxic and they produce plentiful Vitamin K2 during cool porridge periods.
Lance Armstrong reports that high intake of K2 causes the fingers to tingle. He should know. He had an aerobic bicycle lab in his home. He titrated his bicycle aerobic performance versus intake of multiple supplements by sending out blood samples for analysis. He won 5 Tour de France races.
Independent physiological athletic research comparing bicycle teams with and without 300 micrograms per day of K2 showed 6% improvement of aerobic performance on this low dose of K2.
I take enough K2/day to achieve tingling in my fingers. I grow my own Bacillus subtilis and blend it into a liver/Limburger cheese pate. I dare say I get more than 1 mg/day. I cannot afford outside analysis like Lance Armstrong.
I suggest to you that OVER 1 mg/day of K2 was the norm over a million years of human evolution.
K2 might have played a role in Armstrong’s career but EPO, steroids, etc were the elephants in the room. He’s worthless
Industrial farming helped kill K2 in our diets (here in the USA). I’m sure our natural K2 intake was a lot higher eating grass-fed meats, grass-fed butter instead of factory farmed grain-fed meats/butter. If one had a healthy diet with a combination of grass-fed meats, grass-fed butter, eggs, and the right cheeses before our grain-fed factory farming took over the country, I believe our K2 intake probably rivaled a diet high in say.. Natto consumption like parts of Japan. At the very least, we weren’t deficient in K2 (before factory grain-fed farming).
I read on nutritionfacts dot org that in former times our diet included bugs, dirt and feces, all high K2. We make it in our colons, but it’s too far down to be absorbed. Termites are loaded with K2 and gorillas crack open rotting tree trunks and logs to get at them.
I would suggest;
Vitamin K2 and the Calcium Paradox: How a Little-Known Vitamin Could Save Your Life;
Kate Rhéaume-Bleue, BSc., ND
I am personally on the WFPB &No oil bandwagon…i know and understand a lot of people are on the paleo/carnivore/ alike bandwagons.
I am no fundamentalist, no strict vegan and no preacher. I take several supplements and vitamins.
Anyway as a whole food plant based person consuming little or no oils…. i wonder how to get good absorption of K2….
i understand with meals with saturated fats would be best. So which non-animal -whole -foods might best be consumed to eat with vitamin k2 caps besides avocado? Cause i cannot purchase those here. Please do not suggest oils.Thanks
Hi, Brenda, I am on WFPB also, with no added oils. I add ground flax seeds to my green smoothies for fat-soluble nutrient absorption, if that’s any help.
BTW being whole food, I add natto to my green smoothies as well to get the whole package of K2, plus many other things, enzymes, etc from the natto. I hate natto, but added to the green smoothie it’s ok. Here’s the formula for about 3 days worth smoothies: greens (various, kale, spinach, chard), natto 2 packages, 1/2 tsp baking soda, 3 tbsp. ground flax seeds, few sprigs basil, few sprigs mint. I buy basil and mint in big bags from restaurant supply cheaply. Top with ground nutmeg.
I also take “Koncentrated K” which has all the K types in large daily amounts economically in addition to natto, since it appears K isn’t harmful in typical amounts. The product has 500iu K2 mk7, 25mg K2 mk4, some K1 too. It’s about 45 bucks for 2 mo supply (60 caps).
Bob,
IMO, “Koncentrated K” has way more MK4 and MK7, than is desirable. It also has Vitamin K1, which virtually noone needs to take.
Do you happen know what color the ingredients are? If not yellow, than its not likely to be pharmaceutical grade.
The capsules are pale yellow. The maker/seller is a professional chemist. The dose of 500ui/day is within range of the 360iu/day used in clinical trials by Dr. Shurgers in Netherlands. 360 was the lowest dose that would fully carboxylate the MGP of all subjects. He would’ve used more than 360 but laws over there limited it despite no evidence of toxicity. The maker checked all of it with Shurgers, and himself takes two of the capsules per day. He also tested to affirm that some of the MGP remained un-carboxylated, which he says it essential. Hope that helps.
the CONTENTS OF THE CAPSULES ARE PALE YELLOW, NOT THE CAPSULES THEMSEVLES. sorry.
Thanks bobluhrs for the suggestion ground flaxseed is indeed a good option,very healthy too….
I will look into the k2 source you mentioned. Natto inwould.like to try; but is hard to get hold of here. Should be ordered and all and logistics here are suboptimal.
Sure. I’ve seen online info about how to make natto at home. Just soy beans and a starter bacterium. Once you have some you can make all you want. It was made by accident in Japan when they wrapped their soy beans in straw and buried them, came back and found all this goo around the beans, but ate it anyway, and from there it became a huge fad, nobody remembers why. Half of Japan loves it and the other half thinks they’re daft. Good luck, though your time of depending on luck is over with what you’re doing. So good luck if you need it for something else, I guess… Calcium scores always go up a bit while the body disposes of plaque (80 percent is soft plaque) it throws in some calcium to stabilize the plaque while it melts away. This is from Dr. Wm Castelli of Framingham Study, as reported by Esselstyn. Enjoy your miracle.
thanks for your response
How would you compare their shade of yellow to the one on the link below?
not to beat a dead horse, but
my point being that the more pale the yellow is, the more likely it is less potent.
It may not be valid to compare a photo to an “in person” view but regardless how do they compare?
I looked at their website but didn’t find any pictures of their capsules to compare the yellow color. Mine is pale yellow about straw colored. I know the maker, spoke on the phone with him, he started with the calcium score and that’s why he created the product, to save his own skin. He’s industry veteran chemist seeking to provide a product that covers all the K bases below the cost of the others. I doubt he’s a cheat at all, nor that the other one is, either. I also take natto, and another brand of MK-7 at 100 iu/day from ‘nattopharma’ named menaq 7. I’m sure all these sources can criticize the others to where you’d buy from them, that’s just marketing reality. So I use a few sources, since I think K2 is a good vitamin to supplement, just a vitamin, however, and won’t fix plaque much at all on the US diet. The body will override any attempt to remove calcium it has placed there to stabilize plaque, unless the plaque itself is removed, then the body will throw more calcium at the soft, degenerate plaque till it’s gone. THEN and only then might the vitamin come in handy to normalize the calcium. Maybe. It’s just my thinking, certainly not an expert.
With that amount of K2, is it a problem with how much Vit D I take? I only take 2000 IU a day.
As I understand it, and have read about it, vitamin D tends to increase body’s production of MGP and osteocalcin, among other things. K2 then reacts with these to improve osteoporosis and retard calcification of soft tissues. 2000 is plenty of vitamin D according to some, and not enough, to others. Dr. Fuhrman recommends 2000, the D association, 5000. Another guy, Dr. Eric berg says he clears calcium from people using 10000, plus 400 of K2 MK7 for a few months time, then lowers the dose of both, I forget the details. He’s not one of my favorite sources, sort of messes around without documentation or discipline, but he hasn’t killed anyone I know about.
I strongly disagree with bobluhrs.
If one isn’t getting enough calcium in the diet, it is pulled from the bones, creating calcification/bone spurs. Yes, calcification may happen from not enough vitamin D and or possibly K2, but K2 may lower blood calcium levels as Chris has noted above, something one DOES NOT want if they’re deficient.
Off topic, but Furhman is a joke IMO, and Berg not much better. I’d like to see his published studies showing those kinds of results.
I am not worried about calcium deficiency, don’t think many actually are unless their diets aren’t sufficient. I eat plant-based and get plenty of both calcium and potassium and no animal protein to create metabolic acidosis and rob bones of calcium. I don’t have low calcium in blood. If K2 lowers it, maybe because it steers it from the blood into bones and teeth where it belongs, and the person needs more of it. Off topic, I don’t think Fuhrman’s a joke at all as a doctor, his patients appear to be doing quite well, especially when you consider where they started out, though Berg I can agree on. Fuhrman’s a hypothesis generating type of researcher not a proof type, he doesn’t conduct studies, only summarizes and conjectures, which is quite common at early stages of discoveries. If it’s not then tested properly you can’t rely totally on it, which is where he’s at currently. I heard there are some studies on his diet underway, not sure how much finished.
Eric & Bob’s info is not current…go to koncentrated K website for better info! L
The reply button in the thread below is gone so i put my response here.
Anyway Fuhrman is very knowledgeable, no joke at all. One of THE smartest doctors out there, so do not insult him.
In fact many normal doctors ARE a total joke, ( i work in a hospital , traditional doctors know next to nothing of nutrition, they will advice cow milk and cheese for bones like most nutritionist so they have like traditional orthodox views you might say)
but Fuhrman is far from it.
He and Esselstyn, Klaper, Greger, Mc Dougall, Pritikin and a few others deserve a medal. They belong to the tiny group of doctors which are not money or ‘incentive’ driven…. There is no money to be made from good advice and good foods.
They managed to reverse lots of cardiovascular dieseases, no statins or other drugs ever managed that. Pritikin himself has a very special story, sad ending, but very very special and fascinating.
I think the paradox is THE most unhealthy foods, also contain a tiny little K2. Loads of saturated fat and a tiny speck of K2 to counter it? That just won’t cut it today.
Some time ago i got really interested in dr Joe Prendergast, he treated people with massive doses of Vit D. Of course people will say he is a joke too, they always do and will do with people who are out of the mainstream. You might want to try telling your family doctor you take K2, he or she will not even know what K2 is or does in 97% of cases nor know anything about dosage etc. Anyway, Prendergast was or is a endocrinologist and had lots of success with treating diabetics. I guess i got into him because of Bobluhrs here LoL .Anyway all you meat- chease- dairy eating keto believers might want to look into him too.
Very special indeed.
Don’t believe me, just find out for your self, same with Pritikin. Mc Dougall and Klaper, very special and fascinating stories that share 1 common trait: they often had major health issues themselves in youth.
bobluhrs, you might want to read up more on calcium. It doesn’t just belong in the bones and teeth — your muscles need it to contract AND relax. Not enough calcium and you get tetany, and extreme contraction of the muscles.
Brenda, I doubt I’ll convince you of anything, but humans are omnivores, not herbivores. That’s a fact.
Now certainly if one eats too much muscle meat then that can create acidosis, where minerals are pulled from the bones to try to correct that.
But we NEED dietary cholesterol. If you don’t believe me, ask Chris. Studies have shown that a cholesterol level below 175 greatly increases the risk for depression and anxiety. And the fact that one does not get that from a vegan diet probably explains why McDougall has become so unhinged.
Don’t believe me, then check out a video on youtube, entitled “An Explosive Interview with Vegan Expert Dr. John McDougall”. The man snaps at almost every question and is clearly unable to settle down.
As for Furhman, a friend of mine who is very ill with ME/CFS has gone downhill markedly since starting Furhman’s restrictive diet 6 years ago.
We’re not herbivores.
Well said. My wife and I followed Furhman’s program for two years. Mainly looking for a solution for my wife’s isolated systolic hypertention. My wife was even seen by Dr. Fuhrman at his office for the cost of $500. We thought he would give her a personal protocol something designed more for her but he never ordered any blood tests or other tests and he had nothing to say that wasn’t already in his books even though her systolic blood pressure was 205 while in his office. Sorry but I don’t consider that to be a great doctor. Waste of money and waste of time. She has found a solution since then and for the past two years her blood pressure has been normal after following Morley Robbins Root Cause Protocol.
I agree we’re not herbivores, not carnivores, either. We’re frugivores (fruit, root, veggie). Our jaws move sideways, while true omnivores like dogs and bears only move up and down. The fact we ate so much variety is likely due to our wide ranging travel and migration; we’re everywhere. But for the longest time we were like the chimps, our closest relative in what we ate, 23 million years, not 2.5 paleo period. Not much changed over the 23. Our gut is 9 times body length, while omnivores is 3. You can’t give a dog heart disease with fatty meat, but a series of chimps fed like that died in under a year from it. We last longer, but are not proof against it.
Off-topic, I don’t do all of what Fuhrman says, just the nutrient attentiveness. His diet, to me, restricts calories too much for the sake of micronutrient load maximization. I think that’s good for about 6 months, after which the body’s probably saturated and has shed the extra pounds. Now what? At that point, compensation has been reached for nutrients, so now you need to work out how you’ll get your calories, macronutrient load.
Take my case, a bad calcium score for motivation 579 three years ago. My doc offered a cardiologist, I asked for 6 weeks. Did Dr. Esselstyn’s diet with an eye to Fuhrman’s micronutrient rating scale (ANDI), used by Whole Foods. Esselstyn’s video on youtube “Treating the Cause…” will explain why his diet and the success rates in human trials over many years. I’m not saying this is for everyone, it was the best track record against what I’ve got. If I become a McDougal, just shoot me. He needs a good hot meal ala grandma. I think compensation to correct dietary problems then readjusting things for a good balance makes the most sense. I think the mind will clear up and some people may find themselves pissing others off, so they should watch out not to be upsetting. I have found my depression/anxiety has improved over the 3 years, but not assuming that’s going on forever, it could be compensation effects. I always try to self-examine and revue. In order to get my stuff right, I use the nitric oxide remedies of Prendergast, Rainer Boger, and research of Dr. Robert Vogel, U of Md on FMD (flow mediated dilatation) saying which foods restrict and which promote it. That way, if I need something not on my Esselstyn diet, I can take some of that technology with the meal to guard against the effects. I believe some animal product on a very irregular basis might offer benefits, however, as a steady diet (something nature never anticipated) it seems to encourage bad bacteria that produce TMA, which the liver oxidizes to TMA0, which directly causes coronary artery disease. It takes about 2 weeks for the bacteria to become established, as tested on vegans who were given steak every day for 2 weeks (anything in the name of science). I’m not vegan, but get splashed a bit by the similarities. Anyway, my fight is deadly and highly motivating that much is for sure, and so is that of lots of others.
Prendergast is interesting in that he used a blend of arginine and citrulline, but not much citrulline, that was wrong. Rainer Boger (dir of pharmacology U of Hamburg) found by experiment that a ratio by weight of 2 arg: 1 cit resulted in the largest rise in blood levels of arginine. But even with Prendergast’s inferior formula, which resulted in his patients taking a big dose, about 4 times what’s needed if the 2:1 ratio is used, he still got 20 years with 7000 patients, 80 percent with diabetes, having NO admissions, means no heart problems. That is unheard of. To dismiss that would be insane, I’m using it. My blood pressure is usually 110/70, and some of that probably comes from the arg/cit mixture I make for myself. It will take a combination of things to roll back what I did the first 70 years at the table, if it can be done at all.
@NevadaSmith, i am really sorry to hear that. It was not what i expected.So thanks for the info.
i am happy the Morley Robbins advices worked out for her high blood pressure. I know a lot of diets do not work for everybody. I agree on a lot with Fuhrman and colleagues cause i see a lot of lifestyle related cancers and diseases- the big lines-, but then again it obviously does not work for each and every person. I agree with the big lines, not with all. For instance being dutch i have a hard time leaving out butter like now, if the cows are outside eating fresh grass it must contain K2 and lots of other goodies. So much religion and dogmas, maybe in 20- 50 years food will be highly customized to individual patterns/ genes. Thats what i expect, but i am not sure. I also recognize that in a lot of more neurological issues the ‘good’ fatty acids are really important, and those tend to be pretty low on certain diets, especially on WFPB diets. Anyway i have a hard time connecting Weston A Price ( the man himself not the modern adepts of it with lots and lots of meat and fat, ) and people like Fuhrman, I know they both are right on a lot- in their own right-. Anyway fat soluble vitamins are important, thats why we are on this page.
Who knows the role of pollution, plastics, hormone disruptors, obesogens and thousands of other chemicals we are exposed to daily?
Fact is almost all those substances are fat soluble. I sometimes wonder if that might be part of the puzzle explaining why WFPB and no oil brings down so much diseases( but not all). The more up the food chain, the more pollution,
I will look into Morley robbins, i know too little of him.
Tanta celeuma e de complicado, é tão simples.
Vitaminas A, D, e K1 e K2 , E,…sim, SIM! mas sem magnésio as enzimas não funcionam. ” A alimentação dita ocidental tem 10 vezes mais Cálcio que o Magnésio necessário para o metabolizar”. Veja J. Durlach, M. Sircus, Masterjohn, Univ. Tufts, W. Price e muitos outros e, a prazo, constatando os resultados que isso traz. Só com a adição de uma pitada de Mg (600mgx70%=420mg)diário, as outras já funcionam bem melhor. Ele é determinante. Eu curei-me depois de 4 episódios de enfarte. Com 6 stent, andei perto de entregar a alma ao Criador!
Para anedota pode ser, viver sem a K2 da gordura animal. Mas hilariante mesmo, pode ser, depois de procurá-la, a seguir destruí-la com varfarina e sucedâneos; sem o Mg, a A e a K, como o cálcio não vai para onde faz falta, forma placa nos vasos; depois é correr atrás do prejuízo, pôr ancas de platina, a calcificação dos átrios cardíacos, ‘curar’ o enfarte, medicamentos para contrariar as defesas do sistema, tensão alta, diabetes a prazo… ah! ironia, mas mantendo a aterosclerose. Interessante, não é?!
Depois de 6 meses de desmame aos medicamentos , ganhei-lhe o jeito. Acho que percebi. VIVO há vários anos sem qualquer droga , sem queixas, colesterol total 254, nem dietas especiais. O meu cardiologista até podia por as mãos na cabeça… mas eu nem vou lá, faz mais de 3 anos!
Acho que perdi os stent. Ao fim de 1 ano deixei de os sentir, mas não esqueço, todos os dias, 300 + 300 mgr na água.
hi , what about California Gold and Solgar ?
Hi
I love your podcasts and vitamin emails; thank you so much for your devotion to helping others. Question, I am presently taking a Vitamin K2, (Relentless Improvement). It has 15,000 mcg of MK-4 (12.500%), and 60 mcg of MK-7(50%). 1 serving size. In your email and on your website under Vitamin K, you mention taking 100- 200 mcg. You mention on your website if I don’t get K from enough foods you recommend getting closer to 200 mcg. I have osteoporosis, and kidney stones. ( Not kidney disease) and probably need the 200 mcgs. I am not on any other medications, & my bones have remained stable for 1 year since my last bone density test. My bottle says “15,000 mcgs of MK-4), which is very different from the 200 mcgs you are recommending. I thought it was strange so I wanted to ask should I stop taking this vitamin? Or am I not reading the numbers correctly. Please I would appreciate your advise. Thank you so much.
I’d like to let you new about a new vitamin K2 product (vK2). It contains pharmaceutical grade MK4 (5mg) + MK7 (100mcg).
If the brand of Vitamin K2 you take is NOT yellow, then its not pharmaceutical grade and probably contains Chinese ingredients.
Do you believe Relentless label claims? for their price, i think it is very doubtful
The capsule is yellow in color. There are so many vitamin companies not sure what to believe. However, I do trust Dr. Masterjohn and his responses as I have been watching and learning and researching for some time. I was concerned with how much is okay to take and it seems like 15,000 mcg of MK-4 is much higher than Dr. Masterjohn would recommend. Just want to make sure I am not hurting myself in some way. I liked the product because it has clean fillers. But would buy elsewhere if these are too high in dose.
What is the make of this new brand Eric? if it is ‘vk2’ then it is a poor choice…nobody will be able to find it online…
Also how come the pharmaceutical grades are (always?) yellow
Yes, Brenda the Product name is vK2, which can be found on Amazon by searching for vK2. It is distributed by NHS Global Distributors (http://www.nhs-global.com)
The MK-4 we use is pharmaceutical grade, meaning pure (The assay specification is 98% – 102% with the current lot test value = 100.6% by HPLC ) and the MK-7 is in a 1% potency (with 99% Microcrystalline Cellulose)
The pharmaceutical raw materials, must be cold stored (turns into liquid if over 100.2 f) They are not only expensive, but must also be shipped to our lab in a cold shipping engine, which adds an additional expense.
The raw materials are VERY yellow, but are not stable until “cut” with microcrystalline cellulose, which results in a temperature stable yellow (but more pale yellow than the uncut raw material)
The less pure (or more cut) the material, the less yellow it is
Hi Eric,
I do like the product you recommended, looks promising and the reason for it as described on your website I am familiar with. VK-2. My dr has me on 2000 IU of Vitamin D3, not 5000. And she is not ready to increase my dosage. So with this in mind; your K would be too high of a dose for me. I really appreciated your insight and info on this vitamin K; but need to find one that fits my regime with the amount of vitamin D I take. Still looking for a better Vit K2- with MK-7.
Hi Janet,
Your doctor is ignorant of vitamin D3 requirements. She is a trained ambulance chaser not a health practitioner or nutritionist. 5,000 IU Vitamin D3 along with 300 micrograms K2 and 5,000 IU natural vitamin A is necessary for prevention of a host of age related diseases. Among these are arthritis, osteoporosis, Alzheimer’s, periodontal disease, atherosclerosis, stenosis, cancer, bone spurs, dementia…. Medical schools do not teach health and nutrition. Medical students are taught that they pop out of the box knowing everything there is to know. They do not read for improvements in the state of the art. They never learn. My advice is to find a conscientious nutritionist or Nurse Medical Practitioner to guide you. You can also read the literature and YouTube for expert science behind the combination of Vitamins K2, A, D3. Doctor Chris Masterjohn is an excellent resource.
Hi Janet, Sorry for my delay in responding, i did see your comment till just now.
I’m not sure why your doctor is recommending such a low dose of vitamin D3, but regardless, there is no harm in taking more vitamin K2
Hi! Thank you for this awesome resource! I’m wondering what your thoughts are on the Just Thrive K2 supplement. Consider adding it to the review above? Thank you!
Does nattokinese contain k2, as natto does?
My 15 year old daughter has been diagnosed with pcos I don’t want her to be in the birth control pills all her life she is not fat and her sugar levels are normal. I would like to know more about vitamin K2 and how this vitamin can help with the pcos. I think this condition or syndrome has been for many many decades and very little to nothing has been done to help or cure it.
Look into iodine for pcos, the fertility Friday podcast on YouTube has an interview with dr Jorge fleachas about it.
I had a Calcium scan done and got a score of 46. So I started taking 320mcg of Vitamin K2-7 a day because I read it will help reduce the calcium build up in your blood vessels. I have been taking them for a month and in the last week my stool has gone from dark to blond color or very light beige if you will. Is the K2-7 causing this color change and should I been concerned?
Are you also taking Vitamin D3? I hope Dr. Masterjohn will answer you as he is more knowledgeable.
Curious about a comment in the content of this article that suggested MK-4 might be best for distribution…or lack thereof…in soft tissues. Would that indicate MK-4 could be of more benefit for arterial health (preventing calcium/plaque buildup) than MK-7?
More research needs to be done in this area, but my money is on mk4 as that is the animal-sourced component and makes more sense evolutionarily to me. I’ve experimented with mk4 and mk7 over the last 3 yrs and I have visibly better results with mk4 (teeth and skin). I have been very consistent with my intake.
Doesn’t it make just as much sense whether you are looking at it from an evolutionary standpoint or not?
I am taking CV meds. Metoprolol,Losartan, Clopidogrel and Atorvastatin. Is it ok to take k2 and what do you think a safe dose would be? I would also like to take coq10, any thoughts on that? Thank you, Chris jensen
The blog is really appreciable and inspiring. Helped me a lot. Hope same sort of blogs in future too.
https://goo.gl/XZYCpS
Greetings, do you have commentary on, or could you comment on the relationship of K2 to any decrease in calcium in the brain? Previous to K2 supplementation along with increased consumption of olive oil and the probiotic bifidobacterium infantis, (a microbe known for producing seretonin) my 77 yr old mother was experiencing full on episodes of Alzheimer’s-like agitation and disordered thinking, ( logic-splices, child-like Behavior,etc) approximately every third day on average over the course of 2 months. After beginning her supplementation of the above mentioned items she has experienced only 1 episode as described above in the two months following this new protocol, and that one episode occurred within the first two weeks of beginning the protocol. I’m happy to add that mom is back to laughing at jokes again. Btw, She takes meds only for thyroid and blood pressure.
Craving more knowledge here, thank you for your informative and very helpful website.
Jamie
Hi Jamie, like yourself I would like to know more. Interesting about bifidobacterium infantis. I am hypothyroid and take calcium supplements and have wondered about the effect on the brain as well.
Maggie
Very interesting article. Do you have any thoughts on the Relentless Improvement MK4 and MK7 that is derived from orange jasmine blossom?
I’d like to let you new about a new vitamin K2 product (vK2). It contains pharmaceutical grade MK4 (5mg) + MK7 (100mcg).
If the brand of Vitamin K2 you take is NOT yellow, then its not pharmaceutical grade and probably contains Chinese ingredients.
Do you believe Relentless label claims? for their price, i think it is very doubtful
The capsule is yellow in color. There are so many vitamin companies not sure what to believe. I do trust Dr. Masterjohn and his response. I was concerned with how much is okay to take and it seems like 15,000 mcg of MK-4 is much higher than Dr. Masterjohn would recommend.
vk2 has 5mg of MK4 and 100mcg of MK7
i just dont see how its possible to sell what Relentless alleges to contain for their price
Great read. My mom has high levels of aortic and mitral valve calcification as well as arterial. It is symptomatic now, and I have her on 150 micrograms of MK-7 but wondering if we can help her better with a full spectrum product. We only have a few months to test this, since doctors want to operate and she doesn’t want that. What is your opinion on fastest way to remove the calcification? Thanks so much for your response.
Might be a good resource:
https://www.cureality.com/library/booklets/Track%20Your%20Plaque%20Program%20Guide.pdf
Thank you very much !
A better source for all types of supplementation is Chris’ friend Kamal Patel’s Examine.com.
Here’s a quote:
“Although K1 is directly active in your system, your body can also convert it to MK-4.”
https://examine.com/nutrition/supplementing-vitamin-k/
Thank you for a very informative explanation of vitamin K2.
I gather from reading this information that it is better to make use of BOTH
MK4 and MK7. I use the Thorne Research MK4 ( 1 drop = 1mg) and take 1 drop
three times a day. Am I taking too much?
Would it be beneficial for me to also take 200mcg of MK7 as
well. I am 69 years old (female) and have osteoporosis. My daily calcium intake
is 1200mg.
Thanks ……….
Thanks so very much for the great informative information. What I really really want to know is which K2 supplement you take!
Is there any research on transdermal absorption of K2?
I have been squeezing the contents of gel capsules containing mostly K1 and k2 at a rate of about 300 – 400 mcg per day (half k1 and half k2( mostly MK-4 with less than 15 mcg of MK-7) and applying to wrists, knees and soles of feet on alternate days. I don’t know how this converts to international units, or how much is absorbed into my system, nor whether this is a good proportion to keep calcium moving into my bones and not in my arteries. The water in my area is very high in calcium and low in magnesium.
Since each capsule contains over 2000 mcg of combined K, I wished to reduce the amount taken at one time to a reasonable level.
I have to take K1 to balance the Warfarin I take for a heart valve. I run 2.5 INR b y adjusting my eating of greens. I’ve learned to cheat by eating spinach for two days prior to a test. I could find nothing on K2 impact on INR.
I knew that K1 is water soluble and only in your body for 8 to 12 hours before getting peed out or sweated out. I reasoned that left 12 to 16 hours without K1. K2 is oil based (and ferment & meat). This stays in the body for 3 to 5 days. This left the issue of interference with the Warfarin.
So I tested it. I kept the K1 level while consuming a lot of K2-M7. The results are that there is NO impact on the INR or Warfarin. I now take K2 every other day, figuring that each cap is active for 3 days.it’s been working fine for 6 months. I’ve tried as much as 5x everyday without any effect of the INR.
So only leafy green veggies effect the K! and INR. A heavy dose of K!1 Is gone in half a day with half of the Warfarin untreated. Therefore the Leafy greens should be eaten at least twice a day. This is while the K2 can be effective for 3-4 days. The general suggested dose of K2 is 2 caps a day. This results of 8 cap active in the body unless spaced out. It will also activate any beans eaten, with pronounced fermentation.
I am on warfarin because after a spinal cord injury 6.5 years ago I have quadriplegia and now have a propensity for blood clots. I recently started supplementing vitamin K2 mk7 ( doctors best MenaQ7) at 200 µg per day and my INR dropped and I had to raise my warfarin level about 15%. I am planning to add in MK4 to see what effects it has.
I take NATURE PLUS Vitamin K2. It has MK-7 only. Do you recommend both MK7 and MK4. Are is this supplement a good supply of Vitamin K2 without having to take a MK-4?
getting intoxicated from eating liver every day ?
which liver beef or chicken or else ?
guess wasn’t grass fed liver was it ”
how did you trace the toxicity direct exclusive to the liver eating ?
Chris, outstanding work! As a lifelong student of nutrition and wellness I realize I have learned nothing about the importance of Vitamin K2, until now. Thank you, this has opened up entirely new avenues of thought.
Thanks Mark!
Hello, Dr. Masterjohn,
I recently gave birth to my first child (I’m 25). He has a bad overbite, which has really surprised me given my consumption of vitamin K2. I’ve been eating two eggs a day basically all my life and drinking raw milk for a few years. During the pregnancy around 4-5 months I began eating four eggs a day, beef liver once a week, and a liter of raw milk daily. Before even getting pregnant I had started 200 mcg of vitamin K2 MK7. I’d also been taking 5000 mcg of vitamin A because of a vitamin D-induced deficiency as it seemed to me. In the end I think I overdid the vitamin A… my skin has reacted strangely.
I’m wondering how this could have happened? Could excess vitamin A have interfered? Was it more likely a problem of fat malabsorption? Could the supplement I took be a scam? Here is the link: https://www.sunday.fr/vitamine-k2-mk7/vitamine-k2-mk7-goutte-100mcg-100-pourcent-all-trans-vegan.html
I really appreciate any help. I wonder if there is a way to develop his jaw better from here. Should I try increasing the drops to 400 mcg? Thank you.
I’m not sure what causes overbite, sorry.
Hi Casey,
I hope you don’t mind my thoughts on this.
It’s quite normal for a baby to have a slightly retruded mandible. As they develop, the mandible should grow in a forward and upward direction – so it usually corrects itself if conditions are right for it to do so. Of course, there’s always a chance that it’s currently outside what is considered normal – you’d need someone to look at it and give a diagnosis.
There are multiple factors that influence facial and jaw development. Including: the action of breastfeeding, breathing and nutrition.
The position and actions of muscles and positioning of the tongue have a huge impact on jaw and tooth position. Breastfeeding encourages the proper function of these structures.
A recessed mandible can be influenced by mouth breathing. As a general rule, all of us should be breathing through the nose with a pair of sealed lips, including babies. (Unless you have a cold!) If a baby is mouth breathing then this should be investigated and corrected.
Nutrition sets up the baby to perform these things (above) in the best way possible.
May I recommend that you check out Dr Steven Lins website. He’s a dentist with an interest in nutrition and development and his website is a fantastic resource. I often refer my patients to check out his info.
Cheers.
Teresa,
Thanks for your reply. I did read on a site about breastfeeding that most babies have an underbite. That’s interesting yet strange. I hope my baby’s bad latch, which I need to get taken care of, isn’t affecting his development.
I agree about mouth breathing. He has his mouth open often but I don’t think he’s actually breathing through it.
Hi there,
A bad latch can often be caused by cranial and cervical dysfunction. I’ve treated a number of babies over the years who had latching difficulties and they were easily resolved With a little bit of cranial work. My infant cranial teacher is Carol Gray and she lives in Portland Oregon her website http://www.carolgray.com has a list of practitioners that she has trained.
My buddy Michael Hahn practice is in Seattle and he has treated a ton of babies over the years with all sorts of difficulties like Latching difficulties and torticollis and sleep issues issues and reflux and much more.
It can certainly be worth having your baby evaluated because at this age many things can be fixed really easily.
How does Vitamin K2 work with Proteolytic Enzymes and can they supplement together. How does Vitamin K2 work well with Vitamin D 3?
Hello Chris, Great article! Thank you for writing this.
I have a very limited diet because I have TMJ disorder (arthritis of the jaw joint) and this makes eating and chewing very difficult.
Currently, my only source of Vitamin K1 is organic hemp seeds and organic Barley Grass powder. And my only source of Vitamin K2 is a Multivitamin supplement containing MK-7 (soy-free) and organic grass fed ghee.
I have some dental problems, including slightly bleeding gums and slightly eroded enamel, and slight teeth sensitivity and reduced saliva. Many dentists believe this can be caused by Vitamin K2 deficiency.
I therefore want to buy a new supplement to increase my Vitamin K2 intake.
Which product would you buy if you were me? The Life Extension Super K, or the Innovix Labs Full Spectrum Vitamin K2?
Note: Life Extension have recently changed their formula. Their product now contains 100mcg of MK-7 which is 100% in the trans form. I emailed them and they confirmed it is 100% trans MK-7. You can see the new formulation here:
https://www.lifeextension.com/Vitamins-Supplements/item02034/Super-K-with-Advanced-K2-Complex
I look forward to your reply.
Thank you so much in advance,
Tom White.
Hi Tom,
I hope you don’t mind my 2 cents’. I’m a dental hygienist so your comment caught my eye ☺️
I personally use Thorne Research’s combination D3/K2 supplement. It’s liquid and comes in a dropper bottle which means you can add it easily to a cup of water etc.
I have no comment on if it’s better or worse than any competing brands but my understanding is that Thorne are high quality.
All the best.
Thank you Teresa. I have decided to purchase the Life Extension product.
I was familiar with the Thorne product you mentioned.
Generally speaking, I like to buy individual nutrient supplements so I can monitor my symptoms, health and test result levels, and then “tweak” the dosages as required.
I have previously taken the more expensive Thorne MK-4 without the D3, and noticed some positive improvements.
On this occassion, I have elected to go for the full spectrum Vitamin K product by Life Extension purely because I want to minimise the amount of capsules and tablets I am taking currently, which is at least 10 or 15 different supplements.
If I am dissatisfied with the results from the life extension product after 2 to 4 weeks, I will take a different product.
Thank you again for your comment.
Take care.
Please see my supplement review in this article.
Thanks for your reply. I have read the full supplement review section twice.
However, I would specifically like to know which Vitamin K supplement you would take if you were in my situation, and had to eat a very limited diet due to a jaw joint disorder, chronic facial pain and many food allergies/intolerances. I will be addressing these issues and getting treatment for them, but the treatment will be slow and the recovery journey will be long.
In the meantime, I have purchased the Life Extension Super K product because I get very little Vitamin K1 from my diet (approx 119mcg per day).
I’m currently taking 2 capsules per day of the Life Extension Super K. If I am unhappy with the results in 2 to 3 weeks, I am thinking of buying the Innovix Labs product and take 1 or 2 capsules of the Innovix labs per day, instead of the Life Extension Super K. Would you do the same thing as me? If not, what would you do instead and which Vitamin K supplement would you try next?
Thank you in advance,
Tom White.
brie cheese vs
jarlsberg cheese which has more mk4 k2 vs duck fat ?
The database is down and we’re trying to fix it. When it’s back up you can search the database.
Hi,
I have been on statins for over 20 years ever since my cholesterol was about 200 and my ratio was low . I exercise regularly, eat low-fat, nutritional foods. I did drink alcohol regularly until I quit 5 years ago. I never smoked. I had regular lifeline screenings that never showed any plaque build-up until some minimal build-up recently at the age of 60. I got tested and my calcium score is 800. My grandfather and father both clogged up and my grandfather passed from major heart attack at 60. I have seen 2 cardiologists and they have ran several tests which were all negative and their recommendation is to increase my statins from 10 mg to 40 mg daily. They say that the calcium has repaired and hardened coronary soft plaque deposits which is better than having soft plaque deposits that could break off. Also calcium scores are based on the fact that normal plaque is about 20% calcium and a person that takes statins has a higher percentage of calcium in their plaque which should mean that the calcium score of a statin user is effectively much lower than calculated. I started taking 2 daily doses of 50 ug of mk4.
The bottom line question that cardiologists do not want to entertain is can K2 usage actually soften my coronary hardened plaque deposits and turn them into a dangerous softer consistency and allow them to break off. I believe I have an inherited lipid disorder from my grandfather who probably died from soft plaque rupturing and giving him a heart attack.
Per Dr. Wm Castelli, of Framingham Heart Study, via Dr. Caldwell Esselstyn, of Cleveland Clinic: when the soft plaque begins to break up, the body pitches in some extra calcium to help stabilize it.
I got a score of 579 abt 3 years ago, and took up Dr. Esselstyn’s diet since he’s the only one with 100 percent results if you do his diet his way, not your version of his way. It isn’t easy but it does work. Even my ED has been breaking up and my doc has me on zero meds, he’s onboard since all the test results are better than any drugs he could use. Calcium hasn’t been shown to be a vitamin k2 problem, it may contribute, but just taking big doses of K2 hasn’t seemed to work all by itself. I am using the diet, exercise, Arginine-citrulline in 2:1 ratio about 5gr total twice a day, and nitrate/nitrite orally per the book “The Nitric Oxide Solution” by Dr. Nathan Bryan. There are good reasons for all of these things, I don’t F around, I want human interventional trials that worked on everyone to prevent-reverse heart attack, stroke, and death from heart disease. Period. Esselstyn has it, others don’t. It’s just a bit of a tough diet at first, then it’s not that hard as it seems. The arginine is based on Dr. Joe Prendergast who got great results on his diabetic patients, no admissions in 20 years, over 7000 patients. The nitrate/nitrite solution, well read the book. Good luck to you, keep your standards high about proof, and see these things I’ve mentioned. One more thing, I do take K2 in about 500u/day in MK7, plus 25mg/MK4 and K1 as well in one single pill a day from Koncentrated-K vitamins. It is very cost effective for the dose. Like I say, I doubt by itself it will do Jack, but more of K2 isn’t going to dislodge soft plaque, the body will not let that happen, so long as your diet doesn’t give the body the building blocks of plaque, like it is in your case, most probably. You’d have to see and become convinced of Esselstyn’s diet and the need for it, don’t pay too much heed to doctors telling you “you
‘re fine” etc. Pay attention to Esselstyn, and live. See the video: “Treating the Cause…Esselstyn” on youtube. It is 90 minutes long and tells the whole story. Best of luck. Bob
There are actually three problems here. One is if the plaque is calcified, two is if there is a soft blockage, and three is if the body is repairing the damage faster than it happens.
The calcification of the arteries is regarded by some experts as the most important and accurate indicator of a future heart condition. More calcification means more area of the arteries involved in artery disease. Medical opinions that calcium hardens plaque and makes it safe is a guess that runs counter to the statistics on calcification. The calcification is actually bone tissue growing in the arteries where it should not be.
The calcification can be reversed by adding a few nutrients. The MK4 form of vitamin K2 is specific to making the Matric GLA Proteins work to stop the calcification and reverse its formation. Its also advisable to take 10,000 IU of vitamin D3 daily as this boost the Matrix GLA protein that the MK4 works with. Including 20,000 IU of retinol vitamin A is also advisable as this helps in forming the proteins to do this. While you can try use of MK7 vitamin K2, its not normally present in the body and the body makes its own MK4 for this function when we are young and healthy. This rate of production drops off with age, thus the need for a supplement.
The soft deposits in the arteries are a separate problem. These are reversed by boosting arginine and citruline intake which enables the interior of the artery to protect its thin lining of cells. There is an old reference on how to do this in a book by Dr Louis Ignarro who discovered the function of nitric oxide in the body but newer references should be good. He included items like Alpha Lipoic Acid, CoEnzyme Q10, and natural vitamin E with the gamma form in it. I found that my blockages responded to 4-6 grams of arginine and this was separate from any calcification. I also found that adding the arginine took 25 points off my blood pressure, bringing it back to normal.
Thanks David, very interesting.
How do you know that your blockage was reduced? What tests have you had?
After being unable to get a diagnosis out of my PCP, I looked over everything on cardiac disease and the symptoms available in 2005. I was already taking many of the nutrients known helpful in heart disease. A book by Dr Louis Ignarro, No More Heart Disease suggested adding these and Arginine and Citruline. Within 20-30 minutes of taking 4 grams of arginine there was a measurable reduction in blood pressure. Since arginine is a component of connective tissue, over six months there was a reduction of 25 points in blood pressure to normal, probably due to larger arteries being formed. During this time my training speed in 6.5 mile runs went up by 8%.
One of the medical references had this report of a 2% death rate for patients treated with arginine. These patients were people with prior clotting events and arginine stimulates the immune system making immune generated clotting events more possible in simplistic or careless trials. I’d never had any clotting events so this was safe for me to try. Others have argued that this medical test was not valid due to the form of arginine used.
So no blockage measurements, but increased performance and a complete reduction of blood pressure from 145/80 to 122/70. The arginine also improved a number of minor foot tendon strains in a 53 year old male. I’ve repeatedly found over the years that lowering my arginine intake results in rising blood pressure.
Well done, David. I take arginine-citrulline in 2:1 by weight twice daily about 5gr each dose. Thousands of cases exist for the type of things we are seeing with it. Dr. Joe Prendergast has the proof in his endocrinology practice with diabetics in which their heart disease issues vanished over 20 years, over 7000 of them. Amazing. In my case, I also got a blood test for ADMA done by mail to a lab in Germany. ADMA is an arginine antagonist which competes against it for the enzyme eNOS. By upping blood arginine levels this can be overcome. Not all people have it but if you’re getting a big boost from arginine, it’s 90 percent likely you have high ADMA too. People with low ADMA don’t get as much benefit from arginine as those with high. High ADMA is often a death sentence unless arginine is used properly and continuously. It’s partly a genetic thing, I think. best, Bob
we are still waiting for any good human trials that show K2 reverses coronary calcium. Calcium is only 20 percent of plaque. If diet can remove soft plaque by 20 percent and calcium in the process grows 20 percent, due to the body throwing in some calcium for stability, I think you’re way ahead. No evidence yet shows that arginine-citrulline removes anything, though it may make blood flow better and arteries smoother due to nitric oxide. It may reduce the tendency for new plaque to form, but we don’t see that it will remove anything. Even the rat studies just showed nitrites in the drinking water only prevented, not reversed plaque in rats fed a highly atherogenic, high cholesterol diet.
Diet has shown the ability to reverse plaque, however, see Esselstyn’s photos of angiograms of plaque reversals in his patients. I’m not saying anything is impossible, just that we don’t have real evidence you can reverse plaques of any kind with just supplements while ignoring an atherogenic diet of cholesterol and saturated fat. Removing saturated fat and cholesterol and eating whole plant foods has shown that effect, without supplements, so it makes sense that be the cornerstone of any serious attempt at reversing heart disease, and probably essential to preventing its progress, with or without supplements.
How about individual results for grass fed and non grass fed dairy?
Whatever is in the literature, we put in the database.
In your review of K2 supplements you state, “While the label recommends a daily dose of 45 drops, this is based on studies using pharmacological doses to treat osteoporosis.”
My primary interest is in supplementing with K2 to treat osteoporosis and have read a couple of articles that recommend 45 mg of K2. There appears to be no clinical data on the effectiveness of doses between the 100-200 mcg for general health and the 45,000 mcg for osteoporosis (and no explanation as to why 45 mg is magic). And, although I believe that K1 is more specifically involved in blood clotting, I suspect that there could be some conversion of K2 to K1 which at osteoporosis treatment dose levels might not be negligible.
Chris, thank you for your research and for so generously making it and yourself available.
My question is specific to a supplement that I am considering taking for osteoporosis (as well as general heart/arterial health), rather than succumbing to the doc’s suggestions for injections of a now-popularly-pushed anti-osteoporosis pharmaceutical drug with possibilities of some serious side effects (no thank you!). The supplement I am considering is: 8X Strength Natural Vitamin K2 Formula. Provides 4-in-1 Support with MK-7, MK-4, K1 and D3 with Maximum Absorption for Stronger Bones and Cardiovascular Health 60 Capsules
by One Elevated. My concern is “should I be” 😉 concerned by the divulgence when one reads really thoroughly on Amazon’s descriptions, that it contains “trace amounts of lead”. I have always understood that lead is cumulative, can’t easily be chelated. The flip side of this is that there certainly is lead in our natural environment. Is it your opinion that one should be concerned by supplements that disclose “trace amounts” of lead, or, are they simply doing due diligence whereas, perhaps, other companies might not be so forthcoming in their disclosures and have “trace amounts of lead”, as well?
Thank you for your response.
Best regards — Suzanne-Marie
This might be related to California’s laws? I once went to a restaurant in a nice hotel in California where there was a sign saying “Warning: This restaurant uses ingredients known to the state of California to cause cancer.” I’d ask the company about it and see what it compares to for things you consume every day.
Thanks, Chris. That was my conjecture. I appreciate your suggestion; I’ll call company if I feel I need more info; thinking not! I’m “fine enough”, I’m sure.
good start: https://www.cinnamonvogue.com/Types_of_Cinnamon_1.html
Suggest you make sure you are ingesting Ceylon Cinnamon. Your liver will thank you and it may not be an issue with anticoagulants.
I am seeing sublingual K2 suplements . I like the idea, as I have absorption issues due to partial gastrectomy. I need to take K2 as part of my fight against osteoporosis. What is your opinion on getting proper absorption of K2 with a chewable, and/or sublingual supplement?
I haven’t studied, it, sorry. I will have to look into it.
Yesterday I saw a You Tube video [in French with English subtitles] that was a testimonial of a gentleman who had leukemia and was given months to live. Long story short, he began eating natto among other things and his leukemia eventually went away.
I’m wondering how much and how often eating natto would be suggested? He also too D3 which is something I would not do. Studiesseem to show that retinol would be just as effective along with magnesium which is required for the body to make its own D3. I take Rosita Extra Virgin cod liver oil which provides retinol and natural D. Seems to me natto is the best source for K2 as it also provides needed minerals.
Did I miss any mention of the powerful anticoagulant effects of Natto as in Nattokinase?
Hi Chris,
You said that your Thorne K2 drops last you three years; I have a bottle of the Thorne D & K2 drops that only had about a year shelf life. Is it safe to take after it’s expired?
Yeah I’m not sure. I’d ask the company. Next update I’ll revise the text to reflect the expiration date.
I’ve been taking D3, K2, zinc, boron and magnesium for one year. A year ago a Mayo Clinic surgeon said my CT showed the second most wide spread inflammation he’d have ever seen. My recent CT shows no inflammation. I use K-vitamins.com . I believe their K supplements give the best bang for the buck. It cost more but you get 25 times more K2-mk4 than the others. Can I have permission to copy your prints.
The supplement you mention being sold at http://www.k-vitamins.com only contains 1/2 milligram of MK-7. I dont see how that could help anybody who is trying to reap the Vit K2 benefit. It does have 25mg of MK-4.. maybe Im missing something here.
500 mcg is a lot. Read the section on how much we need.
Hi James.
What kind of inflammation are you talking about?
I don’t know what you mean by copy my prints. You mean print the article and distribute it? In what context, to whom, in what quantity, and how will you credit me?
Why do you think the rat and mouse research are 1:1 applicable to humans?
There is a lot of animal research where they found effect in animals, and in humans the same substance didn’t do anything.
I certainly don’t trust extrapolating Rodent research to humans; from what I’ve read, it’s used mainly for studying safety, toxicity, etc.
They are not reliable when it comes to benefits. For one thing, they aren’t fed diets too far removed from what they eat in the wild, like we are. Their bodies work in some ways the same but in others far differently from ours.
You have to estimate this on a case by case basis. Old evolutionary paths that are highly conserved are liable to have a common thread between rodents and humans. For example, the MK4 form of vitamin K2 is produced in both and its produced in all animals I’m aware of, even chickens and geese. When rat pups were given warfarin drugs from birth to prevent them from generating MK4, the rats died at around 2.5 months of age of calcified, burst arteries. Its known that warfarin has the same effect in humans of increasing calcification so the chemistry in both will be similar. So how MK4 is used for carboxylation and its need in any animal body is highly conserved, the animal doesn’t reach reproductive age if MK4 is missing or disturbed.
One example of a different chemistry is vitamin C. Most mammals make their own vitamin C internally in large quantities. Humans and Guinea Pigs survive without it by eating foods with vitamin C. Compared to this, not much MK4 vitamin K2 is available in foods and the internal transport systems that work with MK4 do not appear to work with the MK7 form, so we can’t adapt by eating the MK7 made by bacteria.
To me, the experiment where you study K2 vs calcification in rats on warfarin versus calcification in humans on warfarin should be compatible. Basic chemistry. But humans not on warfarin and on an atherogenic typical US diet vs rats on warfarin and on their typical chow would be a stretch. Too great a difference, even without the species issue. Yet that is often what is being done when hoping that ‘calcium is calcium’ and we should see improvement. The bodies would need to be matched up better with dietary challenges capable of spawning calcification in both species to tell if we can hope K2 will save lives from artery calcification from diet in humans; it would need to do exactly that in rodents with similar diets, and so far, that hasn’t been attempted to my knowledge. Anyone?
Glad to read such thorough coverage of an important nutritional topic.
One question came to mind given the warning about taking vitamin K while on Coumadin. I recently became aware of the coumarin content of some cinnamon. Would very much get your opinion about whether a warning should be extended to people not necessarily on prescription anticoagulants who consume cinnamon ?
Thank you for your writings
Good question, I’d have to look into it. Got a link to the research on it?
good start: https://www.cinnamonvogue.com/Types_of_Cinnamon_1.html
Suggest you make sure you are ingesting Ceylon Cinnamon. Your liver will thank you and it may not be an issue with anticoagulants.
Nice article! It is worthwhile reading this blog. Most of the people have not any kind of knowledge about K2 vitamin. K2 vitamin is also an important part for the body. Thank you for sharing this article.
I have a question about storage of my MK-4 supplement. I decided to buy the Thorne brand liquid K2 supplement (it is MK-4 suspended in MCT oil as a carrier). I am trying to simplify/minimize my daily routine because I don’t like having to rummage around and take several different pills or oils or supplements.
My thought is that since the Thorne product is so concentrated (1000ug per drop), could I just add it in to my bottle of Cod Liver Oil so I only have to take 1 supplement per day? Especially if I put the (already amber) bottle in a paper bag and keep it in the fridge, and shake it each time before using? Just take the number of servings per container and divide by 5, then add that many drops, right?
CLO is made up of approximately 1/4 PUFA (that’s the DHA/EPA), 1/4 saturated fatty acids, and 1/2 monounsaturated fatty acids, and most formulations also contain some tocopherols to promote stability. I would think a quality CLO would be a good carrier for this MK-4 supplement, but I wondered if anyone would be concerned about something in the CLO deactivating the K2?
I don’t think it will deactivate it, but you’d have to make sure it mixes properly.
Why not add the drops to your spoon first and then pour the CLO onto the spoon?
Thank you for your excellent information Chris. I have been reading your articles in Daily Lipid and the Price foundation for many years. My comments here are regarding the possibility of consuming too much K2. I am 75 year old female. I am in good health and take no medications and exercise daily. I do take some supplements in small quantities. Several years ago after becoming aware of vitamin K2 through reading Dr. William Davis’ site I started to make sure that I had K2 foods in my diet – mostly through pastured eggs and dairy (especially imported cheeses like Gouda and Jarlsberg , E. Swiss) and natto. I ate these foods every day and the cheeses in a large quantity. The natto I usually ate 1 of the 3+ oz cartons every other day. If I missed a day of natto I would take a Jarrow K2 7 capsule which has around 90 mcg or an Emu oil capsule. Last year I had surgery for a prolapsed bladder. The doctor told me that I did not bleed during surgery and asked me if I had any bleeding after surgery. I did not. He thought that was highly unusual. I did not discuss the issue with him. I was taking some supplements before surgery that actually could cause xs bleeding during surgery but I had stopped these about a week before the surgery. I was concerned about the lack of any bleeding from surgery and did a little research and did come up with a few articles that stated xs K2 can cause “hyper-coagulation” and hence possibly a stroke. I do not know if the information in the articles was valid but I decided that perhaps bleeding is a normal reaction to being cut during surgery and maybe I should cut back on the K2 just in case. So I cut down on the amount of cheese I was eating and eat natto every other day. I stopped taking K2 7 supplements altogether. I hope to have no more surgery to test the results of my cutback. I do bleed when I cut myself though.
Hmm, interesting, I too take K2 caps (mk7) and natto in green leaf shakes in a blender. Never thought it could affect my bleeding seems normal except I never bleed when I get a shot or blood draw. I tell them it’s because I’m too cheap. (old Jack Benny joke).
Hyper-coagulation fromcommon doses of vitamin K2 is a theory that is generally rejected by the results of MK4 and MK7 trials but the topic seems to have returned recently. In trials to identify this possibility, a group of patients were given 135 mg of MK4 daily for a few months and the result was no additional coagulation has occurred.
Here is a research reference:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5494092/
One with rabbits:
https://www.ncbi.nlm.nih.gov/pubmed/9414028
K2 cannot cause extra clotting. However, perhaps you have a clotting disorder and you had been K-deficient before, and now that you are not, you have too much clotting. You should have the doc check it out.
Your online article on Vitamin K2 is practically perfect. The graphics are well done and very helpful. You have answered all my questions, including ones I didn’t know I had. I have only recently learned of the importance of K2 for bone health. Since I don’t believe in calcium supplements and I am at higher risk for osteoporosis, this is important information. Eating lots of eggs, dark meat, and pork run counter to the dietary advice provided by most physicians to seniors. Looking forward to the medical community catching up (or breaking away from big pharma)
How can I get my sex drive back after taking insulin ejection 2 years???? Is it possible?
Chris (or anyone!),
Are you aware of any studies using K2 (with A, D3, magnesium) to treat heart valves? I have a congenital, bicuspid aortic valve and I would like to begin using K2 to assure that calcification does not harm its function.
Has anyone with this condition been using K2 (with A, D3, magnesium) successfully to stop valve stenosis / calcification and even reverse it? Which forms of K2: MK4, MK7 or both? Dosages?
What tests do I need to take to determine the function of this valve and to determine if calcification is, indeed, an issue?
Is there a cardiologist on the web who posts updates about K2 research?
Note: Everything I have read discusses the absolute vital importance of magnesium for heart / cardiovascular health. I am purchasing Dr. Carolyn Dean’s (see her mg book) ReMag and also using Ancient Minerals’ transdermal magnesium (see Dr. Sircus’s book).
I have been told if you have to go to the ER for a heart issue (stroke, heart attack, etc.), immediately take magnesium and / or spray it all over your body, and ask that the ER immediately give you IV magnesium, before any other treatment is begun.
William Davis is a cardiologist who has blogged a bit about K2. I’m not familiar with heart valve research.
I searched Dr. Davis and found this quote “Vitamin K2 is indeed worth considering, but you should know about the issue of bowel flora and K2 for future reference.” As usual my next rabbit hole was to search – gut flora and vit K2 issues which landed me here –
http://www.meschinohealth.com/blog/just-in/2012/05/24/vitamin-k2-heart-disease-gut-microflora-produce/
Dr. Meschino states that so much K2 is made in the gut that supplementation may result in overdose of K2 that “can make blood clotting too aggressive, forming abnormal clots that can lead to sudden death from a heart attack, stroke or lung embolism.”
So, my burning question is…. have you ever found this metabolic situation supported in you study of Vit K2?
You can safely discard these two opinions about vitamin K2.
Find sources that consider the MK4 and MK7 forms separately in research and in the body. The MK7 form is made by bacteria and doesn’t get around easily in the body evidenced by the 3.5 day half life and higher side effects in those sensitive to MK7. There are no records of clotting events I know of from research or medical reports, otherwise eating natto would be known to be dangerous.
The MK4 form is that which is made by the body for carboxylation of MGP and Calcitonin, vital proteins to reversing artery calcification and maintaining bone health. The MK4 is made in a bio identical form by a factory but is normal to the body and well controlled by the body. In research trials, doses of up to 135 mg per day have been tried with no ill effects. MK4 has been an adjunct to treating heart disease and bone loss since 1995 in Japan. The MK4 works outside the liver in the body so it only has a small effect on blood clotting as compared to vitamin K which is central to blood clotting factors. Adding more vitamin K does not increase blood clotting in healthy people who are not on warfarin drugs.
Reliable reporting is available in Life Extension magazine articles on vitamin K2 and referenced NBI research articles. Both Companies sell MK4 and MK7 vitamin K2 products.
Dear Chris, Dwight and Dave,
Thanks for the info! I really appreciate the cutting edge help re. heart valves and K2!
I have also noted inconsistencies on the web re. K2 MK4 and MK7 and given that I need to keep a heart valve happy, I cannot afford mistakes. Do I need MK4, MK7, or both, and how much is therapeutic?
Since I ferment foods, I looked into fermenting as a good, reliable source of daily K2.
Dave, I read an earlier comment of yours, below, re. Dr. Mercola and Vitamin K2; you stated he – incorrectly – utilized K2 MK4 research to validate buying his K2 MK7 supplement products.
I actually looked into buying the bacteria/fermentation product Dr. Mercola sells, with which you can ferment vegetables and create, supposedly, a fermented food product with a lot of K2 (menaquinone: see https://www.probioticscenter.org/dr-mercola-kinetic-culture/).
Kinetic Culture PR states: ” Vitamin K2 is naturally produced by the fermentation process, and certain probiotic strains can produce more K2 than others. Kinetic Culture was created specifically to produce ample amounts of K2.” (See: https://www.mercola.com/pressroom/march-2014/mercola-com-releases-kinetic-culture.htm)
(Note the PR does not disclose which type of K2 the product produces.)
The bacteria he sells are mostly Lactobacillus, with a few Bifidos added in and it is EXTREMELY, outrageously expensive. Furthermore, natto (fermented soybeans, which is the highest fermented food source of K2 MK7, I believe) uses B. subtillus bacteria to ferment. Mercola’s product contains NO B. subtillus.
Here is the list of bacteria in his product:
Lactobacillus acidophilus DDS-1
Bifidobacterium Lactis
Lactobacillus plantarum
Lactobacillus rhamnosus
Lactobacillus casei
Bifidobacterium bifidum
Lactobacillus brevis
Bifidobacterium longum
Streptococcus thermophilus
Lactobacillus salivarius
Note the absence of B. subtillus. Actually, I don’t think B. subtillus would work upon vegetables, it works upon beans: hence natto (fermented soybeans) as a high source of K2 MK7.
Therefore, I don’t understand how this fermented product is producing a large amount of K2 MK7. Sauerkraut, according to food lists, is a very poor source of K2 MK7; how can this Mercola ferment product be any better than plain old fermented cabbage and salt?
I believe Chris stated in his article that he contacted Dr. Mercola to find out how much K2 MK7 his bacteria product produces and he had not yet heard back.
And, this product, if it is producing ANY K2, would be producing K2 MK7 (sourced from fermentation), not K2 MK4 (sourced from animal products).
I, therefore, decided NOT to buy this bacteria product and will, instead ferment my own black beans (soybeans are too risky as re. to GMO and Round-Up contamination) using B. subtillus from Cultures for Health for a mere $5.95, which will last for months of fermenting beans! (see: https://www.culturesforhealth.com/mitoku-traditional-natto-spores.html)
However, I am still left with the issue that this homemade fermented food is producing K2 MK7 not K2 MK4.
Is it, in fact, K2 MK4 which I need to take to keep heart valves / arteries free of calcium?
One factoid which I throw out there is that this Mercola bacteria mix MAY produce a lot of K2 MK7 (we need verification of that fact from Mercola with stats/data), but its potency may degrade rapidly, once the product is exposed to air.
I know this because I have followed the sinusitis story over at lactobacto.com (it is an amazing story, go read it if you suffer with sinusitis and go buy kimchi or the brand new L. sakei probiotic pill) and those people who use the juice from Kimchi to repopulate their nasal biome have found that the Kimchi bacteria which balances the biome (L. sakei) loses potency – after opening the jar – in about 7 – 10 or so days.
So, we need to know if this fact is true about Mercola’s – or anybody’s – fermentation bacteria product, with, alleged, high levels of K2 MK7: that is, is potency lost after 7 -10 or so days’ exposure to oxygen?
BTW, it is at that website – lactobacto.com – that I discovered that it is likely the garlic in the kimchi which produces the L. sakei bacteria which re-balances the nasal biome, so I am going to ferment just plain old garlic and take one every morning.
Dr. Kate Rhéaume-Bleue, ND, who wrote the book Vitamin K2 and the Calcium Paradox: How a Little-Known Vitamin Could Save Your Life, wrote about using K2 MK4 vs. K2 MK7 for healing rheumatoid arthritis, in her article, Choosing the Right Vitamin K2: Menaquinone-4 vs Menaquinone-7
Clinical considerations of different forms of vitamin K2 (see: https://www.naturalmedicinejournal.com/journal/2015-10/choosing-right-vitamin-k2-menaquinone-4-vs-menaquinone-7).
I, too, am going down the rabbit hole – in my case re. de-calcifying heart valves – and this K2 article by Chris Maseterjohn is an INVALUABLE tool for me! Thank you Chris. You are helping so many of us get and stay healthy with (and despite, in many cases) the advice of our medical doctors.
Newsflash: Vitamin K REGULATES clotting, it doesn’t cause clotting.
MK-7 is THE form that is most effective, not the overhyped K2-K4.
“Later studies, in which the long-chain menaquinone-7 (MK-7) was used to counteract warfarin-induced calcification, showed that this form of menaquinone was even more potent than menaquinone-4. ”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3648717/
Laura, you often see that comment “you don’t have to take K2 because bacteria in your gut make plenty”. The problem is that the K2 is bound up inside the cell of the bacteria and is not available to us. Mercola has an interview with Cees Vermeer who is a member of the Rotterdam Group research team that have done a lot of research on K2. Mercola asks about absorbing K2 from your gut bacteria and Cees replies “only if you’re prepared to eat your own feces like rats do”! (See, easy and doesn’t cost anything 😁) He goes on to make the point about the K2 being bound up in the bacteria cell and also points out that the K2 bacteria are too low down in the gut for absorption to take place anyway.
The Rotterdam Group have done experiments inducing arterial calcification in rats by giving them warfarin and then reversed it with K2-MK7. The calcification is because the warfarin (aka Heparin or Coumadin) prevents the K1>K2 conversion. They also showed that by giving K2 with the warfarin they could prevent the calcification in the first place. (search PubMed for the papers) If you are taking warfarin/Coumadin you might want to do this but I would take MK-4 (doesn’t convert to K1 per Chris above) and adjust the warfarin dosage to get acceptable INR.
A lot of people (including Cees) recommend MK-7 instead of MK-4 because of its longer persistence in the blood. But as Chris points out that’s because the body prefers MK-4 so it’s rapidly absorbed. I take both.
I take both,too, but I doubt either is going to fix a calcification problem that stems from acidosis, or soft plaques that attract calcium, all by K2 alone. If the body is using calcium from bones to neutralize acid from too high protein in diet, or to stabilize dangerous plaques, the body is complicit in the calcium deposits out of self-preservation. A low acid-forming diet, a low plaque-forming diet, plus K2? maybe. maybe. But alone with just vitamin D3 or other tweaks against the tidal wave of the other factors, I tend to doubt it.
Prolia was not mentioned. Every 6 months syringe of 60mg.
I do take. K-7
Have critical osteoporosis
Does one fight or enhance each other?
Thank you. Marge Lyons
Natural Vitamin K2-7 is very important for healthy life e.g. Bone, Dianetes and Muscle health etc.
MenaquinGold is the most researched natural vitamin k2.
This is properly explained in this page.
https://www.synergialifesciences.com/natural-vitamin-k2-menaquingold.html
GreatDanes –
Cyclodextrin may cause permanent hearing loss.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5676048/
You should not concern yourself with the calcium that you already have in your arteries. You are asymptotic; It’s not a problem.
Plaque is caused by oxidized LDL and endothelial inflammation. Eliminate either one of those and you cannot form plaque.
You need to get back on your statin. As I recall you had an LDL 500 Ca score may just as well have been from 20 years ago before you were on statins.
You need to focus on your inflammation. Your HsCRP is still too high and may well be indicative of inflammation of your endothelium. Pauling therapy may help. Plant based diets will usually work well. Testing for Homocysteine is more specific to blood vessel inflammation and costs about the same as HsCRP.
I would not be trying to remove any Ca until you get your LDL under 60 and your CRP under 1.
Best of luck!
ChetT – My original LDL score from March of 2016 was 50. At that time I was onw of the longest people in the world on statins – my doctor in Phoenix Az back in 1979 to early 1980’s, got me into a trial (and then a followup trial for many years – if I remember that went from around ’82 or ’83 to ’87 some time) and a pharmaceutical product that eventually was approved called Mevacor. I had been on increasing doses of statins since then until I stopped in 2016. I stopped because I still got a calcium score of 299 with an LDL reading of only 58.
My Homocysteine is consistantly around 9 for many years.
Oxidized LDL seems not to be a problem because my last Myeloperoxidase score last month was a good 282 with an LDL particle number of 626 and a LDL particle size of 21. Small LDL P was <90 and APO B was 95 (I would like to get that down to 80, but 95 may be OK).
Insulin good at 3.2 and hbA1C good at 5.1 – normal values on a plant based diet (but the Homocysteine of 9 is a bit of a puzzle?)
My GP can't figure the bad CRP and neither have 2 (mostly useless) cardiologists.
Yet still the calcium score rose to 452.
The paper you referenced was mostly base on HPβCD. theHPαCD doesn't seem as bad.
Heart Disease
maintain flexibility and integrity of the intima.
Magnesium supplements
Vitamin K2 activates Matrix GLA protein
Vitamin D3 stimulates production of Matrix GLA Protein 6x
Vitamin A required for D3 activity
DHA vitamin lipids maintain membrane flexibility
curb systemic inflammation
niacin reduces the LDL capable of passing through cracks in the intima and accumulating as plaque in the intermedia.
——–
The porous interstitium behind the arterial intima accumulates Low Density Lipoproteins through breaches in the intima. The intima loses elasticity, and structural integrity for lack of magnesium counter ions, Matrix GLA Protein for Ca removal, and fluid continuity induced by docosahexaenoic acid. The mechanism for repair of atherosclerosis follows the cause.
maintain fluid integrity of the intima, lining of blood vessels.
Magnesium supplements, the proper flexible counter ion for cell membranes
Vitamin K2 activates Matrix GLA protein that removes improper Ca counter ions
Vitamin D3 stimulates 6x production of Matrix GLA Protein (10,000 IU)
Vitamin A required for D3 activity (10,000 IU)
DHA fish vitamin lipids maintain membrane flexibility
Chelates help remove calcium (Vitamin C, alpha lipoic acid, citrate)
curb systemic inflammation (tumorecht)
niacin reduces blood titer of LDL capable of passing through cracks in the intima and accumulating as plaque in the intermedia.
Elevated blood homocysteine signals an impaired methyl transfer pathway. Methyl groups are essential for producing choline for cell membrane structural integrity, DNA regulation, and brain memory neurotransmitters.
Methyl transfer pathways depend upon a combination of essential vitamins: B6, B12, folic acid, and a source of methyl groups. Meat is a good source of methyl groups. Otherwise think lecithin, and arginine.
It took you 68 years to build up a Ca score of 299. Then you stopped the Crestor and went from 299 to 452 over the last 2 years. That’s about a 25% increase per year. I gotta wonder just how high that number would have been had you not been on statins for most of your life.
Switching to the Mediterranean diet did seem to do you some good in lowering your CRP but your LDL is now at 99. I really believe that you need to get back on your statins.
It looks like you have had expanded cholesterol tests. I’m curious, what are your HDL particle counts? With all this “good” cholesterol you gotta wonder why there is little reverse cholesterol transport (RCT). Do you supplement with omega3? Do you know if you carry the ApoE4 gene variant?
Hi ChetT – my ApoE4 score is double E3 which is standard risk.
I do use Innovix Triple Strength fish oil every day, and eat at least 3 fish meals per week.
My HDL-P is consistently around 40 on the NMR scale, so it would be much higher on the CIM scale but I don’t have that scale available here. On NMR > 30 or 31 is standard risk and > 34.9 is very low risk .
Also on the NMR scale my LP-IR score is <25 which is very low risk and that brings me to the crux of the statin problem.
In 2015 the American College of Cardiology finally released their report (after sitting on it for well over a year) "Statin Intolerance: Not a Myth".
In this report on strongly under reported side effects from intensive dose statins they finally admitted that one (among many side effects in the report) they found "risk of new onset diabetes (NOD) (9-27%),
Intensive-dose statin therapy is associated with a 12% higher incidence of NOD compared with moderate-dose statin therapy".
So, to get back to the statins, my IR and glucose/A1C readings were bad on statins at effective doses. Low dose statins did almost nothing for me and high dose statins were puttin me pre-diabetic, which was a common problem in the report.
Stop statins and my IR clears but cholesterol goes up. Continue statins and new onset diabetes train was in the tunnel – so stopped statins and IR A1C are all good now.
So pick my poison – low cholesterol or bad IR? Not a great choice.
Greatdanes-
My advice is don’t worry about the cholesterol levels. Be concerned about the long-term damage that might have accrued due to statins and do everything you can to support your health, rather than poison it.
Many studies have shown that statins don’t reduce the progression of calcium scores. While statins might reduce inflammation, you’re better off doing so by discovering the source of the inflammation and eliminating it. Ask the hard questions: where would I be harboring sub-clinical infections?
I for one would be wondering whether I had an low grade infection in the heart vessels and looking into studies that show anti-microbials success in reducing the progression of heart calcium. eg., using aged garlic extracts or allicin. I would also be asking whether my dental health is somehow involved, eg., do I have root canals that might be infected and in need of removal? (Really big question and potentially very expensive as most root canals show no signs of overt infection
Your genetics might necessitate a higher need for ascorbates. The high HDL might indicate a higher blood lp(a) level than normal (did your blood tests include testing lp(a) ? ) , and that is again genetically determined. The theory that by increasing the serum ascorbate level will reduce the lp(a) level is worth reviewing. Again, if there are sub-clinical infections untreated, any ascorbate you get via diet and supplementation must be great enough to deal with those as well as countering any genetically determined levels of lp(a).
The use of lycine and proline in the Pauling/Rath treatment will also somewhat inhibit the ability of lp(a) to “stick” to the problematic blood vessels.
https://www.scirp.org/journal/PaperInformation.aspx?PaperID=72016
At least one source suggests removing gluten food products from the diet will also assist in halting the progression of calcium although I don’t know the nature of the studies done
(same source for aged garlic references):
https://jeffreydachmd.com/2015/06/coronary-calcium-score-benefits-of-aged-garlic/
Alan – I have started the Rath/Pauling Protocol and hope to be at recommended dose by next week, I am increasing the C a bit each day since C added quickly can have gastric side effects.
As previously noted my Myeloperoxidase score last month was a good 282. MPO is an indicator of oxLDL activitity.
I have scheduled full dental x-ray’s for next month so that will be checked as recommended.
Regrettably did not do lpa(a) yet so that will be corrected soon however Apo B was pretty good at 95. Gluten has been gone for 2 years now – I don’t touch it.
A low grade infection in the heart vessels is a real possibility – the CRP is coming from somewhere. There is also some probability that BPH/LUTS is the source of some CRP problems in my case. The other strong possibility is inflammation discovered during 2 endoscopic procedures. Gastro specialists recommended long treatments with PPI’s – been there and done that for ulcers and probably had leaky gut from PPI’s for many years, so I avoid them now. These are some sub-clinical infections areas to be looked at, however I try to avoid antibiotics unless I have a extreme emergency – so I will look at natural anti-microbial treatments now.
GreatDanes,
Well if you can no longer take a statin to lower your LDL then I guess your left with focusing on the health of your arteries. The Pauling protocol reads well and has a lot of anecdotal support. It should help but who knows. That anti-inflammatory protocol by Dr. Kaufmann might be another thing to consider. It seems I’ve been doing a variation of this for some time now.
Hey if you’ve got 10 grand to spend you might want to take yourself to the ILC clinic in Hungary for 6 weeks and get the cholesterol immunization they’ve been selling for a decade now.
http://www.ilchungary.com/treatments/cholesterol-immunization/
I found it very interesting but could never verify any of their claims.
Best of luck
My recommendation to look into your dental health for low grade infections is based on very controversial ideas about root canals and so called cavitations: areas of infection left behind to fester in the jaw after the bone/gums have healed. If you’ve had ANY root canals or ANY extractions, there are dentists that believe that those are areas of possible long-term low grade infections (and that the toxins produced in those infections are very strong, if only in small amounts produced and seeping into the bloodstream). (Implants are more likely to represent areas of inflammation due to a body reaction to an incompatible metal, eg. titanium.) Any mercury/silver amalgams in your teeth also might contribute to inflammation elsewhere in the body if you have a strong reaction to the metal.
The more obvious type of dental infection would come from gingivitis and periodontal disease; some dentists will determine the nature of the organisms in your dental plaque to see if they are esp. virulent. We’ve all heard about these organisms ability to further infect heart tissue, esp. valves. I know someone who had a severe backpain, that turned out to be an infection in his spine and the doctors were amazed that the infectious organisms found were dental in origin; this same person shortly afterwards had heart valve surgery (and possible never connected the dots about the possible relationship to the dental infections). These types of infection should be relatively easy to treat.
The problem with root canals and cavitations is that it can be near impossible ( x-rays won’t help much at all unless the root canal tip is obviously infected, in which case you’d probably have symptoms already) without more surgery to determine if an area is infected, ie., the need to remove the root canal(s) and/or an exploratory dig into long sealed over extraction sites. Some dentist believe that all root canals are problematic and advise extraction. There was a device developed to determine if cavitations existed, but I don’t believe it got much usage.
So, if you’ve had no extractions (eg. long ago removed wisdom teeth) and you’ve had no root canals, and your gums have been in good condition, I wouldn’t worry too much about dental related inflammations.
Considering that you’ve had ulcers and assumedly treated the ulcers with antibiotics (or perhaps mastic gum) while you were using the PPI’s, and assumedly you’ve tested negative for h. pylori since, then given that you believe you’ve had leaky gut going on, it would seem beneficial to continue to work on healing that as you’ve indicated. Again, if you have any mercury in your teeth, it could be contributing to problems in your digestive track, such as leaky gut.
For me, it’s most important to realize that many factors can increase the need for extra vitamin C (and other complimentary nutrients). Excessive exercising will definitely increase the need. Negative stressors in general will put an increased demand on the adrenal glands which then need more continual and consistent support.
You may want to change your opinion in mk4 vs mk7 in terms of coronary artery calcification. This studyhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC4866409
found one YEAR worth of mk4 supplementation did NOT reverse CAC, in fact CAC got worse in the mk4!
https://www.ncbi.nlm.nih.gov/pmc/articles/
Also this study found blood levels of vitamin k did NOT INCREASE above baseline whatsoever in a mk4 supplemented group compared to significant increases up to 48 hours in the mk7 group. youhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC3502319/
You may need to rethink the effectiveness of mk4.
Not surprising. It seems to me that coronary artery calcium isn’t the result of a simple vitamin deficiency. And it won’t be reversed or stopped by supplying the vitamin. The body is responding to the atherosclerosis by throwing in calcium to stabilize things, not mistakenly adding calcium where it does not belong.
Plaque volume is about 20-25 percent calcium. What I’ve read shows that it forms when smooth muscle cells migrate into the sub-endothelium and change their phenotype, forming a matrix for calcium to attach onto.
To stop them from this migrating, it’s necessary to introduce nitric oxide. If the endothelium is damaged it can’t make nitric oxide so the process continues. Dietary changes, including introduction of nitrates and nitrites from beets and greens, L-cittruline, and natural whole food antioxidants can boost nitric oxide and may help to halt this process. If you are not willing to give up things in the diet that cause the disease, don’t bet on a vitamin to go up against them. I use Dr. Esselstyn’s diet along with nitric oxide management and test strips by Berkeley to find my nitric oxide levels. I got a bad calcium score of 579 two years ago, and have not gone back to find out how much higher it went. I’m more concerned about the softer plaques rupturing, and reducing those. In the 2 years, my erectile dysfunction has been reversing without any drugs, so that is good news. Even if I stop the nitric oxide supplements, the ED stays fixed on this diet. I’m 72
Personally I have found taking 1.3 mg of MK4 daily to be very effective at reducing artery calcification over 12-18 months when there was nothing else that would affect the condition symptoms over 20 years.
Its been verified in research that the MK4 vitamin K2 is what the animal or human body makes for its own carboxylation purposes. Totally subtracting MK7 and MK4 from the diet does not produce recognizable K2 deficiency in young animals as the MK4 produced within the body answers this need. The production of MK4 can be stopped by applying warfarin drugs to the cohort and this immediately produces severe artery calcification and early death in animal trials.
I don’t know why this trial didn’t work to produce better results. One item is that if vitamin D levels are low, little of the Matrix GLA Protein is produced and since this protein actually does the calcium control when carboxylated, a low or very low Matrix GLA could produce null results in calcium scavenging actions. There are numerous successful trials with MK4 vitamin K2 that cannot be discounted due to a single null result.
I had and probably still do have, real bad calcification, 579 calcium score, and absolutely no symptoms from it. I was amazed to find out via the scan.
I don’t know how you can know what is going on with coronary calcium from symptoms alone. If that were possible, the disease wouldn’t be known as the stealth disease, and the scan would not have saved so many lives by alerting us to who is really at risk. I’m glad your symptoms have improved and hope that continues for you, of course.
I’d say that Angina is a very unstealthy symptom of a constricted coronary artery and you’ll find a lot of anecdotal testimony about how taking this or that supplement or some other lifestyle change will have a significant effect on the symptoms.
I see that you have chosen what I would call an extreme lifestyle change with your plant based diet. That may be a great choice but until you get another scan we won’t really know if it’s had any measurable effect but you do have some good studies on your side.
I chose to make some sensible dietary changes and use supplements and my read of the science to offset the negative effects my fuel and lifestyle might cause. I’ll get another scan and tests to monitor my success or failure.
I’ve commented before but will say again, the calcium score rarely if ever lowers, even if total plaque volume declines. Plaque reduction destabilizes it and the body throws in more calcium to help out. Don’t be disheartened if your score goes up again. It is only 20 percent or so of total plaque volume, you want the rest of the plaque to go down to get the greatest benefit percentagewise from your efforts. I have little doubt my diet, which is only extreme in western civilization, but not in places where it is natural and they do not have heart disease. I’m used to it now, and your diet would seem extreme to me, I’d bet! 🙂 Best of luck, and good going on fighting back.
Thanks, Chet. I had so much fear I did take extreme measures, however, I believe the diet isn’t that extreme except in the US and others. In a large part of the world population it is very normal and they’ve got close to zero artery disease per studies. It’s a couple billion people doing this. I considered moderation but with my former big meat diet, I chose to compensate, not moderate, so as to drag my lifetime average to moderate. Most people consider what I do extreme, however. I tell them I eat what everyone else does, just different quantities, and zero is a quantity. 😉
Regarding these ncbi studies, no one has mentioned a critical detail: that the participants took 45 mg of mk-4 per day. Although I have long been a bit skeptical regarding these reversal of calcification in the arteries claims myself, the skepticism goes both ways. Yes, I know that that is the dosage used in studies in Japan to reduce bone loss (NOT intended for reducing CAC), but for a person to take that much per day for long periods of time is a dubious course of action. First of all, no group of people throughout history could ever have eaten anywhere near that much mk-4 as part of a natural diet. Furthermore, as Chris has stated, it is actually the mk-7 that seems to more effectively aid the bones, such that one can get impressive results with pedestrian-level intakes such as 100 mcg. per day. Trying to improve your bones (or reverse CAC, for that matter) with massive doses of mk-4 may be a lot like trying to get your daily requirement of potassium by eating snack foods — it may be possible, but there are far better ways to do it, and you may be also doing yourself some damage in the process.
What I’m leading to is that it does not necessarily follow that just because taking vast amounts of K2 mk-4 has not been shown to “reduce CAC or arterial stiffness,” that this then must logically infer that taking far lesser amounts will be just as ineffective — crazy as it might at first sound. After all, many people get too little vitamin A, for which the RDA is currently set at about 5,000 IU’s. Does this mean that getting 50,000 IU’s of it daily will be even better?
There seems to be controversy as to whether D3 and K2 should be taken together or separately. Some nutritionists recommend taking D3 in the morning and K2 in the afternoon or evening for greater absorption. I take fish oil at both times. What is your view? Also, I take two Calcium/Magnesium/D3 supplements (Kirkland/Costco) totaling 500mg calcium citrate each day, once morning, once evening. I’m thinking I have serious calcium buildup. Should I cut back? (I also take Magnesium 400mg at a different time.) I am working hard to eat more nuts, dairy, salmon and fresh vegetables.
I don’t think it matters if you take them together or separately.
This is a documentation of one person’s experience with calcium scoring and attempted treatments. None of my degrees are in a medical field and I can not give medical advice, and I am not making any medical recommendations in this post – simply stating what my calcium problems and attempts to treat myself through my own research.
March 2016: Age 68 yo. Weight 192 lbs.
First ever calcium score.
Total 299 (Right Corn. 127, Left Ant. 172)
Meds. 40Mg Crestor and 10 mg. Lisinipril.
BP 122/82 Chols. Tot. 165, LDL 58, HDL 93 TG 69
The Calcium score caught me by surprise at 299 so, in my individual case, a high dose of statins did not prevent calcification. I Have no idea if statins might help others?
So, time to research.
Started taking MK4 at 5mg 2X day. MK7 at 180 mcg. 2X day. Vit A at 5000 iu. 2X day and Vit. D at 5000 iu also 2X day.
At least 1.5 hours exercise per day 5X week – heavy on aerobics.
Plus a Mediterranean type diet heavy plants, but mostly grain free.
Fast forward to Sept. 2018: Age 71yo. Weight 150 lbs.
Calcium score of 452 (Right Corn. 217, Left Ant. 235)
BP 109/70 NO MEDS anymore.
Chols. Tot. 217, LDL 99, HDL 99 TG 93 NO MEDS anymore.
So I am much worse on calcium but better on most other measures.
And I don’t understand what went wrong with continued calcium buildup – or maybe ‘capping’ is what increased the calcium score?
Changes since the bad Sept 2018 reading:
Modifying my diet away from Mediterranean toward primal/keto (see Mark Sissions book if interested).
Changing exercise to much more weights and much less aerobics. All the aerobics appeared not to help me.
Currently investigating the use of meds/supplements:
dasatinib, metformin, and rapamycin and cyclodextrin.
I have e-mailed with Dr. Alan Green and he believes that the combo of staggered, low dose rapamycin may cap soft plaques when combined with daily metformin.
Also now investigating Dr. Sandra Kaufmann’s protocols but haven’t made decisions on anything except diet/exercises.
AGAIN – my personal experiences here – there is no medical advice or medical recommendations.
Thank you for your detailed documentation. I can profit from your experience.
Your calcium score result is perplexing. I suggest you add a magnesium supplement to your diet. Magnesium is the intended counter ion for all cell membrane phospholipids. In the absence of adequate magnesium calcium substitutes because of its similarity on the periodic table. Unfortunately calcium does not confer the fluid property of magnesium. The least expensive source of magnesium is milk of magnesia diluted into lemon juice, and diluted again into drinking water.
Hi Keith – magnesium (mostly citrate) has been at least 600 mg per day with most days at 800-1000 for many years. I also take high quality fish oil, B vits (pre-methylated) and a very complicated multi vit schedule.
On a plant based diet some of the things that happened was my iron/ferritin levels plummeted to anemia levels and my TSH went from 2.5 to 4.05. These values are recovering now. TSH back to 1.97 this week and iron/ferritin just above the anemic range and seem to be improving.
Back on grass fed meat/dairy and more salmon meals for almost 3 months now.
One possible conclusion to me (and there is much research on this) is that not all diets work for all people and a plant diet was not correct for me – seemed worth trying at the time. Plant diets work well for some people and for those lucky ones I an happy they found a solution.
Notice the significantly high HDL in both of your shown labs. Has this been explored, eg. have you been taking high dose niacin? For men with HDL’s in the 90’s there might be a genetic cause for CVD:
https://www.medicalnewstoday.com/articles/319275.php
GreatDane,
Vitamin K2 is not the whole story, nor the complete answer to age related maladies. You may ponder my recent observations:
mitochondria
I’ve been reading and wrestling with potential cures for my age onset asthma. Slowly my thoughts consolidated on the loss of mitochondrial ATP energy supply as the foundation cause of aging also called senescence. I found several good reviews on the subject. The masters of the universe have come to the same conclusion. I am a few years late to the party.
Fortunately there are seven interventions to restore mitochondrial ATP production.
1. maximum stress on the quadriceps stimulates the healthy mitochondria to divide. This replaces damaged mitochondria. Think leg press machine and squats.
2. Taurine is a conditional vitamin necessary for the first steps in oxidative phosphorylation. Plenty = 1gm/100gm is available in fatty fish, shellfish, and egg yolks. Well cooked meats lose their taurine. Veggies have none.
3. alpha lipoic acid is necessary for the second two steps in oxidative phosphorylation. 600mg supplements are adequate. This one declines with age but I have read no data.
4. L-carnitine is necessary for transport of fats into mitochondria for oxidation fuel. Diversion of fats away from storage and toward ATP production aids in weight loss. 1-2 grams per day supplements are adequate. Body builders swear by it for removing fat between skin and muscle. I notice more energy climbing a 30% uphill grade after four days at 1.5gm/day. I am hopeful for a gut fat reduction effect. Half time in blood is 2.5 days so it builds to max blood titer in fifteen days. Acetyl-L-carnitine rapidly (hours) crosses the blood brain barrier and contributes to positive mood and synthesis of acetyl choline necessary for memory. L-carnitine apparently does not cross the blood brain barrier.
5. ubiquinol peaks at age 20-25 at 500 mg/day. Synthesis declines by half every twenty years. I take 400 mg/day. Required for the last four stages of ATP production. Said to be highly synergistic with alpha lipoic acid.
6. Vitamin K2 substitutes or contributes to ubiquinol function and low level 360 microgram/day supplements add 15% to respiratory capacity of young trained athletes. Perhaps more is better. No known toxicity to 45 milligrams/day.
7. Zinc. 22 milligrams/day seems minimum daily requirement. Up to 100 mg/day for a few days are tolerated. 300 mg/day is toxic and inhibits ATP production. Zinc deficiency causes benign prostate hypertrophy and difficulty urinating. Men have a built in signal for zinc deficiency that can be cured in two days of 50mg/day. Zinc is necessary for countless enzyme systems including the mitochondria ATP systems.
Low ATP leads to failure of cell repair and failure of apoptosis (suicide of old sick cells). Bad cells are not cleared but become necrotic. Stimulation of inflammatory interleucin peptide hormones results and leads to inflammatory diseases such as asthma, arthritis, eczema, psoriasis, Crone’s, periodontal disease….
Keith
https://link.springer.com/content/pdf/10.1007/s001250051536.pdf
https://news.harvard.edu/gazette/story/2017/03/harvard-scientists-pinpoint-critical-step-in-dna-repair-cellular-aging/
http://www.resveratrolnews.com/history-of-nicotinamide-and-aging/868/
After two to three months I notice general health improvements:
1. Severe asthma cured
2. Blue color vision is more intense.
3. Dreams are in vivid colors
4. Recurring ear canal infection cured, hearing recovered.
5. Blood pressure normal with medication and near normal without.
6. Positive mood and great tolerance to situation stress.
7. More resistant to itchy fungal skin infections, a hyperthyroid risk.
8. Exercise is aerobic without lactic acid soreness. Increased strength.
9. I move more quickly with a bounce in my step…I am stressing my arches.
10. Less appetite …Lost ten pounds of fat effortlessly.
11. Better memory and focus on academic texts.
12. Better balance when donning undershorts in the morning.
13. I am motivated to begin and complete projects.
14. Deeper sleep and more sleep. Repairs are underway.
15. Benign prostate hyperplasia cured without the aid of Zinc.
16. All the women look pretty.
Therapy per day:
1 gram L-carnitine
1 gram acetyl-L-carnitine
1 gram nicotinamide
600 mg alpha-lipoic acid
400 mg ubiquinol
homemade fermented vitamin K2 liver pate
frequent omega-3 foods
5,000 IU Vitamin D3
frequent vitamin A foods
50 milligrams DHEA
25 milligrams pregnenolone
———————————————
Millions of experiments support the following model of old age remediation:
Age is caused by insufficient mitochondrial production of ATP energy. Inadequate ATP energy causes lethargy, failure of the immune system, and repair failures. Mutated damaged cells are not cleared via apoptosis.
Damaged cells become necrotic and exacerbate inappropriate immune responses.
Mitochondria ATP energy production declines from failure of DNA repair.
Cancer is caused by failure of DNA repair.
DNA repair fails for lack of mitochondrial ATP/NAD+ support.
Supplementing mitochondrial energy production cofactors does significantly increase ATP production in mitochondria. These cofactors are NAD+ from nicotinamide, carnitine, alpha-lipoic acid, ubiquinol, and vitamin k2.
Restoring adequate ATP enables clearance of necrotic cells.
Restoring adequate ATP enables clearance of damaged mitochondria.
Restoring adequate ATP enables DNA repair.
Restoring adequate ATP prevents cancer by apoptosis and DNA repair.
Exercise stress causes healthy mitochondria to multiply.
Keith – thank you so much for your extensive research and experience. Some of the things you recommend I am already doing. I do ubiquinol, but will boost to 400mg now and will up zinc carnitine and add taurine.
Unfortunately, do to 5 hernia operations, my surgeon has read me the riot act on squats, dead lifts and leg presses (my 3 most favorite exercises for last 50 years or so) and also most Ab work.
This is a real crimp, but he has done over 7500 hernia and if I get one more it will set his all time record. He says I was not age/weight class appropiate, so i have stopped these heavy exercises since June 2016. I really miss them.
Your 1 gm. Nicotinamide may be a bit of a problem. I was a bit in shocked at the cost when I looked it up today.
Question – will your 50 mg of DHEA increase BPH problems or will pregnenolone cause problems? Haven’t tried these yet but am putting together a supplement order now (ouch on the Nicotimamide!).
Again – thanks,
Regards,
Greatdanes (Mike)
Keith, Mike–
I need to advise research into the potential downside to supplemental alpha lipoic acid (aka lipoic acid, thioctic acid) and suggest caution if you have any mercury “silver” amalgam fillings or have any history of mercury exposure (broken florescent light bulbs are common potential exposures, although playing with “liquid” mercury as a child (from themometers) is perhaps more common); ALA is a known to chelate mercury and it is also capable of passing the blood-brain barrier. Andrew Cutler did quite a bit of research on this and there ‘s quite a bit of anecdotal evidence that doses of ALA taken at too high and too infrequently can severely aggravate someone showing low grade symptoms of chronic mercury toxicity.
That being said, I was taking high doses of ALA once a day, and it took a few years before I started having increased symptoms of said toxicity.
I consider myself fortunate that I stopped when I did….
GreatDanes:
Pregnenolone and DHEA are inactive reservoirs of raw material for producing active steroid hormones as required. Our bodies produce these inactive molecules in a daily cycle between 4AM and 10AM. As we age we produce less. One activity of pregenenolone is notable. During WWII the USArmy gave 100 mg of pregnenolone to half of a large sample of recruits. The recruits were given a competency exam. Those who received the pregnenolone before the test scored significantly higher than those who did not.
Keith, you wrote:
“. Zinc deficiency causes benign prostate hypertrophy and difficulty urinating. Men have a built in signal for zinc deficiency that can be cured in two days of 50mg/day.”
If we can cure enlarged prostate with 50mg zinc for 2 days it raises the question: why is surgery performed on so many older men ? (I think I can guess – no money for the doctors in zinc tablets.) Do you have a source for zinc curing prostate hypertrophy? – it would come in handy to convince sceptics. Also, how did you reverse your PH without zinc?
Re acetyl-l-carnitine and alpha-lipoic acid, when Bruce Ames supplemented old rats with ALC they became much more active but their mitochondria were spewing out lots of free radicals so he added the ALA to mop them up. It’s therefore important to take both together.
Re the B3, AIUI nicotinic acid is metabolized in the body to niacinamide, but with cardiovascular benefits. So unless you can’t stand the flushing, NA might be the better option.
How are you making your probiotic liver pate and how do you ensure it’s got K2?
Stuart
Method for fermentation of Bacillus subtilis vitamin K2:
Homogenize two 50 gram packets of frozen natto into one cup molasses plus one cup of nutritional yeast.
Dilute to 3 liters.
Aerate at 3.5 liters per minute with aquarium air pumps and air stones.
Add molasses if appropriate.
Fermentation ends when the ferment bubbles over after approximately 3 days. Foaming may be prevented by covering the surface with vegetable oil.
Recipe for Bacillus subtilis pate:
Homogenize fermentation liquor product with 3 pounds cooked beef liver.
Add liver pate spices.
Slow cook the liver slurry to a paste.
Cool the paste and mix with equal amount of mixed cream cheese/ brie cheese/ feta cheese/ labneh kefir cheese inoculated with limburger/swiss and aged several months. High salt in the feta prevents botulism.
To your health,
Keith
Keith, thanks for the recipe. Just to clarify a few points:
Presumably you dilute with water dechlorinated and sterilized to prevent contamination by wild bacteria and yeast. Do you also cover the molasses starter while fermenting or use an airlock to prevent contamination by airborne bacteria and yeasts?
The aeration – is that continuous for the 3 days of fermentation or do you just aerate it before starting?
Nutritional yeast: I’m guessing this is dead yeast cells to supply the bacteria with proteins and minerals. Home brewers use this to prepare yeast starters before adding to the wort. Presumably also why you’re using molasses rather than sucrose, for the extra minerals.
Re the cheese: is that a mixture of all the cheeses or are they alternatives ie cream cheese OR brie OR feta etc or cream cheese AND brie AND feta etc. You then inoculate that cheese with a mixture of Limburger and Swiss cheese and ferment that for several months?
By my calculation you’re winding up with 6-8 pounds of pate – that’s a lotta food. How long does it keep in the fridge, do you freeze some of it and how much do you eat a day?
Apologies for all the questions, I just want to get your recipe clear in my mind. I’d also appreciate your input on how you cured BPH without zinc.
Thanks in advance, Stuart
If you were able to do Mediterranean diet, I’d stick with that, but eliminate olive and other oils from it. It works despite, not because of, oil. The higher scores for calcium should represent your plaque melting away and the body pitching in. Total cholesterol went up on Med diet, which is normal using olive oil or other oils. Olive oil is 14 percent of calories from saturated fat, same as a Big Mac. Saturated fat blunts the liver cells whose job it is to remove excess cholesterol, so it builds up when you consume saturated fat. If you stick with whole food plants and avoid oil, dairy, meat, fish as much as you can, the evidence is overwhelming you will reduce heart attacks, strokes, and deaths. See Dr. Esselstyn’s video “treating the cause…” on youtube for proof. Just tests don’t show the hard enpoints like death, stroke, attacks, they are only stastistics. I like to stick with hard endpoints since my calcium started out at 579, time to get serious and find the only diet with 4 years and 200 people 90 percent of whom were able to eat the diet and none of them got any further hard endpoint events. Calcium areas are stable, it’s the soft plaques that kill you. Your diet controls and reduces these soft plaques. I feel that is the best approach since it’s got human trials over 4 years with hard endpoints. Find a study like that for keto, etc. I couldn’t so here I am. It’s working well for me, maybe you should think about it. I can’t help but think if a couple hundred people went 4 years and had total cessation of their heart problems, I won’t be the only exception. ??
ALan – not on niacin for several years now. When I too 500 mg of niacin 2X day my HDL’s shot up to 3 readings of 125, 127, and finally a reading of 135. So my doctor stopped all niacin for me. that was probably sometime in 2014 if I remember.
ALan – also my mother has extremely high HDL’s – always over 100 (no supplements of any kind to get those numbers) and she is in her 90’s.
Greatdanes,
I was just pointing out that research shows that cardiovascular problems in cases of very high HDL might be related to a genetic quirk … women’s HDl seems to be ok at a higher level than mens, although in the 100’s also suggests a genetic quirk. She might have a genetic predisposition to CVD also because of this, but it might never have been expressed perhaps due to other factors inhibiting gene expression.
Thanks ALan – definitely worth checking out. One thing retired people with useless Ph. D.’s seem to manage is doing research. My doctor just said the same thing you pointed out about HDL’s but he doesn’t seem sure about what can be done.
Greatdanes –
You never mention being diagnosed with CAD/CVD nor having any symptoms of such except for the high Calcium scoring…
this scoring may of course indicate an increased risk. Given that this does however indicates some degree of arteriosclerosis, you might want to consider the Pauling-Rath hypothesis, in light of there being little else advised for high (potentially genetically related) HDL-C increasing your CVD risk (besides lifestyle changes (ie. avoidance of smoking, etc.).
The hypothesis, in a nutshell, proposes a normal body process of healing the insides of specific arteries that become easily damaged/inflamed when there is a chronic low level scurvy -(ie. lack of vitamin C (ascorbates)) and insufficient collagen production and/or ingestion. This proposed normal body process is protective of inelastic blood vessels and minimizes the potential leakage/hemorrhaging that might occur when the vessels become damaged and is characterized by the buildup of plaque, sort of like mortar covering a crack. Cholesterol and calcium and other agents play a role in the development and maintenance of this protective plaque. (I don’t know if the theory answers the question as to why the plaques seem to continue and thicken with time, but again, this is just the “nutshell, most likely to raise more questions than to give answers).
The theory proposes that supplying large amounts of vitamin C (ascorbates) daily together with sufficient amounts of lycine (and some other amino acids (eg. proline) perhaps typical in high collagen foods, like gelatin) can lead to a reversal of the build up of plaque and the inelasticity of the arteries, in effect reversing arteriosclerosis.
This theory has its roots in the understanding of lipoprotein(a) being a surrogate for ascorbates in humans:
https://www.ncbi.nlm.nih.gov/pubmed/2143582
Given the lack of pharma drugs being involved, it’s highly unlikely that this theory has ever see any in depth clinical trials, but a follow-up on Rath’s works over the last couple of decades may prove me wrong.
Perhaps it’s possible that eating a high vitamin C diet with sufficient amino acids to support collagen production (whilst minimizing other agents that might further trigger arterial inflammation) might suffice to start the reversal, esp. if competing amino acids (like methionine) are reduced to a minimum needed. Hence, the oft suggested plant-based diet for heart patients might be working in some way similar to that proposed by Pauling-Rath.
Alan – I have not shown any real indications of CAD/CVD. I have had 2 Eco’s and they were pretty good, age adjusted (readings taken at 85%. of max heart rate). Velocity’s were good and Ejection Factor of around 65%, which is apparently good.
2 different cardiologists for each test, one says things OK, the other is bothered but couldn’t say why, and he has since left my State so I can’t contact for more info.
Calcium score was on a 64 slice CAT, we don’t have any 128’s yet im my home State, so older 2D reading. My GP thinks Eco’s were OK due to collateral circulation development but would need a 128 slice 3D to make a better guess.
Rath et. all, Pauling is being revisited by me.
http://www.drdach.com/Heart_Disease.html
seems there might be worth trying.
The other worrisome problem is hsCRP just came in at 2.74 and my 3 previous readings were over 5, so inflammation going on somewhere, probably vessels. I need to fix this and neither of the cardiologists seemed to care and my GP doesn’t bother because won’t pay so I do these tests on my own dime through Life Extension.
Another possibility that worries me is the unknown factor of embedded cholesterol crystals in the plaques, since they herald ruptures, but there is not an easy way to measure them right now.
Myeloperoxidase number was in the good range and so was APO-B.
The last year I have been mostly concentrating on AMPK, HBA1C, Insulin levels and the last 2 have been very good. So, inflammation and calcium?
Have also just gotten 1 mg. tablets of cyclodextrin
https://www.sciencedaily.com/releases/2016/04/160408112235.htm
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4878149/
Definitely going to try the Rath/Pauling Protocol now.
Hi Greatdanes, I notice that in the mouse study of cyclodextrin that they were injecting the CD subcutaneously. Do we know if CD is absorbed when taken by mouth?
Also where did you buy your CD tablets?
Lot of Gouda Cheese is made in US, especially Wisconsin. Any idea if the Vitamin K2 content of this Gouda is similar to Dutch Gouda? Can’t seem to find an answer to this question. Wisconsin also produces lots of aged Gouda.
Thank you much
Jay
If it’s not in the database, I don’t know.
Dutch Gouda is a variety (as opposed to smoked Gouda, etc.). It’s the one that usually has the red rind. I don’t think it’s actually referring to where it’s made.
My strength has went through the roof on just 500micro of mk4 and 100micro of mk7. I was sick for a couple weeks, and sat on the couch and did not workout at all. My bench went up from 205 to 245. And my shoulder pain is gone. Is this normal?
Depends. Could be the perfect storm: you were ready to go anabolic and the period of recuperation allowed you heal the injury and gain strength…or the rest time allowed your shoulder to heal enough to increase baseline function to lift more weight. See “Body by Science” – Doug Mcguff.
Sounds great. Could be coincidence, or could be testosterone.
My experience with starting on 1.3 mg of MK4 vitamin K2 was that it boosted connective tissue production, boosted testosterone mildly in an older male, and it also participates in some of the energy production in the mitochondria. It will definitely help bone formation in older adults.
If you are of an age to be getting artery calcification, MK4 works with the Matrix GLA Proteins to halt soft tissue calcification that might also be an issue for that shoulder.
Can one take Serrapeptase with K2? Thanks!
Really appreciate this post, thank you! 🙂
Thank-you for very informative discussion. It helped me resolve some questions on the MK-4/7 controversy. For severe osteoporosis, I am thinking vitamin MK-7, K1 in morning and MK-7 with high dose MK-4 (1mg) at dinner followed by Ca/Mg before bed since most bone remodeling is done at night?? Any thoughts??
Also, I am combining with Earthing which seems to help preserve minerals in body.
Earthing is something you might look at if you haven’t already. http://www.earthinginstitute.net/ and http://www.earthinginstitute.net/wp-content/uploads/2018/08/2018-congress-on-integrative-medicine-poster.pdf
It’s my understanding that Ca levels in bloodstream are high at night, implying lower during day. This would make the hours immediately preceding sleep to be the time when Ca is pulled from teeth and bones to flood the sleep metabolism and the time immediately following awakening to be when Ca is put back into teeth and bones (remodelling). Optimum Ca intake in the American models is 800 mg, in Euro models 750 mg. Good convergence. As max absorbable dose is 500 mg, a split dose is necessary. Upshot: I dose 400 mg in late evening to support rising Ca levels and 400 mg in morning to support remodelling, both from dairy and in isolation. K levels, not surprisingly, are inverse to this: low at night, rising in morning, circadian noon peak, lowering in evening. Thus, I shoot 1 mg K2 MK4 with the morning Ca dose. In 2013, I took a 28 foot fall off of a ladder onto a 45 deg slope, with full weight transfer onto my right foot. High grade sprain only (3 months rehab, all hail intensive heat-cold contrast therapy). No break. No fracture. Not even a hairline. Doctor x-rayed twice. Couldn’t believe it. I was 50 years old, with 25 years of backpacking experience. In 2015, I did the John Muir Trail (again): 200 miles, 3 weeks of continuous backpacking at 8,000-12,000 ft. Performance: 100%. Hat tip to Dr. Weston Price.
Just noticed your post. So you have had success with MK4 in morning. I have been using at night with MK7 and only MK7/K1 in morning. Sounds like you suggest AM and that remodeling is in morning not night.
How heat sensitive is the K7 in Natto?
If I do not want to consume the soy beans is it possible to swish/agitate the natto in warm water to separate the slime from the beans and then drink the liquid?
Since MK7 lasts 3.5 days in the body can I just consume a loading dose every 3 days? What would that dose be? I have been eating my natto with a teaspoon of cod liver oil or a teaspoon of red palm oil along with 1000 IU of D3. Does that seem functional?
You don’t know where the K2 is located inside the beans or in the slime, right? Start there, ask around. NattoPharma is a company that extracts K2, nattokinase, etc from natto. They might offer suggestions for you.
The idea of loading doses to span 3.5 days will result in less total K2 in the body, as it has a half life. You want the most area under the curve of K2 in the system, it won’t be the same on day 3 as on day 1, not even close. Natto contains MK7, a highly potent form of K2 which is oil soluble and persistent. 360 u/day results in fully carboxylated MGP, which keeps calcium away from soft tissue. It’s not known if this will keep it away if the body is wanting to put it there, however. People with artery disease, for instance, have plaques which can destabilize and cause clots, so the body throws calcium at them to keep them from rupturing. If you just take K2, that’s fine, but if the diet is atherogenic, the body will fight you on it, and probably win. Taking K2 so far hasn’t shown any positive results in studies, though there are a few anecdotes around that the calcium scores reduced. They didn’t say by how much, or how many people. Just typical slipshod references to it. Like Kris Kresser and I think Dr. Sinatra mentioned in passing. We haven’t heard back from Dr. Leon Shurgers anything about his 2 year study of couple hundred people and their calcium scores while taking the 360 units/day of K2. It was funded by Nattopharma, and was to be out in 2017. So I guess that showed either no effect, or even made things worse. Calcium in arteries doesn’t seem to be just a vitamin deficiency but a reaction to diet and poor nitric oxide levels in the arteries…not likely to correct it with a vitamin alone. It can be corrected, and has been, but took a lot more than that.
The article has a section on light and heat stability.
Hi Chris,
This is from your article:
Light and Heat Stability, and Proper Storage of Vitamin K2:
Vitamin K is only slightly sensitive to heat, but is extremely sensitive to light.
> Can you be more specific about the heat Sensitivity? I usually heat up some curry sauce or tomato sauce and add the natto beans. I have to cover the smell and taste. So how much to I need to cool the sauce after I take it to a simmer?
And… on light sensitivity — do I need to keep the natto in an opaque container if it is just exposed to the light in the refrigerator?
Thanks – Dwight
Hi Dwight, please see the references in the “click more” part of that section for details.
Hi Chris,
When look at the references in the “click more” I only find– Vitamin K1 (phylloquinone) content of edible oils: effects of heating and light exposure -.
Is there something I am missing in relation to K2 or– are you implying that K1 and K2 are comparable in regards to heating and light exposure?
In the absence of studies directly testing it, it is fair to assume similarity.
Chris,
Thought folks might be interested in this info:
http://www.meguminatto.com/about_natto.html
Finally found my answer to the heat tolerence:
Is it possible to cook hot dishes with NATTO?
When the enzyme Nattokinase is heated to a temperature of 150 degrees Fahrenheit or warmer for more than 10 minutes, the enzyme loses its effectiveness. However, you may add NATTO to your favorite pasta dish, to an omelet or hot dish of choice at the end of preparation and NATTO will keep its nutritional integrity. See our Recipe section for ideas and preparation tips.
This is another link with an overwhelming amount of info on Natto:
http://www.soyinfocenter.com/HSS/natto1.php
No my next rabbit hole is find the difference in Bacillus Natto and Bacillus Subtilis and I am still not sure if I rinse off the sticky substance (glutamic acid polymers), which forms long silvery gossamer threads when natto is lifted from a bowl I will get the full effect of the MK-7.
Any info on this would be appreciated.
Interesting long reads, I have been trying to research the truths/benefits of the GP butter oil/cod and if its really worth the money or if there are better things out there. NO WHERE seemed to tell you how much k2 was actually in it, and the owners didnt say it either. How did you find out it only has like .5 mg per pill?
Regardless, according to your research, you are saying that emu oil is the better option for the k2 mk4, is that correct? And you stated that k2 mk4 i “activator x”, therefore, emu oil is the better option for trying to ‘heal cavities’ or remineralize teeth? That is my most important question. Unless people swear that there is other ingredients in the butter oil that is healing their teeth. Just seems odd that emo oil has like 8x the amount and you aren’t hearing as much about people taking it.
OH another question (related to your long study about Price and how he tested with butter oil).. if you /others strongly believe k2 mk4 is activator X, why would Price use butter oil? In which you’ve proven there are better alternatives by far… including goose liver pate, which is even higher /cheaper per 100g? (100g of pate is easier to eat than 100g of pills or oil, and again cheaper since the emu oil only has 4 oz total)
thoughts? thanks for the writeups
These are in my database.
What does “these” mean? I asked questions and asked your thoughts and you replied with this dismissive answer. Not even a link if they are ‘in your database’
The items you discussed.
Please ask specific questions and not for “my thoughts” about anything. It takes me many hours to answer all of the specific questions, I cannot possibly answer open-ended ones.
Oh My God. I never knew all these benefits of vitamin K2. A friend of mine was diagnosed with vitamin K2 deficiency so I was searching the internet on her behalf to find some useful info regarding it. Trust me, your article is really helpful.
Dr Masterjohn,
thank you as always for your invaluable information. Any thoughts/comments on this option: https://www.naturalpartners.com/us/full-spectrum-vitamin-k/AL0250PAR?x=
?
Thanks,
Lilian Holm
I’d prefer something with less K1, and lower doses overall for more control. Not sure the point of the low-dose D/A/E in it.
Hi, I am taking Ortho Molecular Products K-force. It contains Vitamin D3 as cholecalciferol, 125 mcg,(5,000 iu) and Vitamin K2 as menaquinone-mk-7 180mcg.
Would love to know your thoughts. I guess I need to add MK 4 as well?
Thank you for your time.
Donna Elliott
Too much D for most people. K2 is fine though I’d rather see it include some MK4.
5000IU/day is too much D? IIRC Michael Holick said in his book The Vitamin D Prescription that most people could take 5000 IU/day pretty much indefinitely. Also see this blog post by the late Robert Heaney
http://blogs.creighton.edu/heaney/2015/02/13/the-iom-miscalculated-its-rda-for-vitamin-d/
which reports that some Canadian statisticians found that the IOM got their maths wrong and the requirement is closer to 9000IU/day. Heaney’s estimate is 7000IU, as he says still an order of magnitude greater than the IOM limits. Heaney also points out in this post
http://blogs.creighton.edu/heaney/2014/06/05/vitamin-d-and-the-nursing-mother/
that nursing mothers require 5-6000IU/day to ensure adequate D in their breast milk. Of course given that UVB exposure, dietary D and individual’s dose-response all vary, the only way to determine your individual daily dose is to have regular blood tests and adjust accordingly.
Prior to coming across his blog I wasn’t aware of Dr Heaney but judging from the fulsome tributes on his death in 2016 he was THE premier researcher into osteoporosis being the prime mover behind the Omaha Nuns Study on bone health. As I’m witnessing the effects of osteoporosis on parents and neighbours I have become interested in preventing it in me and my family. Dr Heaney’s blog is particularly useful, especially his point about the interaction of Vit D status, calcium intake and protein intake ie
1) Vit D status must be adequate to enable dietary calcium absorption, typically 125nmol/L (50ng/dl)
2) Even if D is adequate, dietary Ca also has to be sufficient
3) If either of these conditions are not met then the body breaks down bone to scavenge the Ca it needs for more critical body functions
4) To rebuild that bone adequate protein in the diet is required to build the protein matrix destroyed in the process of bone resorption. Dr Heaney found that elderly adults required 1.2 grams protein per Kg of body weight to rebuild osteoporotic bone, 50% higher than the recommended intake of 0.8gm/Kg.
5) Bone rebuilding is also dependent on the stimulus provided by weight-bearing exercise.
This is explained in this post
http://blogs.creighton.edu/heaney/2013/04/08/defining-normal-part-two/
and the other posts in his “What is normal” series.
Yes I’m very familiar with their work, I just disagree with it. I laid out these arguments in a series on “ancetral 25(OH)D” on the weston price site.
Chris, it takes 7,000 IU of D3 per day to just get me to a level of 40 on my 25-hydroxy vitamin D labs. And I’m an ApoE4 homozygote…so I’m sticking to it that amount. 🙂
Ok. 🙂
Chris what do you think about Jarrow K-right? It has 1500 mcg MK4 and 180 mcg MK7, plus 2000 iu of D3. Is that a safe D3 level? I don’t want to give my mom too much daily. Daniel
MK-7, made from bacteria, and found in natto (fermented soybeans) is not a bioactive form of vitamin K2 . In fact, research by Yanagisawa, 2003, shows a large amount of water-soluble MK-7 in natto. Vitamin K2 is a fat-soluble vitamin…If MK-7 is really a form of K2, why is it water soluble? It cannot be both ways. Is MK-7 not really what the industry says it is?
While there is some function to the MK7 form of vitamin K2 in the body, what the body makes for its own use is the MK4 form of vitamin K2 which is converted from vitamin K. There is a large difference in the half lives in blood of the two vitamin K2 forms, MK4 has a half life of 3.5 hours while MK7 has a half life of 3.5 days. While there are arguments over the meaning of this, one hypothesis is that the body is highly adapted to use of MK4 as it is present in all mammals and MK4 may simply be more mobile in the body than MK7. The MK4 gets into a variety of places, helping manage calcium metabolism, regulate blood sugar levels, cell energy levels, and build portions of the myelination of nerve cells. The six very successful Vitamin K2 Research Trials in Japan were all run using the MK4 form which resulted in 80% reductions in bone breakage rates in elderly adults.
The longer side chain of the MK7 form makes it more fat soluble and the higher MKx forms of the vitamin generally are present only in the liver and have no function in the body that I’ve read about. Small mammal trials with birth into a sterile environment and no digestive bacteria result in normal vitamin K2 function, so the MK7 bacterial form is not essential to mammals. The MK7 form may well have some function in carboxylating Matrix GLA and Calcitonin present in the blood where MK7 tends to reside.
In a number of reviewed reports on vitamin K2, I’ve noted the authors missing the important difference in chemistries between MK4 and MK7, at times conflating the two molecules with the result that research results found with the MK4 form are often used in the promotion of the MK7 form in much promotional literature and even some research reviews. This leads to a very confusing situation unless one examines the original research for the precise form of Vitamin K2 in use in order to classify the health outcomes of MK4 and MK7 forms separately. Animal livers often contain MK4 while cheeses, natto, and other products may contain mostly MK7 with some MK4 present in cheeses. You will note that food sources of vitamin K2 often don’t separate the two forms by source.
I hope this answers all your questions.
“The six very successful Vitamin K2 Research Trials in Japan were all run using the MK4 form which resulted in 80% reductions in bone breakage rates in elderly adults.”
Are you referring to studies by Sato (so?)? I believe most of them have been retracted he and his work quite discredited.
I was not referring to the retracted article by Sato. There were six successful trials with MK4 over several thousand patients so
Sato’s retraction with 178 total patients is rather minimal. Recent work has continued at lower doses of MK4: https://www.ncbi.nlm.nih.gov/pubmed/23702931
Thank you
MK7 is fat-soluble.
That’s it? Please give us your analysis of the study by Yanagisawa, 2003 which states that MK-7 in natto is mostly water-soluble, If It is fat-soluble why did Dr. John W. Suttie, a life-long Vitamin K-2 researcher, give this study as a reference in his books? And what about Viridis and others announcing they made a “water-soluble” form of MK-7? Was it not water-soluble to begin?
I wonder if the water solubility of MK7 is a promotional statement and a concept coming out of the manufacturing process. See this informational write up that describes a water soluble MK7 due to an added ingredient yet also refers to MK7 as primarily fat soluble in technical terms.
http://www.nutritionaloutlook.com/heart-health/water-soluble-vitamin-k2-mk-7-ingredient-eases-formulation
Please link to the study, thanks.
MK7 at a dose of 360 u/day fully carboxylated MGP by test in humans, according to Dr. Leon Shurgers, PhD, a primary K2 researcher. So it is bioactive, whatever its solubility.
Sir, does continued high doses of k2 mk4 and k2 mk7 actually remove hard plaque from the vessels, while directing calcium to the bones as well. Is using higher doses of these k2’s considered a artery cleaner in your opinion. We know that k2 inhibits further deposits onto the vessel walls, but how about removing whats already cemented on the walls. May GOD always bless you and your family.
Dear Stevie, I have used an excellent product made of liquid EDTA from Cardio Renew, and the EDTA cleans the hard calcium deposits slowly right off the blood vessel walls. Who knew till lately that K2 mk4 and 7 “tell” the calcium where to go, to the bones and teeth. Wish we would have known this sooner. My high blood pressure is medicated, but I am now getting great results with the edta, slowly my HBP is changing even while on the meds, I know that a few more weeks and I can ditch the meds, and have Dairy far more often, Yes certain cheeses are high in k2, but pizza, milk shakes, grilled cheese sandwiches, cottage cheese, yogurts, ice cream, soooo much dairy and no k2 lined my arteries real good (bad), so now I have found EDTA liquid is really liquifying the harden plaque, thank you JESUS THE CHRIST.
In my experience and readings, it’s not yet clear that K2 will prevent further calcium build up in arteries in humans. I don’t see any real evidence yet of that. There are animal studies, and people saying they can feel it is going away, but actual images and measurements would be required to know for sure, and I have yet to find any.
The idea that K2 will remove existing calcium from arteries, without significant dietary or other changes is unlikely, in my opinion. Calcium is not there totally due to low K2, it’s also put there by the body as a stabilizer for soft plaque. It can be produced in lab animals simply by feeding them a high saturated fat and cholesterol diet, similar to the US diet, or Atkins, or Paleo type diets with low calories from carbs and high calories from fats. The only thing that really worked to save the lives of these poor animals was dripping a tiny amount of sodium nitrite into their drinking water, which prevented the plaques from forming.
I bought some K2 pills that are 600 mcg. Not sure if I’ll be able to cut them in half or not. The question is, if I want “200mcg per day”, and I take the 600mcg pill once every three days, am I really going to get the full benefit of 600mcg, or will I only get the benefit of (say) 200mcg on day one and then nothing on the subsequent days because I excreted the rest of it?
Basic question: cut the pills and take daily, or take entire pills intermittently?
Intermittent is probably fine.
Is it safe to assume that cOCN won’t have the chance to become ucOCN and circulate freely and abundantly systemically without adequate vitamin K? But then how is is that ucOCN is associated with vitamin K deficiency? Perhaps acutely only.
This part is a bit confusing – I am trying to read some sicentific articles on it, but it is still confusing.
It certainly is confusing. If I recall correctly, the body keeps some uncarboxylated osteocalcitonin around as its used as a hormone in the body, so the carboxylation of osteocalcitonin is well proportioned and never actually gets totally complete. The body discards the excess MK4 Vitamin K2 to keep some ucOC around for use as a hormone. This is why there is research saying that both 1.5 mg and 45 mg daily doses of MK4 work in different trials.
Note that the body normally makes enough MK4 by converting it from vitamin K but this process slows with age and then people need to supplement to replace the missing production. I would take the 45 mg a day if I had a dangerous amount of artery calcification or medically dangerous bone loss. Since I’m in good health my dose is in the 1 mg to 6 mg range and I found even 1.3 mg over 18 months to be very helpful with reversing artery calcification.
I very much appreciate your input!!
David, could you please clarify that i understood you correctly?
You said “1.3 mg over 18 months”. I’m assuming you mean 1.3 mg per day?
You also said you found that dosage to be “very helpful with reversing artery calcification”.
How did you determine that it helped with artery calcification? Did you have any medical scans?
I started taking 10mg of the Thorne MK4 per day. But after a few weeks my teeth have become a lot more sensitive.
I don’t eat dairy due to an intolerance so my calcium intake was probably quite low. I’ve started taking calcium supplements now which is why i did the high dose of the MK4.
But after reading around a bit, including from one person in this thread, (Brik March 27, 2017 at 5:40 pm), vitamin K2 can have adverse effects in people with low calcium levels.
My other theory is perhaps MK4 should be taken with MK7 as the latter is supposed to be best for transporting calcium to the bones?
Do you have any thoughts on this as you seem to be quite knowledgeable on this subject?
I didn’t have any scans for calcium, but the symptoms matched up with those of artery calcification and I had them steadily for twenty years until I started on the MK4 & MK7 supplement. It was a surprise that the symptoms started decreasing, I didn’t know at the time they were calcium related. The symptoms did come back when I started on a second multiple mineral supplement by mistake and was getting over 2000 mg of calcium daily for a few months. The symptoms returned until I figured out I was taking two mineral pills so artery calcification is the simplest, most likely explanation.
I was taking 1.3 mg per day during this period. Your 10 mg dose is reasonable and might be a little high if your physiological needs for MK4 are low. Generally the body cuts up and discards what it doesn’t use so taking MK4 is very safe. You can take the MK7 if you wish, but its not as functional at the MK4 form in research trials. Some people are sensitive to MK7 and get anxiety, sleeplessness, and a thumping heart beat from taking it after a couple of days while MK4 never has this problem.
All the fat vitamins, vitamin A, D3, K, and K2 work together so you might try taking dose that science has found most effective in recent trials.
I have a 540 calcium score, 4 months ago got a stem implant. Doctors placed me on Crestor 40 mg, lowered to 10mg due side effects. Zetia 10mg.
Since both of these drugs interfere with the production or absorption of K2-MK7.
How should I start a K2 + D3 treatment along with medicine I am taking now?
What dosis of K2 + D3 should I take? Since half life of both of these drugs is high should I take them every other day?
Thanks
Jerry Lectora
If vitamin K could affect the action of the drugs, your doctor should arrange that your levels be checked often enough to assure the drugs are not impacted by either your diet or your vitamin supplements. I think they used to just say “don’t eat this, don’t take that” but nowadays they test your levels and increase or reduce dosage to fit your lifestyle. I have a friend who gets his levels of coumadin checked about every 2 weeks. HTH
One more thing, about doses. I take both the form Mk7 and Mk4 about 400 of 7 and a few drops of Thorne liquid Mk4 (each drop contains 1mg Mk4). I have a 579 calc score.
I take 5000 IU vitamin D3 per day as well.
I am on a plant-based diet for heart disease. I do not believe heart disease or calcification of arteries is a vitamin deficiency, it’s a food-borne illness that responds best to whole food plant based diets like that of Dr. Esselstyn. He’s got the goods on it, and can halt-reverse it predictably with ease. I’m doing great with it and feel it is worth the work to get on it and stay on it. The point is, food causes it and food alone can prolong it despite all our efforts–we have to change the food before we expect to change the outcome. If we do, then the supplements and drugs do stand a chance. If we don’t they won’t help. I’ve seen this all over the place and there’s no escape at present.
Not sure how heart disease can be dietary but not involve a vitamin deficiency. An excess? Then why would supplementing, adding more, of anything, help? Do you literally believe that it is an infectious disease? —I don’t think you will find much evidence supporting that—or do you mean “food borne illness” as a metaphor?)
Also, has it occurred to you to question why it is your “healthy” diet requires any supplementation? I’m not telling you to eat differently. Perhaps you ate poorly in the opposite way and now this diet is therapeutic compensation. For you. For now. Not a universal panacea against heart disease.
It just seems disingenuous to be promoting a “plant based” diet on a page dealing with a vitamin deficiency that many of us were brought to (the page and the deficiency) by that same inadequate diet.
Well, food-borne illness means to me that if you take away the foods causing it, it goes away, in much the same way a vector such as fleas or mosquitos carry diseases with them. Food can provide building blocks for disease or health. Many believe all food is good in moderation, or small amounts. Variety is spice of life, etc. This despite evidence to the contrary. The whole food plant-based diet is well documented and 100 percent effective despite age, or extent of illness. It’s not my claim, in other words. I’m following it because it’s the only diet that has been proven. Not many realize this has happened, but it has. Having b12 is part of it and I do supplement with that, as well as D3 and K2. I did eat a delicious but nasty high meat diet that put me into trouble, and this is therapeutic towards undoing some of that, as much as I can, and at least stopping the progress of the disease. I realize the diet sounds extreme and improbable, but it’s not that way in many parts of the World where billions don’t have much if any heart disease. It makes sense to try their diet, and sure enough it does work. Not maybe, not seems to, but works 100 percent of the time. I take supplements because even if you do eat meat, today the b12 is less present there. Grass fed has more because the bacteria that make b12 are in grass but not so much if any in grain. Dr. Caldwell Esselstyn’s research just completed on 200 heart patients showed the ones who did his diet for 4 years had zero further heart attacks, zero strokes, zero deaths. The ones who failed to do the diet had 66 percent of these. What’s interesting is the compliance rate was 180 out of 200. I expected the diet to work if used, but had no idea it would be so accepted and practiced. I am not in love with this diet, just trying to keep living, of course. I loved my steaks, hot dogs, fish, name it, I ate it. But this diet has a lot of benefits beyond the heart disease too. No more acid reflux, ED is half gone away, lost 40 lbs am now 180 at 6′ 1″, it’s really quite good, and my protein blood levels are better than on the meat diet. I still workout with weights and so on.. So ignore it like I did until it was too late? If I couldn’t do it without a gun to my head, you probably can’t, either. The most amazing thing to me is that this diet’s results are so ignored. If the threat exists and you feel it, I hope you do try this, as it will work, whereas I can’t find anything else with that kind of documentation. I wish I could find a diet with animal products in it, but nope, the one that’s got the goods is plant only. My best, Bob
Bob that isn’t what food-born means.
I am going to reiterate but more clearly: many people, myself included, have been made ill by following the nutritionally deficient diet you are proselytizing for. I can only wish I had not had the discipline to follow my (misinformed) ethical principles for all those years, I might be a whole lot healthier now.
Bafflingly to me, some people with certain problems do seem to get benefit from your diet, at least for a while. Some people with certain problems get benefit from IV poison (chemo therapy). That doesn’t make either a prescription for healthy living.
Antonio, very sorry your diet involving plants didn’t work out. There are people who did Esselstyn’s diet who said it didn’t work. When Esselstyn questioned them to find out exactly what they did, he then said, ok you are going to be ok, we’re going to do this again, this time we’ll do it my way, not your version of may way, and they got well after a death sentence from their doctors. The evidence isn’t that just some people got well as you said, but they all did..all stopped and reversed their heart disease. I don’t know what you were trying to do with your diet, but I know it wasn’t heart disease, and I know you didn’t do it the way Esselstyn prescribes. The evidence is overwhelming, not just in his trials but people all over the world, billions of them who have eaten his way over time immemorial have not had any significant heart disease in their societies, and so long as food for the diet was available, lived long healthy lives. The meat heavy diets in the world have discovered damaged arteries and rampant heart disease when investigated properly. The diet isn’t just vegan it’s whole plant foods and no added oils, low salt, low sugar, similar to native diets in areas where heart disease is almost non-existent, and health is robust, such as Tarahumara Indians of Northern Mexico, who run 500 mile foot races lasting a week, in which men, women, children and old people participate. Their diet is chiefly corn, beans, and squash, almost no meat at all. But it would not mean much had it not been tried here in the US with 200 people, 180 of whom ate it for 4 years and had zero recurrence of heart disease, while the 20 who failed 66 percent had recurrences, including deaths. If your experience was different, well, ok, sorry to hear it, but would certainly not put it up against that kind of evidence in choosing my own path. I don’t think you would if you were me, either.
with regards to plant based versus whole food plant based, I know it sounds like nit-picking, but it’s truly not. There’s a big difference, a critical difference. If you said try veganism as a heart disease cure, I’d agree, don’t do it. You expose yourself to every junk food on the planet that way. Chances are you’d get even sicker. Dr. Esselstyn has treated many vegans successfully for heart disease. The question of nutrition from day one was measured with tests of protein, and other nutrients to spot any deficiencies and found none if the diet was done right. In my case, I may have mentioned this, I was a huge meat eater until age 70, and my protein blood levels tested low-side normal, but well within the range. After the whole food plant based diet, they rose to dead center of the normal range, and have remained there for 2 years now. All my blood tests are superb at this point in time 2 years on the diet. Blood pressure is 110/60. It went down from 140/90. I do weights at the gym 2-3 times a week, and climb 50 flights of stairs 2 steps at a time. I could never had done that previously. My weight has dropped from 220 to 180 and is within 2 lbs of it constantly. There is no medical treatment my doctor could offer me to equal or even approach this. The difference between vegan and whole food plant-based is chasmic, not subtle, in terms of results. If you think I’m a vegan think again, far from it. I wear leather jackets, but I eat only whole plant foods. WHOLE. I am aware too of the pollution from animal industries, and suffering. Hate that all. But there’s a way to do this right, and it’s stunning how well it works.
Heart disease could also be a Vitamin C deficiency. Humans do not make vitamin C in their livers like most mammals do. We need to get enough in food or supplement. Since animals make 1000 mg per day minimum that might be a good place to start.
The point being that animals typically don’t get coronary artery disease like people do. Vitamin C may explain that.
That’s true we don’t make our own vitamin C like other animals do. But it’s very easy to induce heart disease in rats and monkeys by feeding them a diet high in saturated fat and cholesterol, similar to humans in the US. The monkeys died off in months, the rats in weeks. Monkeys were fed actual hospital meals in a research center hospital and they all died in under a year! eek
Thorne’s vitamin d3 + k2 supplement is not vegan but there are vegan ones availible that contain both mk4 and mk7. Heres a link to a vegan vitamin d3 + mk4 and mk7 supplement if youre interested https://www.amazon.com/gp/product/B07CRLLM6C/?tag=lifesupdat06-20&th=1&psc=1
The situation is that in research trials with rats, they gave rat pups doses of warferin from birth to stop their use of vitamin K and its its conversion to MK4 vitamin K2. This resulted in the rats dying of calcified and burst arteries at about two months of age, so the research points in the direction of MK4 being critical to control of calcium metabolism in the body, scavenging it from the soft tissues and helping place it in bones.
Artery calcification is the most critical health measurement of heart and artery disease, so the use of MK4 should be of primary interest for many people with heart disease. Atherosclerosis can be reduced by a reduction in triglycerides caused by going to a low carbohydrate diet. These two items should be major factors in planning your health.
I understand that Vitamin D3 consumption increases the demand for Vitamn K2.
I’ve read that if taking both Vit D3 and K2, that it is best to NOT take them at the same time. Do you agree with this? why or why not?
Hi Eric,
This has been discussed before. In short both vitamin D3 and Vitamin K2 are absorbed easily and do not interfere with each other so there is no need to worry about separating them in the diet.
Hi Chris,
I have been taking the Nested Naturals MK-7 for at least a year along with cod liver oil. I usually take 1 capsule a day although when I was pregnant I took 4 capsules a day. I’m wondering if I should add MK-4 to my diet in the form of emu oil (or the other supplemental versions you recommend).
Basically, my questions are first, does a bioidentical MK-4 supplement affect the body differently than emu oil? Second, using your database it seems like I would have to eat almost half a bottle of emu oil every day to get 200 mcg. Does that seem accurate? Database says emu oil has 416.3 micrograms of MK-4 per 100 mL, and a bottle of the liquid emu oil is 118 mL and costs $45. I just want to make sure I’m doing the math correctly.
I am trying to heal from several health issues and rebuild my body for a future pregnancy so I want to get the optimal dose of K2 and it can be so confusing.
Thanks!
Just stay away from green pastures ‘fermented’ liver cod oil……google the scandal exposed by former wapf vice ceo…..it is crap
How much Mk4 does one bottle of Green Pasture BUTTER OIL have? In the database, it says 81.5. Not sure about the unit.
If it is 81.5 μg/100ml, then the whole bottle has 81.5ug/100ml * 240ml = 196ug = 0.196mg.
If it is 81.5ug/100g, then the whole bottle has 81.5ug/100g * 500g = 407ug = 0.407mg. I don’t know the exact weight of the 240 ml butter oil. But the website says the shipping weight is 1.1lb, which includes the glass bottle. So 500g is a good estimation.
Anyway, the whole bottle has less than 1 mg MK4. In contrast, one drop of Thorne has 1 mg MK4. So one drop of Thorne has more MK4 than the whole 240ml bottle of Green Pasture BUTTER OIL.
Is my calculation correct?
I take exception to the conventional recommended Vitamin K2 requirement.
The following clinical trial showed that tissue calcification can be reversed by taking Vitamin K2:
M.H. Knapen, et al., “Menaquinone-7 Supplementation Improves Arterial Stiffness in Healthy Postmenopausal Women. A Double-Blind Randomised Clinical Trial,” Thromb. Haemost. 113(5), 1135–1144 (2015).
In this trial the daily dose of K2 was 500 micrograms. Yet only 50% of matrix GLA protein was activated. Clearly 500 micrograms is inadequate and a simple estimate for daily requirement would be 2×500 micrograms/day or 1 milligram/day.
My reading of the literature tells me that 10,000 IU Vitamin D3 plus 10,000 IU Vitamin A per day promotes a six fold increase in matrix GLA transcription. These two vitamins were not supplied in the clinical trial. Another six fold or 6 milligrams/day of Vitamin K2 would be required by logic.
Lance Armstrong reports on his website that high doses of Vitamin K2 cause a tingling vibration in the fingers. I find this as well as extra sensitivity in my finger tips. Lance Armstrong had incentive to take large doses of Vitamin K2. Physiological studies report that modest K2 in the 500 microgram/day range confer a 15% increase in aerobic ability. A 15% aerobic advantage is enough to win a bicycle race. Res ipso loquitur after six Tour de France victories.
Studies are underway to establish the K2 daily requirement. Linus Pauling noted repeatedly there is a great deal of difference between adequate vitamin intake and the amount that confers optimum performance.
Kevin,
Thank you for the through review of the varying carboxylation needs for Matrix GLA. One of the reasons for so many varying estimates of vitamin K2 requirements are that in youth and health, all of the body requirements for carboxylation are met by internal conversion of vitamin K to the MK4 form of vitamin K2. When this slows with age or poor health we find loss of bone and calcification of the soft tissues as parts of calcium metabolism. As a result, estimating vitamin K2 needs is a varying target. Better research methods look at carboxylation levels to answer this question.
An additional complexity is that the body also uses uncarboxylated calcitonin as part of its hormonal control system and works to keep this hormone available. So the carboxylation level never gets to 100% with calcitonin. This is part of the reason that MK4 vitamin K2 doses have such a broad range of recommendations and use in research ranges from 1 mg to 45 mg daily as the body actively discards MK4 to preserve a useful level of uncarboxylated calcitonin. This aspect of controlling MK4 vitamin K2 availability may affect carboxylation rates of Matrix GLA as well. The 45 mg of MK4 daily has been noted as the most effective dose at reducing bone breakage rates in the elderly, but lower doses may have a nearly similar effectiveness.
In my own experience I had a turn around of artery calcification symptoms over 12 to 18 months with a supplement with just 1.3 mg of MK4 vitamin K2. As a 65 year old healthy male I noted improvements in testosterone levels from adding more and taking 6 grams of MK4 vitamin K2 daily which is in line with your estimates. Certainly a patient seeking reversal of calcification would want to add vitamin D3 and other nutrients to boost Matrix GLA production along with a matching level of vitamin K2. This relationship with vitamin D3 makes sense, as more vitamin D is available, more calcium is absorbed therefore more Matrix GLA is needed for a well controlled calcium metabolism that avoids calcification.
Such thorough information about Vitamin K2; fascinating and so helpful, especially the details about the Ubiad1 gene expression for the conversion of Vitamin K1 to MK4, which depends on zinc and magnesium.
At 69 years of age, I notice my need for magnesium increasing, with my refusal to part with my youthful stamina to stay active and healthy. From experience (although I don’t know how it feels to be 80 or more) I can say that keeping the body cleaned out, intestinal tract normal with smooth moves, the lymth system and liver in top form, magnesium helps a lot!
Finally, I am very, very thankful for your work! I receive many health-newsletters and I look forward to the more personal time and involvment and depth you express in yours.
Blessings to you from Koh Samui, Thailand
This is a quote from you K2 info:
“Light and Heat Stability, and Proper Storage of Vitamin K2
Vitamin K is only slightly sensitive to heat, but is extremely sensitive to light.
What do you mean by “only slightly sensitive to heat”? I like to mix my natto with some kind of spicy sauce and a veggie to help overcome the small and taste. I’ve been heating the mixture to about 129 F. Is this too hot, am I degrading the Natto?
Hi Chris,
Thank you for this resource and your podcasts!
I’m really interested in K2’s role in oral health (I’m a dental hygienist).
I saw that you mentioned in this article that there are not a lot of studies on K2 and dental caries/dental health. However, I’m wondering if you now know of any recently completed research on the topic or even if any studies are being undertaken currently?
Cheers!
I came upon this article from the people who sell Walkabout Emu oil:
https://walkabouthealthproducts.com/in-defense-of-vitamin-k2-mk-4-dr-prices-activator-x/
“Dr. Weston A. Price had found a fat-soluble vitamin that he referred to as activator X, which not only helped prevent and heal caries, but also helped shape the very faces of the isolated peoples he studied. He felt it was such an important nutrient that in 1945 he added a new chapter to his book, Nutrition and Physical Degeneration. Tooth decay is another sign of vitamin K2 deficiency. Children brought up on diets lacking in K2 MK-4, starting in the womb, tend to have narrow faces and crowded and crooked teeth.”
Dr. Weston Price used butter oil as a source of K2…but apparently, emu oil has much higher concentration of MK4 than butter oil.
Adding to my previous comment…about another dentist, Dr. Lin…
https://www.corganic.com/blogs/news/dental-diet
Some might say Dr. Steven Lin, DDS is the present embodiment of Dr. Weston A. Price, one of America’s greatest nutrition pioneers who started out as a dentist.
Now Dr. Lin is the first certified dentist in the world to write a book about the life-changing results he’s had upon applying Price’s findings to his patients.*
“The Dental Diet” has launched today in the U.S., and you can order the book here.
Dr. Price’s work converged onto the path of Dr. Lin in the most serendipitous way. Feeling disheartened with his dental practice after seeing heaps of patients automatically needing braces with tooth decay abound – and even treating some adults with chronic disease that led to death – he took a sabbatical.
Can you explain why beef liver is listed in the database at 106 and then braised, raw, and pan fried are listed as being so much lower?
I have been taking at least twice the mk7 you have for over 2 years, and no effects on my blood glucose or cholesterol. I have 579 calcium score as of 2 years ago and am not planning to take another scan. I know it will be higher, and I don’t care. Calcium is only 20 percent of plaque volume, and I am sure mine has gone down, since my ED is going away without ED meds, meaning the arteries are opening up. Also, when plaque volume declines from plant-based diets, it loosens up the plaque and the body throws in some extra calcium to stabilize it. This may continue awhile until all the softer plaque is either gone, or stable, then perhaps the body will allow calcium to decline, but maybe not until. I’m doing a whole food plant-based diet to deal with the arteries, not depending on a single vitamin like K2, as some seem to be doing. I also take nitric oxide lozenges Neo40, and large dose L-citrulline a couple of times per day. I don’t know your diet, but for insulin resistance, the whole food plant-based diet with no added oil has been shown to work best, see the site: masteringdiabetes.org for more info. Best of luck!
Curious what doze of citrulline you take
I was taking citrulline malate 2:1 powder from bulksupplements.com in about 3-4 grams 3 times a day. I thought lately that in my case, I should also include L-arginine powder (same source) along with each dose of citrulline. This is due to a test I got on my ADMA levels, which were found to be very high. So I should balance them out with L-arginine, in addition to the citrulline malate I was taking. I get the dose of about 5 grams twice to 3 times a day, and the ratio by volume (not by weight) turns out to be 3 part citrulline and 5 parts arginine. The arginine is just straight base arginine, not compounded with anything else, while the citrulline when I buy it comes as citrulline and malic acid 2:1 respectively. Malic acid is the stuff found in apples, so should pose no problems. Currently I take it twice to 3 times per day, spread out as far as possible and away from food. hope that helps. Bob
..the ADMA test can be gotten from contacting Argininecardio.com and emailing them asking for how to order it. You prick your finger and put some dots of blood onto a card they send you and it goes off to University of Hamburg, Germany for analysis. It costs 150 bucks. Arginine was shown to benefit people with high ADMA levels, but not so much people with normal or low ones. This is so because ADMA competes with arginine to use up the enzyme eNOS (endothelial nitric oxide synthase). Too much ADMA and the enzyme gets used up and arginine then cannot work, you get No nitric oxide. That’s my situation. The answer is to increase the body’s ratio of arginine to ADMA so arginine can again compete with ADMA, and make nitric oxide once again. If you already have a good ratio, then arginine may not work well or could backfire somehow I don’t quite understand yet. My ratio of 3:5 by volume was calculated to give me a 2:1 ratio of arginine to citrulline by weight, which was determined the best ratio to maximize the area under the curve for arginine concentration in blood if taken in spread out doses. The powders do not weigh the same by volume, so I figured it all out so that 3 parts loose volume (not packed down) of citrulline malate to 5 parts of base L-arginine, gives you a 1:2 ratio of pure citrulline to pure arginine, which is the ideal to raise blood levels of l-arginine most efficiently. Someone might want to know their ADMA levels before doing arginine, but doing citrulline malate seems to offer benefits without any risks posed by arginine. That study by Hopkins was only one, they used Arginine-HCL, which is not tested, and many other studies showed benefits, so who knows.
I’ve been taking V2mk7 200 micrograms/ day for about 6-8 wks. after 440 cardiac calcium score. I was expecting stellar results on my unrelated routine II Diabetes monitoring and instead got a Hg1ac score increase of a full percentage point, total cholesterol increase of about 20%, and my fasting and post exercise levels BG levels have gone all over the place after having been more or less stable and predictable for the last 18 years. Not to be overly dramatic, but it feels like my choice is death by calcification or by high blood glucose. If K-2 is supposed to increase insulin sensitivity, why does the reverse seem to be happening? What am I not understanding?
Hi Chris,
Got 2 questions for you if you dont mind:
1. Can I take Emu Oil (walkabout) with this product *Long term*? Will there be too much K2?
Garden of Life Vitamin K – Vitamin Code Raw K Complex Whole Food Vitamin Supplement
in this website: https://nutritionyoucanuse.com/vitamin-k-best-brands-and-benefits-for-2017#best
it says ” there is 100 mcg of MK-7 vitamin K2, along with an additional 20 mcg of MK-4 vitamin K2 and vitamin K1.
Collectively, this results in 120 mcg of vitamin K. For many people, this brand may be particularly powerful because it offers a vegan source of vitamin K2.”
2. I am not comfortable with synthetic K2 forms and want to find natural forms like Emu Oil and Garden of Life… do you recommend Emu Oil + another K2 product that is in “natural form” such as whole foods?
Thanks!
Mike
PS according to this naturopath, Emu Oil is all you need for your K2 needs: (I believe that’s what she says)
https://walkabouthealthproducts.com/emu-oil-dr-weston-price-activator-x/
Thank you Chris for all the information about vitamin K2. I’m interested in trying a cheddar rich in K2, and can’t find one in Las Vegas or online. Where can I order Little Milk Company or other cheddar online?
Hi Chris,
In addition to your valuable information about supplements and diet, I was wondering if you have researched the synthesis of menoquinone. There are science articles which discuss various enzymes involved and specifically MenD which is a thiamine dependent enzyme. This is one of the studies. What does this mean to us? Does thiamine deficiency affect Vitamin K2? I know that K2 is fat soluble and it may be produced by bacteria.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3656419/
Specificity and Reactivity in Menaquinone Biosynthesis: The Structure of Escherichia coli MenD (2-Succinyl-5-Enolpyruvyl-6-Hydroxy-3-Cyclohexadiene-1-Carboxylate Synthase)
Thank you, Chris, for such helpful information.
Can anyone suggest any reason why I seem to get slightly breathless shortly after taking vitamin K? I’m taking just 1 drop of the Thorne K2 one.
I’ve also noticed in the past that I have more mast cell reactions and become more irritable when I’m taking K2.
I’m not taking any other supplements other than low dose transdermal magnesium chloride, though I am using homeopathic B vitamins. I don’t eat much in the way of dietary vit K. I eat a limited PUFA, WAPF-ish diet but without the ferments and broths/gelatin, since I don’t tolerate those, and with only small amounts of liver since it makes me cross and less able to sleep. I don’t eat much calcium from vegetable sources, but I do eat hard cheese every day.
I have plenty of food intolerances and likely nutritional imbalances, but the only metabolic issue I know I have is that I had high end of normal range iron and low end of normal range ferritin and transferrin saturation on the one test I did.
I’m just responding to my comment above. I suspect that calcium deficiency might have been the cause of me becoming breathless from taking 1mg Thorne K2 (1 drop). When I started drinking milk kefir – and drinking lots more of it than the small amount of raw milk I was drinking before – I no longer became breathless if I took K2.
I have since realised that although I’m not very badly calcium deficient, I do have a very low dietary calcium:phosphorus ratio thanks to eating lots of oats and lentils and not eating much in the way of calcium-rich vegetables. Low calcium intake definitely seems to be a big trigger for worsened mast cell reactions for me.
Something I’ve not noticed mentioned on your site is the production of K2 by beneficial E.coli bacteria. The E.coli Nissle 1917 is supposed to produce K2 in the gut. I’ve not read the article (you have to download the PDFs separately) but Wikipedia links to this article about it. E.coli Nissle 1917 has been very well-studied and lots of information about it in general can be found on PubMed.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC281544/
It is available as a probiotic under the brand name Mutaflor in Canada and Europe, and possibly Australia too. My understanding was that it’s not sold in the US because it’s classed as a medical food by the FDA, not as a probiotic, and it doesn’t meet the requirements for medical foods – but it was a few years ago I read that, so that might not be the current situation.
I’ve used this probiotic, including culturing it as a yoghurt, and interestingly, it eventually gave me tooth pain and irritability which improved when I started eating hard cheese and also when I started taking vitamin D. I suspect the vitamin K2 produced by the bacteria was increasing my need for calcium, in which I was deficient, but that’s only a hypothesis. Some of the symptoms seen when using the probiotics were similar to the symptoms I saw when supplementing Thorne K2.
https://www.mutaflor.com/index.html
I talked about this with someone recently; I do think that K2 could conceivably redirect calcium away from blood in some people and perhaps contribute temporarily to hypocalcemia, and that calcium would help.
The evidence leans very much against the gut contributing to systemic K2.
Thank you, Chris!
Yes, thank you Chris for acknowledging that K2 can lower blood calcium. It just makes common sense, but especially if one isn’t getting sufficient calcium in the diet, then it will be pulled from the bones in order to obtain what the body needs.
Whenever I take D3/K2, my teeth get LOOSER.
I grew up with asthma; I suffered sinus and respiratory infections my entire life. I started smoking at 16. When I was in my early 40s, my asthma was becoming increasingly worse. I was diagnosed with COPD at age 47. I am now 55. I quit smoking four years ago. The disease does not improve. My good days were far,i was scared that i wont survive it but i was so lucky to receive a herbal products from my step father who bought it while coming from South Africa for Rugby league,this herbal remedies saved me from this disease,at first it helps fight the symptoms of diseases and i was seeing good outcome,i had to use it for 13 weeks just as they Dr was prescribed and i was totally cure of asthma and COPD, (Totalcureherbalfoundation gmailcom) do not hesitate to purchase from them they deliver across worldwide to
Ukraine & Russia Federation
New Zealand and Australia
CIS Countries
USA and Northern Americans
South American Countries
Europian Countries
Hi Chris,
With taking K2, has their been any findings that with the increase levels of K2 in the body, do cholesterol level tend to also increase? Per my last blood lipid panel, my levels were up. I recollect that I possibly read that cholesterol level increases were to be expected. Please advise of any information so that I could share with my Drs. Thank You.
I believe that this is a typo:
… One of them may be vitamin K epoxide oxidoreductase (VKOR)
Should be “vitamin K epoxide reductase.”
K2 is very hard for me to maintain as I have been diagnosed with SIGNIFICANT allergy to soy and other legumes, like chickpea. I would be very interested to further discussion on the non natto or chickpea sources of K2
As far as i know if you cannot use legumes or Soy beans there is nothing else you can use to culture Vit. k2 (MK7).
I have used Soy, Mung and Black Beans with success. I have tried to find out if just rinsing all the slime off the beans with warm water would result in obtaining K2 without ingesting the bean. So Far I have not been able to get an answer.
Chris what a fantastic post! You are incredibly meticulous! You have narrated entire content no copy paste. Interspersed with your valuable insights for example on fat soluble vitamin absorption chemistry or placement and tail size determining half life and location of absorption. Great work!
I was diagnosed with multiple sclerosis 1 month after I turned 50. My Grand-mum was 96 and had it since she was in her 20s. I was on Copaxone, the first year was daily and later I was on 40 mg, 3 times a week. It made a tremendous difference for me. Although the fatigue was what really gets to me. When I do too much, I do start to feel weak.There has been little if any progress in finding a cure or reliable treatment. My multiple sclerosis got significantly worse and unbearable because of my cognitive thinking.. Last year, i started on a natural multiple sclerosis Herbal therapy from Green House Herbal Clinic, i read a lot of positive reviews from patients who used the treatment and i immediately started on it. I had great relief with this herbal treatment. I am doing very much better now, no case of Cognitive thinking or memory Loss,, my multiple sclerosis condition is totally reversed. Visit Green House Herbal Clinic website I am thankful to nature, the medics failed. Share with friends!!
Hello Ms. Drali:
If you have MS you might want to look into a book by Dr. Steven R. Gundry, MD. It is not the easiest book to read, and he doesn’t even mention MS until about 13-14% into the book – it is called “The Plant Paradox…”.
I got it from my local library so it didn’t cost anything on my first read through – I don’t have MS but I had read it for another serious health problem. Anyway, I have read through it twice now to understand how this program works, and it looks promising. So, if you have a large library available you can probably request this book – or it was about $15 on Amazon for the Kindle version. His results are very encouraging . Still this whole idea is very controversial and there are many deniers and people who disagree with this Dr. Gundry, and these are also easy to find on the internet. Bottom line, if it works as he states (and I don’t know yet because I am new to this program) it might help some people – not sure right now, but it is an interesting read if you can find a free copy.
Probably the most successful method for improving MS is use of the Dr Coimbra Protocol which involves a trained physician giving very high doses of Vitamin D3 in the 20,000 to 100,000 IU range daily. You would need to find a doctor familiar with this in order to be fully treated. You can read the Coimbra Protocol which is posted on the web and there are doctors listed who use the treatment. Coimbra has about a 95% success rate improving MS with the vitamins D3, B2, low calcium, extra water and monitoring of parathyroid hormone levels.
If you can’t find a participating doctor, its safe to take as much as 15,000 IU of vitamin D3 daily for many people especially if they take 5000-10,000 IU of retinol vitamin A which balances the effects of vitamin D in the body. The MS is an autoimmune disease, the vitamin D3 enables the body to tell the difference between self and non-self so it stops attacking the brain and nerves.
A number of other nutrients have immune system calming properties, these are typically good against arthritis and other conditions with an auto immune component.
Hello, Thank you for your article. I wanted to ask, you show hypothetical adverse side effects to MK-4, but what about MK-7. I have read many reviews (Amazon) and elsewhere, where ppl had heart palps, and high BP after taking a MK-7 supplement and some went to the hospital. Some had headaches/neck aches. I don’t know if they had taking anything else at the same time or at what exact dose they were taking, but it wasn’t high. So just wanted to ask about MK-7 effects and do you recommend if taking this, when do you take it (time of day) and is it ok to take with any other supplements? Dr. Mercola’s MK-7 from fermented chick peas dosage is180 mcg once a day. Is that a good dosage? That you for this info!
The adverse reactions from taking MK4 are usually minimal and mild. Lots of people move to taking MK4 after finding MK7 to be problematic and have no reaction to taking MK4. The reason form this is largely that MK4 is made by the human body for its own use and its able to discard what is not needed. There are still occasional reactions to the other parts of the MK4 pills where people can be allergic or sensitive to the oils or incipients of the pills.
The MK7 form is known to have a good rate of reaction in people who are sensitive to it. This is about 10% to 20% of people. The reactions are generally increased anxiety, sleeplessness, a thumping heart beat and raised blood pressure. These typically go away within three days of stopping the MK7.
The 180 mcg dose of MK7 is fine if you are able to take MK7. Note that there is much more human clinical research that has been done with MK4 than has been done with MK7, so if you are looking for reasons of improving bone health or artery calcification, the best form to take is MK4. Accept the MK7 research as far as it goes, I find it to have brain enhancing properties but MK4 has much more success in improving bone and cardiac health.
Dear Sirs
I’m taking 25mg of k2.
Why do I need 10,000iu of Vitamin A?
The Vitamin A I see is in the form of Cod liver oil, is this the same thing for retinol?
Or can I substitute Niacin?
thanks
benny
The vitamins K2, A and niacin fill different functions. Because the different nutrients support each other, using the combination works out best.
The retinol vitamin A or retinol from cod liver oil work with the release of calcium handling proteins in the body to improve their effectiveness. This reduces rates of kidney stones and improves calcium scavenging of the arteries especially when combined with vitamin D.
The niacin is a B vitamin that improves carbohydrate metabolism which lowers the triglyceride levels that are important in causing heart disease.
HI, How does not having a large intestine, due to total colectomy, effect someone in regards to Vitamin K2 absorbtion? Thanks.
From what I’ve read, we make K2 in the colon, but it never gets absorbed, because it is too far down. So, K2 isn’t absorbed in the colon. I think that your taking it will be absorbed fine without having a colon.
Would I need to take vitamin K2 supplement if I am on a ketogenic diet consuming about 3-5 whole eggs and 2-4 chicken thighs per day. Also half a cup of spinach and same of broccoli each day. I take vitamin C supplement and my bad cholesterol is very high.
The MK4 vitamin K2 supplement would be helpful in reducing any artery calcification and it provides an increase in bone strength and health along with helping blood sugar management. After artery calcification, the big factor is triglycerides which will be reduced on the ketogenic diet.
Moderately high cholesterol is not a bad thing, but the cholesterol needs to be handled well by the body to avoid oxidized cholesterol. Basically taking 400 IU of a vitamin E containing the Gamma form will help with this. An additional standby is use of plain niacin which boosts HDL while reducing triglycerides. Read more on niacin at DoctorYourSelf.com by Dr Andrew Saul.
Good luck with the illness, sorry you got it. I used to work in the tobacco pipe business for many years in New York City. Back then, people were switching to the pipe as a step towards quitting. You don’t inhale the pipe, but you do get lots a’ smoke and it smells wonderful. You will still get clogged arteries since this is nicotine we’re talking about. I smoked about a pound of tobacco in the pipe every week. I even smoked the pipe upside down in the shower(the pipe was upside down, not me). I finally was able to quit by using 3000mg DLPA on empty stomach with water half an hour before breakfast and in the mid-afternoon. It stabilized my mood, so willpower wasn’t an issue. Best, Bob
I found out that I have chronic obstructive pulmonary disease three years ago. I quit smoking for a few days and started back up because it seems everyone around me smokes, my boyfriend, daughters, son-in-law and it makes it so hard to truly quit and yes I know I’m slowly killing myself. I’ve been a smoker for 38 years was down to three or four cigarettes a day then started smoking like crazy again. I really do want to quit just don’t have the willpower! So if you don’t smoke now don’t ever start,because if not for this herbal remedies i bought from total cure herbal foundation i believed i should av been with my tank now, it’s no fun getting this sick and trying to fight the urge not to smoke. I hurt so bad everyday, my back and my lungs. I wake myself up at night with my wheezing. I cough all the time I cant breath when I’m laying down. I use 2 different inhalers three to four times a day and also do breathing treatments at home.But i was able to get rid of this disease totally through the means of totalcureherbalfoundation @ gmail .com which i purchase from them,this herbal foundation are the only place where you can find the right herbal medicine to any diseases including COPD emphysema.
I discovered that when I eat nightshade vegetables (nearly daily and more than once a day), I get bad joint pain. Once I completely eliminated them, over 3 months time, the joint pain is gone.
In the past, I had taken 6 calcium tablets every night which helped me fall asleep, not realizing the danger of taking calcium in supplement form vs what is naturally occurring in foods.
Now I know better & have found this web site so that I take K2 daily from fermented chic peas & duck fat 1 tsp with each meal. I also liberally eat grass-fed raw butter through the day.
But now I’m questioning my making “eggshell calcium” from free range eggs, soaking them in lemon juice after grinding them. I am concerned about my calcium intake because my bone density got worse every year after menopause and I don’t drink milk (not even raw milk agrees with me real well.)
QUESTION:
Since I took too much calcium pills in the past & then also consumed a lot of nightshade vegetables over my lifetime – should I NOT be concerned with calcium any longer? (The nightshades contain Calcitriol- an extremely powerful form of Vit.D that signals the body to absorb calcium from our diet and then tends to deposit the extra calcium into the soft tissues.) My husband tends to think that I have too much calcium in the soft tissues in my body that needs to be used up for quite a while??
Thanks!
How do you know there is too much calcium in the soft tissues in your body?
Have you had a CT scan for calcium and have a high score? Or did you have a Carotid ultrasound?
These tests usually run about $150 or so where I live, but without a test score you can’t be sure of any calcium buildup.
I base my diet/exercise/supplements on these tests plus various blood tests from Life Extension, particularly during their testing discount months.
Without testing you are just guessing at your treatment options.
Thank you!
Do you know which test is better – CT Scan or Carotid ultrasound? CT scan sounds like a more serious test w/ radiation & ultrasound sounds safer for the main purpose of finding out about possible calcium deposits in soft tissues…
Although admitedly, IF the test uncovered plaque buildup & blood flow problems – that’s pretty important to know. However, wouldn’t there be other symptoms 1st or is it something that’s wise to test for preemptively?
In NJ we can’t get blood tests or scans w/o a prescription. So even if insurance didn’t cover it, it sounds affordable, BUT I would still need to convince my doctor to order one of those tests based on something other than the theory of nightshades & calcitriol.
I do have chronic headaches , so maybe the doctor could order one of those tests to see if I have blood flow issues in my carotid artery?
I am not a doctor, and none of my degrees are in any medical field, so I can’t give medical advice. I have been simply researching and can tell people what I’ve experienced, but I can’t say if my experiences are right for others.
To check your carotid arteries, your doctor will listen to them with a stethoscope. He or she will listen for a whooshing sound called a bruit. This sound may indicate changed or reduced blood flow due to plaque buildup. To find out more, your doctor may refer you tests such as the CT scan or Ultrasound.
My doctor did NOT hear a bruit in my case, and that is why I went with a CT scan. This was based on my family history of heart problems.
If your doctor doesn’t hear a bruit it may be difficult to get a referral.
Yes, the CT does involve radiation, Ultrasound does not, but CT probably gives a more accurate view of your heart vessels.
From my experience, I was one of the very early people in the US on the first statin, Mevacor, as my then doctor got me in a early clinical trial. I was on statins for over 25 years and still got a CT reading in the 300’s, so statins didn’t help me much.
Mt father was also on statins and had several heart attacks and operations, then died with a great cholesterol score and 4 vessels blockages. His CT was awful at time of first heart attack.
Here then is what works for me, and what I think is most important in my individual case.
Endothelial condition first and foremost.
Plaque buildup happens because of damage vessels, in most people it is that simple. Diabetes or metabolic syndrome, hypertension, an overload of omega-6 fats, smoking, and physical inactivity are some of the usual triggers.
I treated my high blood pressure aggressively, especially since my CT also displayed a dilation, so I don’t want a vessel blowout.
The other enemy of Endothelial Dis-function is systemic inflammation. I treat that aggressively with diet. No sugars, flour, syrups, artificial sweeteners, I only use Stevia that does not contain any dextrose type additives.
I take my K2 religiously, both MK4 and MK7 with virgin coconut oil. The only other oils I have in my house are grass fed butter and olive oil. This is to reduce the consumption of omega 6’s and their inflammatory properties. Along with the K’s I also take vitamins A and high dose D.
Finally, and I miss this, but we rarely eat out any more. Means we cook – all the time. Not fun for most people but as Jack LaLanne used to say, that best way to know what is going into your body, and he lived to his late 90’s.
You dont eat animal? No lard, tallow, bacon grease, duck fat?
I do think you are doing great from your post
While GreatDane has good advice, you could just take the MK4 vitamin K2 as a preventative. My experience is when I started on 1.3 mg of MK4 in an Ultra K with K2 complex for bone health, over 6 months there was a decided decrease in my annoying chest inflammation symptoms of 20 years duration. This was welcome and after 12-18 months the symptoms were vastly reduced. The symptoms drifted around my lung area and felt like mild a paper cut. This symptom reduction came from reducing the artery calcification in that area, so lower vitamin K2 doses of 1-5 mg will work over a longer period of time. Artery calcification is the most important predictor of future heart disease, easily beating all other factors.
In addition to this, if you have high blood pressure or endothelial blockages, have a look at taking the amino acid arginine which helps the endothelia produce nitric oxide which protects the inside of the arteries. Dr Louis Ignarro wrote a good book on this, “NO more heart disease” which gives a series of supplements known to help endothelial and artery health. In taking arginine, Co enzyme Q10, vitamin E gamma, and Alpha Lipoic acid, I was able to reduce my blood pressure by 25 points to normal.
MK-7 was the form of K2 that removes calcium from arteries, but that’s great to hear your overall health is better!
vitamin K2 supplements can provide it safer than fats and cheeses, etc., though fermented stuff is very good. I eat natto (fermented soy beans) a little each day, along with supplements. If you build up plaques in arteries, the body throws calcium at them to reinforce them. So long as you eat an atherogenic diet with high fat and cholesterol, the body will be trying to do that, and despite your K2 might not cooperate. Calcium is only a surrogate for total plaque burden, about 20-25 percent. If you lower your softer more juvenile plaques 10 percent and your calcium goes up 10 percent you’re way ahead. The body will throw in calcium to reinforce dissolving soft plaques, like when on whole plant-food diet, so the score can rise, but the overall effect is beneficial. That’s what I’ve read and heard from various sources, none of which are final, but neither is anything around diet as of now. But it does make sense to me.
Thanks for all the research and information. I have osteoporosis. I take Relentless K2 Menatetrenone in evening which I think is MK-4 and Jarrow MK-7 in morning. Do you recommend a better and maybe cheaper plan for me? Thank you for the help!!
I read that the Japanese are medically using 45mg/day of K2 in the MK4 form for osteoporosis. It is not cheap from any source I know of in that quantity, probably about 70 bucks a month from Thorne labs in the liquid drops form. They got rid of the dropper now the bottle just has a little hole that drips so slow it takes forever to get just a few drops out. It can be hacked easily, however and a dropper added to it. They recommend 15 drops 3x a day, which sounds like what the Japanese are using. If I were you, and I had the money, I’d try that since it has been tested and is being used by doctors over there, rather than experiment with cheaper things that might not work as well.
Remember, the needed quantity is 45mg, not mcg. So at 15,000 mcg/pill with Relentless Improvement K2 (that translates into 15mg) you’d need 3 of those per day spaced apart, to get your 45mg daily dose. At 32 bucks a bottle, for 90 of them, you have a month’s supply for only 32 bucks. Thorne wants about 70. Maybe they are more reliable, but who knows..Seems like you have a good solution already if the stuff you have is high quality..
Thank you so much for the help! It sounds like I either need to add two more of the Relentless a day spread out or switch to the Thorne drops if I can afford it. What do I do about he MK 7 Jarrow? Can I stop taking it? If still need MK 7 too, stay with one Jarrow a day? Can it be taken at same time as MK 4? Thank you!
Yes, you could add two more 15,000 doses for a total of 45,000 mcg (45mg) of the Relentless. That’s a dose used in Japan for osteoporosis. Should be great.
I’d stay with the MK7 till it’s gone, then re-assess. MK7 is oil soluble, so take something with fat in it, any kind that’s healthy for you. I like ground flax seeds myself, just grind em up, take a tbsp in mouth and flush down with water. Very good anti-cancer properties, worked wonders for prostate cancer patients.
Here’s how to decide how hard to hit the K2: get a coronary calcium scan. Ask the doc to refer you after you find a local place that does it for the lowest cost.
From that you’ll know if you’re seriously in need or what. Otherwise you’re guessing and could be wasting time and money, while something else would be better done. gd luck
I was hoping to find Microbiome labs Mega Quinone k2-7 reviewed but didn’t see it on the list. Any chance you could review it?? Loved your article thanks.
I am so fascinated by these articles on K2. It was enlightening and interesting to know we still have so much to learn about it. I have more ammunition to get my over weight friend to eat organic dairy and meat. I am very interested in getting the latest news and facts on K2. Also, I will start eating cheese again! Ya
Thank you
Joan
Cool! Thanks for writing this!
i tried signing up for your news letter , it kept returning me to the previous page ?
On Feb 2016 i started using the herbal formula the treatment worked incredibly for my MS condition without wasting much time before reacting on my body.
I used the TOTAL CURE HERBAL FOUNDATION MS Herbal formula for a total time period of 14 weeks,it totally reversed my Multiple Sclerosis. I had a total decline of all symptoms including vision problems, numbness and others. Sometimes, i totally forget i ever had MS.
Kindly email totalcureherbalfoundation gmail .com to start getting rid of Multiple Sclerosis (MS)
Thank you so much for your research. I’ve learned so much. Can you suggest a dose for children? Is 1 drop of the Thorne too much? I won’t give any to my breastfeeding baby but I have a 5,6 and 11 yr old. A lot of threads I’ve looked at suggest 15 drops 3 times a day!!! Also if you could suggest vitamin A and D dosage but for sure K2 please. Thank you it will help so many of us Mommas out!!
The 15 mg three times a day follows the dosing of the successful Japan trials, its the most effective method but also note that one of the trials used 1.5 mg of MK4 daily and this was still successful so dosing in the 1 mg to 5 mg range can be very helpful over longer periods.
Normally dosing considers the weight of the person, so children would get smaller doses and 1 mg or one drop per day should be enough.
For dosing of vitamin D3, other experts suggest 64 IU per pound as a typical optimal dose. For vitamin A, use the retinol form and dose 100 IU per pound. The betacarotene is conveted to vitamin A at only a 5% to 10% rate in recent research trials.
I had success with using 1.3 mg of MK4 for 12-18 months in reducing artery calcification although the Japan protocol calls for 15 mg of MK4 with three meals daily as the optimal dose. a good compromise would be 5 mg of MK4 taken once or twice a day. Its also important to take 2000 IU of vitamin D3 with this as the D3 increases production of the calcium handling proteins that MK4 works with. This combination should give the calcium scavenging you are looking for. Current vitamin D3 research calls for doses of 5000 to 10,000 IU daily to be taken.
In addition:
The artery interior surface is protected by nitric oxide, this is generated from the amino acid arginine in the body. ideally the arginine is given with 100 mg coenzyme Q10 and 100 mg Alpha Lipoic Acid as recommended by Dr Ignarro. I take 4-6 grams arginine daily.
If you take 400 IU vitamin E, see that it is the natural form and contains the gamma form of vitamin E. This form has a function of protecting the circulation and works better than straight alpha vitamin E.
I would advise taking retinol vitamin A which has been shown to increase the carboxylated and functional form of Matrix GLA Protein which is the actual molecule that does the calcium removal.
Good on success with calcium. I’ve got a lot of it, so was wondering, how much calcium reduction did you get, and how was it measured (carotid ultrasound, coronary scan, etc)?
best,
Bob
Hi Bob,
Nobody out of three doctors ever measured my artery calcification or advised me on it. There was a twenty year long history of my drifting chest with symptoms that were similar to getting paper cuts in the interior of the lungs. This was followed by an 18 month period where the symptoms decreased in a major way to nearly non-existent after I started on 1,3 mg MK4 vitamin K2. Their unexpected decrease was first noticeable at six months in. I was taking K2 for my bones so this outcome was a surprise.
What I can say is that my chest symptoms came and went in concordance with my MK4 levels as assessed in the Japan research, generally advancing when I trained hard and had higher cortisol levels, then reducing when my doctors asked me to stop running. In addition to this, they returned when I accidentally took a double dose of minerals, including calcium for a few months then left when this was stopped.
Since calcification is know to be an accurate predictor of future heart disease, I would recommend getting it monitored and taking MK4 as a preventative measure since it can work well.
Thanks, David. Sounds great, I wish someone were taking all the results into one database for hypothesis-generation and proof of principle. I am taking K2 mk4 daily in 25-50mg amounts plus a few drops inbetween doses. I have not yet rechecked my calcium score. It was 579 almost 2 years ago. I have zero symptoms and good exercise ability at age 71. I think I will try to get a carotid artery ultrasound instead of the calcium scan, since there’s no radiation and it’s the same price, 99 bucks. It will also show soft plaques as well as calcium. I do know this: whatever I’m doing is working, my erections have come back about 50 percent strong, after 10-15 years of none, and this is without ED meds. The meds had stopped working for me a few years back, which means that my nitric oxide levels dropped too low. They only work if you have nitric oxide in your arteries when you take them, they just preserve it. It’s a great diagnostic for disaster if the pills don’t work. Best of luck, Bob
I take krill oil along with the above, but heard oils make the calcium tacky?
A Publication in 2008.
Arteriosclerosis can be Reversed, by Dr. James Howenstine
https://www.newswithviews.com/Howenstine/james67.htm
This article has a lot of good info. To me it shows that K2 can slow down atherosclerosis, something which is medically considered impossible. Or at least shows that taking it should result in less calcium build up at some point in time. I didn’t see fro his evidence that it can reversed, although I think it probably can be. I think it’s especially likely to be reversible if the diet is non-atherogenic. Eating an atherogenic diet would put strong forces to work to build more calcium than the K2 may be able to deal with, in other words. I think it should work so long as one is not just taking K2 in the presence of an atherogenic diet. One might have to make dietary adjustments that don’t promote atherosclerosis at least, if not a diet that actively fights against it.
Good news is: There should be a new study coming out from Dr. Leon Shurgers showing if K2 can actually halt or reverse calcium build. This testing should be done by now, and the results are probably being gone over by the statisticians, so in months we should have the publicized version. And that will show how much effect, if any, on coronary calcium scores is achieved by a dose of 360mcg/day of K2. The subjects will get tested at start, halfway into the study (1 year) and again at the end (2 years). Can’t wait for it!!!!
One of the problems with Howenstine and his discussion of vitamin K2 is that it is mistake ridden with a lot of common errors to reporting on vitamin K2. For example: “The primary therapy for osteoporosis in Japan has become Vitamin K2(Synergy K).” This is later reported to be the MK7 form of vitamin K2. If you look up the seven successful research trials in Japan of Vitamin K2, you find that they used the MK4 form of vitamin K2 which is the same form as made by the human body. All of the most successful trials in reducing bone breakage rates belong to MK4 research.
Its possible to find in papers by otherwise intelligent people the conflating of MK4 and MK7 results and this is a problem in trying to understand the two forms of vitamin K2.
In addition to this there is a lot of MK7 promotional literature that again claims MK4 research results as a reason to promote MK7 sales.
The only defense against this type of mistake and misdirection is to track down the references given and read the original science papers for the actual MK4 or MK7 form used and the intervention performed. Although its not perfect, the Life
Extension article does a better job of separating the results. http://www.lifeextension.com/magazine/2008/3/protecting-bone-and-arterial-health-with-vitamin-k2/Page-01
note how they state the MK4 actually does a better job of preventing bone fractures that an osteoporosis drug. Another good article is: https://nbihealth.com/mk7-hip-fractures/
A lot of what I’ve seen from researchers is measurements of the degree of carboxylation of MGP and osteocalcin, the two proteins responsible for chelating calcium away from soft tissue, and sticking it to bones. MK7 is supposed to fully carboxylate MGP at around 360mcg/day.
Nothing takes the place of interventional trials using MK7, but the mechanism is said to be MGP carboxylation, which they can test fairly easily,b so it makes sense that anything which accomplishes carboxylation, whether MK4, 5, 6, 7, 8, 9 or whatever, should have the same results. It is an inference, however, that only carboxylation is required, nothing else that strictly requires MK4.
,,also in terms of cost of vitamin K2, MK4 is a synthetic and is far cheaper to make in quantity than MK7, I think, so it makes sense to use the lowest cost form of K2, MK4.
Enjoyed you research. Have you evaluated the Swanson brand K2 ? I would be interested about your feedback.
The correct supplement for generating nitric oxide is Arginine and /or citriline. You can read about this in Dr Louis Ignarros book NO More Heart Disease which has been out for fifteen years now. This is how the body works so its well controlled and the safest method along with the other nutrients he suggests. You can likely find an updated version of this. I was able to achieve a 25 point reduction in blood pressure to a normal BP with the Arginine and several other supplements.
One of the major factors in atherosclerosis is the typical high carbohydrate diet in the West which raises triglyceride levels. Going to a low carb diet or paleo diet will help this and should give improvement when combined with higher nitric oxide levels.
The theory of old calcified arteries being safe is an out dated medical theory that has been disproved. While old calcifications are less active, they are replaced with new and less stable calcifications that continue the danger. The treatment that is needed is a combination of MK4 vitamin K2 and vitamin D3, correctly done this reverses the artery calcification over a period of 12 to 18 months. Since the level of calcification of the arteries is a major indicator of future heart attack risk, reversing calcification is vital to future health. When MK4 is allowed to work in animals and humans, artery calcification is reduced in a major way.
From Mr. David Sanders:
“The treatment that is needed is a combination of MK4 vitamin K2 and vitamin D3, correctly done”
So, correctly done? Is there a general protocol for doing this the right way? Also, does Vit. A or E fit in with this somewhere?
Thanks.
//sodium nitrite: carcinogen? no, see the book the NO solution by dr. Nathan bryan who created the Neo40 lozenges which use it as the main ingredient. The last chapter goes into the story of sodium nitrite, nitrate, etc. and how science now points to them being helpful, in fact major components of mother’s milk, as well as found in high concentrations in human saliva. Sodium nitrite may even be considered a vitamin. It is, however, toxic in all but very small amounts, milligrams, not grams. A tsp, 5 g, kills.
Thanks for the great resource!
I had one question and I apologize if it has been addressed elsewhere. I have seen mention that calcium actually stabilizes arterial plaque. If K2 removes the calcium from plaque, is it possible it is making coronary plaque less stable and people more likely to have a cardiac event.
Thanks again for all the great info
That’s something I am concerned about, also. It’s why I use other things in my own program for myself to help stabilize the plaque and remove the softer plaque. The chief of these is a whole food plant-based diet. Dr. Esselstyn reports that the diet strengthens the cap over the plaque within 3 weeks, making you heart attack proof. That’s one thing, another is nitric oxide, which I manage via dark greens and beets smoothies, plus a pinch of sodium nitrite (only a tiny pinch per glass, 100mg or less). In addition, I take L-arginine and L-citrulline in a 2:1 ratio. The nitric oxide smooths the arteries and dilates them, avoiding frictional accidents and tears of the plaque. This is the best I can do at the moment. The diet contains no animal products at all, and no oil. These things make the blood and artery walls sticky, and reduces nitric oxide. I also use exercise, which helps exercise the arteries as well as the muscles. I’m very serious about this, nothing is too much to ask to be able to avoid heart attack and stroke. It isn’t that hard to do, either, and has many other benefits. I’d doubt that K2 and D3 alone are going to work on older plaques without any support from an anti-atherogenic diet. If you keep pouring gas on the fire, water isn’t going to help much.
one more thing…I had a chat with Dr. Esselstyn a few months back, and he mentioned that calcium scores are used as a surrogate marker for plaque. They represent only 20-25 percent of total volume. As the diet reverses the softer plaque, the body throws in some calcium to help stabilize the dissolving and breaking up areas. So he expected my calcium score to go up, not down, while the plaque is in fact regressing. This would seem alarming, but it’s nothing to worry about. It makes mathematical sense, at least, that if you lose 30 percent of your soft plaque and gain 30 percent calcium, you’d be way ahead, since the soft plaque lost would quadruple or more the gain from calcium added. So we should remember it’s a small surrogate area of calcium in a much larger area of non-calcium, and not to take the rise as a bad sign. Logically, if the softer plaque keeps dropping, the total area blocked will decline until only the calcium is left, then it can melt away too without other stuff being in the way. But plaque starts with oxidized cholesterol and macrophages getting under the endothelium. It then builds up toxins, swells up the area, and calls out arterial smooth muscle cells that migrate and change their types, utlimately winding up acting as a covering over the necrotic core to keep it from getting into the bloodstream. As these altered smooth muscle cells breakdown, they leave proteins hanging around which act like a ‘matrix’ to build a bone. Hydroxyapatite (calcium plus other minerals) can then form around them in a bone-like manner. The K2 activates matrix gla protein which can prevent this, and retard further calcification. So if you take a lot of k2 and you succeed at preventing this, then you may indeed be interfering with the body’s own attempt to stabilize the plaque. So I think, if all this is so, that it’s important to have a diet and whatever other supplementation, ie, nitric oxide forming things, that will help break up soft plaques. The main thing which has shown efficacy doing that is the whole food plant-based diet with no added oils. The main thing that intereferes with migration of smooth muscle cells into the space between the endothelium and muscular layer, is nitric oxide. The main thing that takes out the foam cells (enlarge, toxic macrophages) is also nitric oxide. So I am hoping that a non-atherogenic diet plus nitric oxide supplementation will help to not just stop, but also to regress my plaque. Non-atherogenic diets exist in parts of the World in which heart disease and stroke are non-existent, and Dr. Esselstyn has simply copied these for use in his research. Nitric oxide can be boosted quite a bit with dark greens and beets taken regularly throughout the day. There’s no need for a supplement if you are able to do that. I find I can do some, but also take the supplement, which is quite effective. One such supplement is Neo40 from Humann. It’s expensive, so I go around it by using a pinch of sodium nitrite in a greens and beet smoothie. It’s quite powerful and drops blood pressure quite fast. Be careful, it is a poison in gram amounts, so be sure to read up carefully. I use only a max of 100-150mg per serving. You can test your own nitric oxide levels by using Berkely Test Strips for Nitric Oxide. Here’s a link for the 25 strip pack for 15 bucks: https://www.amazon.com/Nitric-Oxide-Test-Strips-Tube/dp/B071Z8R2XQ/ref=sr_1_4_a_it?ie=UTF8&qid=1514599114&sr=8-4&keywords=berkeley%2Btest%2Bstrips&th=1
good luck,
//sodium nitrite: carcinogen? no, see the book the NO solution by dr. Nathan bryan who created the Neo40 lozenges which use it as the main ingredient. The last chapter goes into the story of sodium nitrite, nitrate, etc. and how science now points to them being helpful, in fact major components of mother’s milk, as well as found in high concentrations in human saliva. Sodium nitrite may even be considered a vitamin. It is, however, toxic in all but very small amounts, milligrams, not grams. A tsp, 5 mg, kills.
The Nature’s Life brand MK-4 has 5000 mcg (5 mg) per pill, but even though it’s a tiny tablet, it’s easy to cut into several pieces. I have been cutting it with sharp kitchen scissors into 3 pieces, for approximately 1667 mcg (give or take) per portion. It doesn’t crumble/crush very much, so there isn’t much left-over powder (but if there is, you can just scoop it up from the clean plate you cut the tablet over and swallow it with some water.)
[You don’t have to be bound by the amounts that supplements come pre-proportioned in – there are often ways to tailor the amounts — for example, by opening a capsule and taking a portion (saving the rest for another dose), or by cutting a tablet into a specific number of equally-sized pieces.
(Some supplements do have special coatings on them to benefit their assimilation in the body, and it is advised not to open, cut, or break them, but this will often be stated on the bottle.)]
I have osteopenia, and in the past year I have searched many hours for guidance about recommended vitamin K types and intakes — sadly, the whole topic area seems to be quite muddled, whether for treatment of osteoporosis/osteopenia or general/typical nutritional considerations.
Confusions about the different types of K, conflating research on and suggested/typical amounts of MK-4 and MK-7, even mistaken attributions as to exactly which kind(s) of K is/are high in various foods, not specifying the country of origin of the cheeses and other foods tested (gouda from the Netherlands is not going to have the same nutritional profile as “gouda” from Wisconsin, say), etc.
I felt bad on K1 and also felt it wasn’t having any effect, and I didn’t like MK-7 — I didn’t have the unpleasant side effects that some people have reported, but I didn’t feel good on it.
The 1600 mcg of MK-4 I’m taking daily isn’t causing me any problems that I know of, but I don’t know if it’s helping — I can’t have another bone density test for 2 years (and anyway, that sort of test may not accurately show what MK-4 is doing for bone health).
I’m also trying to figure out how much D, A, E, magnesium, calcium, boron, strontium, silica, zinc, copper, omega-3, carbs, fats, and protein to take for optimal results (for my bones. And other areas of health.)
Also, folks with osteopenia/osteoporosis should look into eating prunes (dried plums) – some good research studies have been published which show great bone benefits from only a few prunes a day (50 grams / 5 prunes in one recent study, 100 grams / 10 prunes in the earlier study… probably even less than 50 grams would have very good benefits – the 50 gram and 100 gram results were the same, and they didn’t test less than 50 grams). Additionally, the participants did not gain weight even though they added the prunes to their existing diet and didn’t change their activity level or lifestyle in other ways, and the prunes did not cause most of the participants uncomfortable problems with loose BMs, which some folks may worry about.
And low-level bioidentical estrogen and/or progesterone can be of great benefit for the bones, depending on one’s health circumstances, age, etc.
I was under the impression Gouda bacteria injected in the process are the same in Wisconsin as in Holland. Not sure Wisconsin Gouda has any less Vitamin K2 than Dutch Gouda.
You mention that the benefits of s. Bacillus natto are available if you inoculate any vegetable. I know of studies using beans and garbanzos. Are there any low FODMAP vegetables that would work? Anything that would produce glutamate without excessive ammonia odor? Thanks for your reply
I was diagnosed with COPD & emphysema in May of this year. I have been smoke free for 14 months. I quit because my first granddaughter was going to be born! I didn’t want to smell like an ashtray when I held her! Since then I have been having trouble breathing, gained twenty pounds since quitting smoking I was exercising and not losing any weight, seeing a dietician and being told to quit eating practically! I was depressed and feeling like nothing is working! There’s got to be a way to make me feel like my chest isn’t so tight feeling like something is stuck in my chest. I lost touch with reality.I started on Health Herbal Clinic COPD Herbal formula treatment in August 2017, i read alot of positive reviews on their success rate treating COPD disease through their Herbal formula and i immediately started on the treatment. Just 7 weeks into the Herbal formula treatment I had great improvements with MY breething ,I am unbelievably back on my feet again, this is a breakthrough for all COPD Patients, visit Health Herbal Clinic official website This treatment is incredible!
This seems to have nothing to do with the subject matter of Vitamin K and to be an ad for a product on a different website.
David Sanders
My blood blood test results just came in:
total Cholesterol 255
HDL 74
LDL 166
One year ago total Cholesterol was 156.
Do I get back on statins?
Bob:
On this loaf of bread it says for one slice contains 13g of carbs. Those carbohydrates is what I was going by.
75-100 carbs daily.
JUst came across this with the use of Lipids.
https://www.graphenea.com/blogs/graphene-news/making-graphene-oxide-hemocompatible?goal=0_af7ce00477-d7c5d12697-104427029&mc_cid=d7c5d12697&mc_eid=565b17105d
Ok, thanks. That means 4 calories per gram of carbs, so you’re getting 300-400 calories from carbs if you eat 75-100 grams of carbs. That is not much calories, especially if someone exercises. So you’re getting the rest, say you need 1500 calories/day if you weighed 150 lbs, you still are eating 1100 calories per day from something, and I doubt that’s all protein. There has to be substantial amounts of fat in the diet you may not be aware of. Saturated fat (solid at room temp) will get in the liver and drive up cholesterol by stifling the cells that remove excess cholesterol from the blood, so the cholesterol builds up and your test numbers go up. If you have high test numbers is still does not mean you’ve got plaque in the arteries. The only way to know is some sort of test, the easiest of which is the carotid artery ultrasound. That non-invasively shows the plaque (or lack of it). It’s not as good as an angiogram, but they are expensive and invasive, with some risks. Good luck with it, hope I’ve given you some good info. I’m not a doctor or an expert, just a guy wanting to survive and pass along anything I think might be useful.
thanks bob
my fats –white meat Cranberry Pecan Chicken Salad–fat cal. 210, total fat 23g. sat. fat 3.5g, trans fat 0g.,Cholesterol 45mg. Eaten 3-4 times week 1/2 cup.
Olive oil 1 tbs with scrambled eggs 3-4 times week on low heat. No fried foods. Thats it for my high fats.
Guess its time to get back on topic.
I consume natto, and dislike it intensely. My task was to make the gag reflex go away. So far, I’ve been able to stand it, barely, by blending it in with dark greens and beets, plus a half tsp of vanilla extract (I use the natural stuff, it’s expensive, but I plan to consume a lot, so don’t want a chemical feast). The whole thing tastes like a vanilla egg nog, not too bad. I start by buying the highest priced natto, not the super cheap stuff. They seem to used smaller, nicer looking beans and the taste seems less aggressive in the expensive stuff. It’s only 3.50 for 3 boxes for the expensive stuff, versus about 2 or even less for the cheap stuff.
Getting K2 from supplements should be fine, but I’m impressed that the discovery of natto got a whole race of people excited about it and many still eat lots of it, despite having a wider range of things to eat. I guess you could say the same about hot dogs, but the vitamin K2 in natto has also spawned an industry, even a company called “Nattopharma”. So I wanted to include natto in my campaign to help my arteries. My diet is whole plant food based with no added oil.
bob, where you getting the Natto, at local china store. Just pick the most expensive, or is there a brand?
thanks
benny, around eastside of Seattle, we have these “Asian markets” with various names. I just go to one of them and hit the frozen food case to find it. It’s all in pictogram languages of some kind but the prices are US. I often see different brands and one or two in the top price level, so I get one of each and try it. Natto isn’t horrible tasting so much as the sticky stuff is sort of revolting. The blender takes care of that. At the checkout last time, the guy looked Swedish, and said he loved natto, ate it daily. I told him about K2 and he was floored, had no idea, he just loved eating it. !!
Keep up the good work, seems it is paying off.
I just turned 75, have no idea what my Arteries look like. My cardiologist will just give me a stress test– tells me nothing. Most likely hasn’t heard of the Homocysteine blood test since we live at the end of earth, South Texas
I’d hate to live in Texas and be on the all-plant diet I’m on! 😉 Your numbers in your other post to Sander don’t look good assuming you’re putting down plaque. You can find that out by asking for a ‘carotid artery ultrasound’ If you see plaque there, then your numbers are concerning, if not, they aren’t. But let the doc decide what to do if that’s how you’re playing it. In my world, the doc is for testing and emergencies, not for strategy. I know my arteries are lousy due to a calcium scan I had, so I’m doing the only thing that’s proven, the whole plant food diet. See the movie Forks over Knives, and or especially this youtube video: https://www.youtube.com/watch?v=m8yikz5bOEQ good luck.
Thanks bob for the reply.
Going thru my records, my last 4 years of blood test, my TC been a low of 124 to 156 of 3/7/16, and a 255 reading for 12/19/17. A big 100 point jump.
My diet hasn’t changed, low fat, 75 to 100 carbs daily. Walking 3 miles 6 days week, peddling indoor bike bout every day.
This PD this year could of caused the jump.
JUst starting k2 with mk4 and mk7,1000mcg,- 100 mcg, this hasn’t had time to work yet, I think.
I think someone made a mistake somewhere in the readings—hopefully.
sure thing, benny. mind if I ask, how do you consume only 75-100 calories from carbs (this is calories, not grams, right?) or even if it was grams, then it’s 300-400 calories from carbs on a low fat diet? That would mean you are eating huge amounts of protein. ?? What exactly do you eat to survive and get your 1500-2200 or so calories per day if not fat or carbs?
..I should add, my source for the advice about the carotid ultrasound scan comes from the movie “Fat, Sick, and Nearly Dead 2” (on netflix now). It is near the very end he is in the hospital with a well-known, award winning preventive cardiologist from Mt. Sinai in LA, Sheila Kar. She does the ultrasound for him and tells him what I told you: if you have plaque there, then watch your cholesterol, if not, don’t worry about it. The scan costs usually around 50-100 bucks and takes 5 minutes, no radiation, no shot, no fasting, etc. Easy-peasy. Once you have that, you’ve got a lens to view the numbers through, so to speak. You can check this info easily in the movie it’s only a few minutes of it to watch while she tests him and gives him advice.
oFF Post
to David Sanders;
thanks I have PD. , Just started on L-Glutathione ( reduced) and NAC
Did you know that some vit k2 pills cost 30X their weight in GOLD!!???
And yo can get loose powder Mk7 and Mk4 for just $15 per gram!!???
Find out how here>>and save a fortune>>>
https://www.amazon.com/review/create-review/ref=cm_cr_arp_d_wr_but_lft?ie=UTF8&channel=reviews-product&asin=B01GGFDVUI#
Great Article by the Way…Chris is a major genius in this area and I quote him extensively in my book about vitamin d3!!
As of the end of 2017 there are few specifics on this. While taking Vitamin D3 causes the release of additional calcium handling factors of calcitonin and Matrix GLA Proteins, I’ve not read of this being measured anywhere possibly because of the confounding factors.
In the several Japan trials, taking vitamin D3 was specified along with the MK4 but these were all 2000 IU or less, useful but less than current research recommendations of 5000 to 10,000 IU for many people. Some clinical estimates of MK4 needs have been developed for MK4 by a few physicians but those vary. The Western trials of MK4 have generally failed and one notable difference in the testing has been the use of very small vitamin D doses of 200 IU and 400 IU along with the use of bad experimental designs with inconclusive BMD testing.
Reasons for the scatter in MK4 recommendations are this. In the Japan trials, the 45 mg daily dose was found to be most effective. From what I understand, the body also uses uncarboxylated calcitonin as one of its hormonal signals, so the body actively discards MK4 at this high dosage to maintain calcitonin balance. So smaller doses in the 1 mg to 5 mg area can work well if more slowly. One Japan trial used 1.5 mg of MK4.
In my own experience, I found 1.3 mg worked well over 18 months to fully reduce my previous chest calcification symptoms. Increasing this to 6.3 mg resulted in some improved testosterone release. The popular Life Extension Super K has 1.0 mg of MK4 and this is likely a good estimate. The concept is one of replacing the missing MK4 production in the body that is caused by age or evidenced by bone loss or artery calcification; 1-2 mg daily is good for prevention and 5-10 mg is appropriate for moderate bone loss and artery calcification.
Confounders that affect calcification include adding retinol vitamin A to high doses of Vitamin D3. As shown in the Tuffs University 2009 testing reported by Masterjohn, levels of kidney stones were reduced by giving about 15,000 IU Retinol which also boosted Matrix GLA Protein effectiveness in calcium scavenging. In addition, high doses of boron are known to improve bone hardness and reduce bone loss while increasing calcitonin release and strongly reduces arthritis rates so its possible that boron levels also affect Matrix GLA Protein release. Beyond this, Requirements for replacing MK4 go up with life style when patients have high cortisol levels in nutrient restriction due to anorexia, bulimia, athletic over training, or use of steroids.
So MK4 is valuable, but there is no precise relationship to vitamin D3 intake. I suggest matching intake to symptoms or prevention starting at age over 50 years
Based on everything I’ve read, it seems that MK-4 is the superior form of Vitamin K2 for removing calcium from soft tissue and thus for cardio health. The recommended therapeutic dosage of MK-4 are quite varied. I understand that Vitamin D3 consumption increases the demand for Vitamin K2, so I would like to frame my question accordingly: What is the optimal ratio of MK-4 consumption to Vitamin D3 consumption (per day)?
Thanks for the reply.
Did some carb. counting today, My breakfast and lunch is between 35 and 45 carbs total. Dinner usually consist of 8oz. baked chicken, dinner salad, 6 pices of broccoli. Or 4 oz of tender steak with same greens. I don’t know what the carbs are in that but couldn’t be much. I was surprised that Oatmeal has 27 carbs— wow. When I have to have sugar its 100% pure organic stevia white powder.
I got to reading what kind of K2 I was taking- Healthy Orgins, k2 from natto, mk7 100mcg only. My new supply came in today from LifeExtensions Super K, K1-2600mcg, K2-1000 mcg as menaguinone mk4, and mk7,100mcg. I think the ladder is the better choise for now.
Had triple by 9 years ago, pre Diebete 8 years ago. 1Ac three months ago was 5.7 my last blood run results ought to be in this monday, can’t wait. Been walking 2.4 miles for the past 6 weeks, just upped it to 3 miles the last 3 days. Hope I can hold it. this Parkinsons is holding me back. when I miss a day or 2, legs feel like lead weights on them.
.
It’s off topic, but for Parkinson’s and PTSD there has been some success with NAC supplements.
https://www.sciencedaily.com/releases/2016/06/160616141630.htm
https://scienceofparkinsons.com/2017/07/06/glutathione-getting-the-knack-of-parkinsons-disease/
I know you say you don’t like to make recommendations, but I would like to know this; What supplements do you take? (Including brand names.) I’m sure I’m not the only one who would like to know. Thanks, Mike
Listing all the supplements I take would be a tall order and lengthy. Do you have a particular subject I could reply to?
Dear Sirs;
In the chapter Vitamin resource K2 above, Does this have anything to do with preventing or maybe reversing Arteriosclerosis. My apologizes if this is a dumb question.
Has anyone heard of the Homocysteine blood test to detect high levels of Homocysteine common cause of Arteriosclerosis?
Thanks’
‘
benny
This is not a dumb question but reversing heart disease is more complicated than just using MK4 vitamin K2. What the MK4 will help with especially if combined with levels of vitamin D3 found optimal in recent research is it removes calcium from the arteries and soft tissues. Elevated artery calcification is in some research the best predictor of heart attack risk, so this is a very important feature of MK4. Medicine has no official treatment for artery calcification.
In the larger view its important to reduce carbohydrates to only 50-100 grams per day, eliminate vegetable oils and expand consumption of natural saturated fats which help by reducing insulin production in the body. High insulin levels are shown to increase the rates of heart disease by 300% and saturated fat improves HDL cholesterol release.
Beyond this, nitric oxide production is critical for protecting the linings of the arteries and its possible to reverse atherosclerosis by improving nitric oxide release. Look up a book by Dr Louis Ignarro “NO more heart disease” and read some of the current research on arginine and nitric oxide in cardiac research.
For those in a family with a history of clotting events, its advisable to take natural vitamin E and possibly ginkgo biloba for their blood thinning properties.
I agree it’s multi-faceted to reverse heart disease. A clear case was Dr. Joe Crowe, MD from Cleveland Clinic, a colleague of Dr. Esselstyn. His left descending artery recovered fully after nearly killing him twice. The followup angiogram was pristine after being all moth-eaten. He was 45 so the plaques were likely young ones. He did a very strict whole plant food diet and exercised, and the disease was reversed in 30 months. He worked directly with Esselstyn, their offices were 3 doors apart. No statins were used, nothing but diet. I am 71 and do not hope to do the same, since the plaques will by now have not only calcium but scar tissue in place. My goal is opening up enough blood flow to have a good life and without threat of heart attack and stroke. I use two sources of nitric oxide, a strict whole plant food diet, exercise, vitamin K2 both MK4 and MK7 from two different makers, vitamin D3, natto, dark green leafy veggie and beet smoothies daily, and read constantly over the data available, watch videos on plant diet successes, etc. to keep self motivated. If I slip and eat something off-diet, I pick self up and get back in the race. It’s been good, lots of progress.
Does heat degrade the k2 in natto?
I make natto using soybeans (have tried mung and black beans also) and do not seem to digest even fermented soybeans well.
My questions are:
Is most of the K2 on the slimy outer part of the soy bean and if so can warm/hot water be used to separate the slime from the bean and consume as a liquid? Will this process leave a lot of K2 behind under the skin of the bean or inside the bean?
Where are your works cited??? I stopped reading when I read the name “Dr. Mercola.” This is a known quack doctor who pushes all these supplements for profit. Also, he’s not a practicing doctor anymore and hasn’t been for a long time. It was years ago that I figured all this out.
This article seemed interesting enough, but your section on “Is Vitamin K2 dangerous?” is the shortest section here, which increases my skepticism that began with your lack of citations. I have personal experience as someone who took K2 supplements for a while and also went out of my way to eat fermented cheeses high in it. I was vegan for years, so I thought maybe this was just the thing I needed. So I started eating too much cheese, because natto is disgusting. That led to some problems of its own (too much calcium/magnesium), but I strongly believe that the K2 also led to problems. When I cut all of these things out, my health returned to normal. My doctors, who had no idea what K2 was, thought I was crazy. I wasn’t even taking that many supplements, okay. I believe it was more than you recommend here, so I give you that credit, but there are obvious dangers from my experience. #1 was when I was freaking out about a sudden onslaught of health issues (mostly caused by eating too much cheese, but I initially thought it was the iron supplements), I went to the ER… the first thing they did was try to draw my blood. This was downright horrible. Worst experience of blood drawing ever, and I’ve had some pretty bad ones before due to dehydration (veins not big enough so they had to keep pricking me). This was pretty amazingly bad. The nurse gave up trying to take a second vial from me because the vein in my hand swelled up like a marble when he tried to do this… and it kept getting worse. It was so painful I was screaming at one point. So what happened? The nurse had no idea what was going on, but he said he had never seen anything like it before. He just did not understand. But I understood. I mentioned K2 to him, but he had no idea what it was and just mentioned K1 and its coagulating properties. As you mentioned, K2 has coagulating properties like K1. My blood was hyper-coagulating because of all that K2 in my system, to the point they couldn’t even take my blood. YIKES!
Now, there were some serious health issues I was dealing with those days, in my mid-20s…. of course the doctors though I was crazy and couldn’t be having horrible joint pains. But it was partly my fault because I didn’t wanna tell them how weird my diet was with all the cheese I was eating. I am pretty sure what happened is that calcium was getting stuck in my joints from eating excessive cheese. Once I cut the cheese (no pun intended) the joint pain mostly went away after about 3 days. However, I was also a little Vitamin D deficient and had eaten little calcium during my 5 vegan years, so this is part of why I overdid the calcium. It was also the K2. Now, it’s one thing for calcium to get stuck in your joints…. it’s another thing to have osteomalacia (sensitive bones) from Vitamin D or calcium deficiency…. and it’s QUITE another for your bones to rapidly SHRINK while you consume large quantities of calcium and Vitamin D pills. Actually, I probably wasn’t taking that many Vitamin D pills at the time. I was very confused as to which of these supplements was causing what at the time but I believe they all had different side effects.
Years later, I haven’t taken Vitamin K2 pills or consumed any special foods to obtain it since that whole health fiasco. While my joints still hurt sometimes if I take too much calcium or iron (especially together), my Vitamin D levels have stabilized at a solid mid-range…. and there are a some problems I haven’t had except during that 2-3 months of health scare 4 years ago. One being that problem with having my blood drawn – no more hyper-coagulation. Another is the hypersensitive bones from osteomalacia. The other being this weird sensation as though my bones were being chipped away from this inside of my body. I never had this feeling before or since. It’s a strange, disturbing sensation that probably makes me sound crazy to anyone who hasn’t felt it. But I felt like the side of my head, and the side of my jaw had this weird feeling as if calcium deposits were being removed from them. I did wonder if it wasn’t in fact the opposite happening since that is what I’d read that K2 is supposed to do. I also wondered if my Vitamin D wasn’t high enough yet to benefit from K2. One sign of this was that the Vitamin D really improved my move within a few hours, but if I took K2 with it (some pills come with the combination) it was as if the D was being used up too rapidly and my mood improvement was extremely brief or nonexistent.
I also felt this weird bone-removal sensation in other areas like my hips and my toes going numb when it wasn’t even that cold…. Vitamin D deficiency makes your toes go numb, so I thought it was weird since I had just started taking it. I stopped taking the K2 and this problem went away pretty quickly. I did taper off the K2 as I still hoped it was beneficial, and the strange bone sensation tapered off as well. The more I tapered it off, the more they seemed to be associated, which led to me fully quitting it. Sometimes I did question my sanity since others were doubting me, but I believe I was sane. Just because science hasn’t recorded your experience yet doesn’t mean it’s not real, it might just mean your experience is uncommon or even rare or this Vitamin hasn’t been scientifically studied much yet (fact). Most doctors don’t even know what the hell IS the Vitamin I was taking, so THEY’RE the ones whose credibility should be questioned here, imo, not me. It’s hard for me to say if my jaw or skull actually shrank from K2, but I have a few pieces of evidence: 1. my shin bones are VERY thin/sharp and I’m an LMT now so I touch a lot of shin bones and few are nearly as sharp as mine, 2. my weight during this time period reached the lowest it’s ever been since I was like 13, and even when I started gaining weight again it remained lower on average than when I recall having a similar degree of fat, 3. I am pretty certain my hips visibly shrank quite a bit. My hips now have an odd-looking inward curve. I am a 28-year-old woman. While I have always had small hips for a woman, what woman’s hips curve sharply INWARD at the iliac crest? I am pretty certain this was not the case before. It makes me look funny and self-conscious when dating. The more fat I gain in the belly, the weirder it looks.
Granted, I think my bones have also thinned from years of calcium and Vitamin D deficiency, so it probably didn’t START with the K2 supplements, but this was the only period in which I felt a gnawing sensation at the edges of my bones.
I’m not saying that K2 isn’t important, but it’s not a miracle pill, nor is anything else. Most if not all dietary supplements come with side effects if you take too much… and given their large, concentrated, and unnatural nature, not to mention the human propensity to overdo it on things that work or that we are told are miracle pills – I think it’s very important to discuss the potential dangers. For me K2 supplements were not right. I will just get it from natural sources from now on. Now, maybe it was just that my body was not prepared to benefit from K2 due to my long-term Vitamin D and calcium deficiency before that…. I upped my Vitamin D a lot after that and concluded that I needed about 4-5000 IU per day to keep my mood elevated throughout the winter. I am not taking that much this winter because I think my levels are high enough that I can survive on 1200IU per day for now. But I still wouldn’t take K2 pills again. Because it could be other things… maybe genetically I am not predisposed to benefit from consuming that much K2. Or maybe it was just too much in general. All I know is I won’t do anything that I know can harm my bones so rapidly.
I also now eat meat, but not a ton, and I noticed over the past few years that when I go from eating no meat to eating some, or from eating some to eating substantially more (this also applies to eggs), my body seems to require an adjustment period. Or my brain, rather. Red meat is highest of the meats in K2. When I eat red meat for the first time in weeks, or suddenly start eating a lot more of it, it has a strong negative impact on my mood in the same way as not taking Vitamin D pills for days. Now I try to eat red meat more consistently to reduce this problem, but there was a long phasing in period for me going back to eating meat. I really believe there a strong and mysterious link between Vitamin K2 and D. There is a known link. It seems not so mysterious, though. I can’t think of any other explanation for meat affecting my mood in this way. I never noticed it before I became vegan. You’d think the protein boost would increase my mood via dopamine. Plant sources of protein seem to boost my mood. And I think meat does actually improve my mood a little sometimes once I get accustomed to eating it again. But the effect of eating eggs or chicken or pork used to be massive. I mean, I could tell you whether or not I’d really enjoy kissing my partner or not based on whether I ate chicken or eggs that day. I might kiss more intensely due to the protein boost, yet feel relatively emotionless doing so. I’d go from laughing a lot to having trouble smiling. The mind is strange and mysterious. Please know that our minds and bodies are incredibly complex and so often misunderstood…. and be careful when consuming things like vitamins in large quantities. I think the scariest thing that happened to me was taking 2-4 magnesium pills the first time I bought magnesium pills, and I found my torso going cold and a pain inside my heart that night. I thought I was about to have a heart attack at the age of 24. The reality is my body already was getting an excess of magnesium from all that cheese when I took those pills.
My advice is to avoid K2 supplements until there’s more evidence on them. The reviews on Amazon and elsewhere read like advertisements, and many of them probably are. At most take one K2 pill once in a while. Once a week at most. And if you do take it, make sure you’re already getting the RDA of calcium and Vitamin D and that your levels are WELL within the “normal” range. Eat plenty of animal products to get your K2 naturally, but don’t be a weirdo like me and eat cheese all day. Or meat, or whatever. Natural is the ideal way to go unless you have a known deficiency. Vitamin D pills are an exception as many studies have been done on it and it’s obviously something that varies based on exposure to sunlight. Nevertheless, even Vitamin D pills can have side effects. For example, taking them without calcium makes me very drowsy, just the same effect you get from lounging in the sun.
I basically just wrote an article of my own. I’m not good at blogging, otherwise I’d just make this a post on my own blog.
Is it possible the cheese, was making your blood thick and sticky?
For a small cohort, this study:
Comparison of menaquinone-4 and menaquinone-7 bioavailability in healthy women
https://nutritionj.biomedcentral.com/articles/10.1186/1475-2891-11-93
reported “…MK-7 is a better supplier for MK-4 in vivo than MK-4 itself.”
Seems like that would simplify supplementation.
?.
excellent! thanks! Bob
The problem with this statement is that there is no health outcome being tested for in the research referenced here! In addition, the 420 mcg dose of MK4 they use is small compared to doses used in actual research trials.
There were seven successful research trials run in Japan that had as an outcome the reduction in bone breakage rates in the elderly of about 80%. This is better than the results from any bone loss drug so there is no question of bio-availability. The 45 mg dose of MK4 vitamin K2 used in the Japan research was tested to verify it was most effective.
Just checking: 45mg is no typo? At what frequency?
Point taken re actual outcomes.
There were safety trials done in Japan with MK4 vitamin K2 at 45 mg per day and also 135 mg per day. These were three divided doses with meals of 15 mg and 45 mg to get the respective daily totals. No additional clotting risk was noted with the MK4 in either case in patients.
One of the successful trials showed improvement in arm bones with just 1.5 mg per day. In the trials the 45 mg dose was found to be most effective and should be combined with 2000 IU or more of vitamin D3.
Since the body in youth and health makes enough MK4 for its own use, think of MK4 as a replacement supplement, if there is severe bone loss or artery calcification, then larger amounts are needed. Many people will do well in preventing early bone loss with 1.5 mg, The 45 mg dose is for essential medical emergencies.
The doses used for MK7 are much smaller, in the 100-200 mcg range but there are experiments with higher amounts. One of the problems is that sensitive individuals can react badly to larger doses. No animal makes MK7 for its own use so the body doesn’t control it as well.
There’s a new product Vit-K product,
http://wileysfinest.com/vitamin-k2-500mg-epa-dha-per-softgel-60-softgels/
Any idea how it compares with the others (Innovix, Thorne Nested Naturals K2 )?
The product by Wiley is good but too modest for the price. The 2000 IU of vitamin D is not considered high according to recent research, a good amount is 1000 IU per 25 pounds of weight. The amount of Omega 3 oils is lower than most commercial Omega 3 pills. The amount of MK7 is OK, but most people would be better advised to take an MK4 supplement of 1000 mcg. Those who are sensitive to MK7 will not be able to take this supplement.
It would be better to buy and take the individual pills and in most cases of combination supplements like this, they are based on older views of nutrition and tend to be a marketing gimmick, not a best approach. Do research the principle concepts for yourself.
Will it reduce high bp. I need to get mine down. on meds but want to come off them.
Read my reply to framistat by : David Sander
December 4, 2017 at 5:26 pm. This should get you started on reducing blood pressure. One caution is that arginine needs to be used with caution in patients with prior clotting events. While it reduces blood pressure by generating nitric oxide in the body and building larger arteries, arginine also strengthens the immune system which can cause additional clotting as long as the original inflammation remains in the arteries. You can start with MK4 vitamin K2 in any case, it lowers inflammation by removing the calcium. High doses of vitamin E including the gamma form of vitamin E can be used to reduce blood clotting as well.
Are you still taking arginine. I have tried it before but not had any success but probably didn’t take enough. Do you think it might get me off the bp meds. how much mk4 do you take. where do you buy your argine and k2 from. thanks.
I take 4 to 6 grams of arginine a day, starting with a BP of 145/80 in 2005. I found a book by Dr Louid Ignarro, “NO more heart disease” which gives a comprehensive view of cardiac treatment, although as a 2001 book it would be good to look up more recent clinical experiences. Over several months my BP dropped to 122/72 with the several nutrients Ignarro suggests. The primaries are arginine, alpha lipoic acid, co enzyme Q10, and natural vitamin E. The main concern by Ignarro is to address endothelial health with nitric oxide and a few other interventions. As a marathon runner, my arginine needs were high, arginine is also used to build connective tissue and it was notable that a bunch of soft tissue injuries became better after adding the Arginine. My daily blood pressure dropped in a decay curve to the 122/72 BP values over several months. My running speed in training went up by 8% as well.
As a person with no clotting events, I was safe to take arginine. In the medical literature, a close reading of the confusing results in research showed that clotting problems happened in patients with prior clotting events. Since arginine is know to stimulate the immune system as well as improve nitric oxide release and contribute to connective tissue formation, the hypothesis is it enhanced local immune activity against ongoing atherosclerosis sites and this activity caused the additional clotting events. Researchers didn’t control for this factor or know to treat for the additional clotting risk. In the trial 3 of 163 patients died, all were prior cardiac patients with clotting events.
If clotting is a concern, you should talk to your doctor and consider taking gingko biloba, natural vitamin E, and turmeric to reduce clotting potential. With no cardiac disease, I had low risk of any clotting.
At the time I had unknown artery calcification which was causing alarming itching and irritation symptoms in my chest. Two doctors were unable to pinpoint a cause for the symptoms. Finally when I started on a daily 1.3 mg of MK4 vitamin K2 with 100 mcg of MK7 eight years later, my artery calcification gradually resolved over 12 months much to my delight. I had started taking the vitamin K2 for long range bone health and resolving the artery symptoms was a welcome surprise.
I suspect that neither Arginine or vitamin K2 will work if the offending diet is not corrected. Basically this should be a moderate low carbohydrate or paleo diet with 50 to 100 grams of carbs to reduce triglycerides with nutrient dense foods and avoidance of processed or heated vegetable oils. Continue to examine the broader topic for solutions as the arginine will also not help if a case of high blood pressure has some other cause.
I get my 1.3 mg MK4 from the Ultra Vitamin K with advanced K2 complex which is sold mail order by Vitacost. Note that vitamin D3 improves release of Matrix GLA Protein which does the removal of calcium in the arteries, so a 5000 IU vitamin D is also helpful. Doctors have few treatments for artery calcification and don’t look for it despite its importance in total cardiac health.
I used to use the Vitacost K2 complex, but, after repeated requests for information from Vitacost have gone unanswered. What I have repeatedly asked for is 1) where is your K2 sourced from – is it China? 2) How much K2 is Trans (active form) and how much is CIS (which is mostly useless). They won’t answer so I am assuming the possibility that 1) it is China sourced and 2) Trans level may be very poor.
OR it may be that they don’t know from batch to batch, and if so, I consider that to be unacceptable since I don’t know what I am paying for. Some China sourced K2 reportedly only has from 0% to 20% of the active TRANS form, in which case you wouldn’t be getting what you think you are paying for.
I got mine down a bit from 140/85 or so, to 110/65 or so. I used the following things to do it with:
1. plant-based whole food diet
2. arginine plus citrulline in 2:1 ratio, 3grams 12 hours apart. that’s 2grams arginine (just plain old L-arginine, not AAKG or arginine ketoglutorate or anything added. 1 gram L-citrulline, and the L-citrulline can be from Citrulline maleate for palatability. The citrulline amount is what counts so subtract the maleate from the total weight to get the amount of citrulline. I get mine from bulksupplements.com in powder form which I mix up myself and add things for flavor and nutrition, including hawthorne powder, I forget where I got it, but just a little, like 1/4 gram or less, because it’s good for the process.
3. daily lozenge of Neo40, nitric oxide generating lozenges from Humann co.
——the next part is probably not related, but in there in case….
4. two capsules of Koncentrated K per day, on in the am, one in the pm.
5. two 5000 iu of vitamin D3 per day along with the K2, once in am once in pm.
===== this is my exercise, you should probably wait till you get the above in place at least a month or more before attempting serious exercise, it can be risky.
Daily walk abt half mile, climbing about 10 or so flights of stairs in the AM.
3 days a week do weights at gym about half hour to 45 minutes.
Daily exercise bike about 20 minutes, moderate intensity, usually after meal to reduce blood sugar.
I don’t think you can use any supplements by themselves to lower blood pressure, frankly. The reason is goes up is usually diet, in particular too many animal products. If you can cut them out, the rest of the program is almost unnecessary. If you can reduce them to around 5 – 10 percent of calories that should help, in other words, no more than a pound and a half per week of meat or dairy products. It screws up blood pressure like nothing else. Unless you remove that, you may not see results from the supplement part. You can find out by simply removing them for a month and see what happens, then decide what you want to do dietwise. I found it helped me a lot, I lost 40 lbs in a year, no more acid reflux, impotence is going away, blood sugars have dropped. Just make it whole plant foods, cooked or uncooked does not matter. Whole wheat, whole veggies, fruits, not juices or extracts. Also no added oils, especially olive oil, coconut oil, but better without any oil. Try all this for a month, and see if it helps. Anything is better than just chucking a drug or even a great supplement like arginine or those nitric oxide lozenges, they can’t correct the pounding from a diet with more than just a tiny bit of animal products in it. That’s my opinion based on a lot of living with it, watching other succeed and fail, finding the science, etc. best a’ luck Bob
I should add, I’ve tried just using arginine, and just using nitric oxide lozenges, and tried just exercise and combining all of them. What really moved the mountain was having it all. You can do the same, try what you want of the list, and see if it helps. None represent really dangerous things to try. All should help some. I found that sometimes the use of all of it almost made my BP drop like a stone, one day it was 92/60 a few minutes after some weight training at the gym. So my nitric oxide levels went through the roof, and allowed serious artery dilation at those times it was needed. BP should go up with exercise to get the blood there, but should not remain up afterwards, it should drop down pretty fast. 90/60 is still in normal range, we just see it in kids, not adults. I’m 71. BP is serious stuff, and can kill you. I’d be very wary of just lowering only with drugs or only with supplements or using both drugs and supplements would probably be dangerous. The diet and the supplements I’ve listed would probably hammer it down in weeks if not months, but if doing it all with drugs could go too low. I took one med that lowered my BP while on all this so low I was stopping at green lights, and falling over when trying to stand up. Be careful if you introduce drugs along with this stuff, even the plant diet can drop it where the drug pushes too hard down. A doctor should be consulted in all of this stuff, since it is potentially life-threatening. They won’t care about the diet, because they think it won’t work, that could cause trouble, because it always does, but the supplements they might worry about, especially if you’re taking BP meds along with it. Some doctors know about the arginine study fiasco from Johns Hopkins where arginine takers began getting heart attacks and the study had to be stopped. They were using arginine-HCL, instead of pure arginine, and no citrulline with it. They used something nobody else uses in arginine therapy and got disastrous results. It then got published in the journal of the AMA, so now everyone fears to use arginine, whereas the majority of studies are positive. That’s how powerful Hopkins and the AMA are, they messed up and they are still believed.
damn, it looks like I said ‘use it all’ leaving out the diet. I didn’t get dramatic results until I used the diet along with the supplements, that is important. Whole plant food diet removed the biggest risk, by strengthening the cap over the plaque in arteries, which takes about 3 weeks on the diet. At that point the whole thing started to work very fast. With just supplements and exercising, it did not drop very much and kept going back up. With diet alone, it dropped to normal, and with both, it dropped to spectacularly low normal, extraordinary at any age low. It’s a pleasure to go and get it tested now. So don’t give up till you tried all of it together, and start with whichever part you feel you want to do, then add the next thing, is what I did. I ate lots of meat all my life, now almost none, and I’m happier. My protein levels actually went up once I gave up meat and dairy. Not from powders, just from whole plant foods like beans, potatoes, you name it. It surprised both me and my doctor, who was worried about it. I am not making a commercial here for vegans, I still eat some meat, just tiny tiny bit once in awhile. I do it to keep my BP, weight and cholesterol nice and safe, and my acid reflux down to nothing as well.
My understanding on the use of arginine from the (John Hopkins?) research with a close reading was that these were all patients with prior clotting events. Well, one thing about arginine is it also boosts activity of the immune system which is attacking the inflamed points within the arteries, so my theory is this increased activity is the cause of the additional clotting events. You need to have either no prior clotting events or take MK4 vitamin K2 for long enough to get these calcified points calmed down before starting on the arginine and possibly include high dose natural vitamin E and gingko biloba as an anti-thrombic adjunct to treatment.
I found that following Dr Louis Ignarros program in NO More Heart Disease worked well when I added 4 or 6 grams of arginine , 2 grams bed time and morning daily.
My taking 1.3 mg of MK4 vitamin K2 was really effective at reducing my chest calcification symptoms over 12 months, so it can work. I’d advise following an exercise program, paleo oriented diet, and the arginine as a complete program.
Since Dr Jorge Fletchas says that estrogen is important to forming nitric oxide and protecting the lining of the arteries, 18 mg or boron is known to raise hormone levels which would help this.
I’ve been using a pinch of pine bark to reduce clotting issues. It has a similar effect to aspirin, but without the bleeding risks.
I have incorporated an Esselstyn-oriented diet instead of other diets since he has good human trials on it for heart disease. I say ‘good’ meaning long-term hard endpoints like heart attacks, strokes and deaths, not just soft points like blood pressure, cholesterol, etc. He also did some before/after angiograms showing good results in significant numbers of patients. His first study had only 24 heart disease patients, 18 of whom completed the period of dieting. Of those there were no recurrences. Of the other 6, they had severe recurrences with 2 deaths. His second study had 200, of which 180 completed the dietary period. Of the 180 only one had a recurrence, and it was debatable if he actually followed the diet. The rest had no heart attacks, strokes, or deaths. So he got very close to 100 percent results. Of the 20 who fell off the diet, 66 percent had further heart attacks, strokes, and deaths. I had to use this diet due to the lack of studies of hard endpoints using other diets that come close to this good.
I normally don’t like to repeat the same comment others have already made, but in this case I feel compelled to . . . thanks for your AWESOME Vitamin K resourse.
I have a background in chemistry and am wondering if you can provide a resourse for how to synthesize MK-4. Also because I live in Chile and gouda cheese is very cheap and readily availble here, I’m interested in possibly extracting MK-4 from gouda as an alternative to synthesis.
I’ve already experimented with drying out gouda cheese and observed it loses about 10% of its weight and leaves an oily residue, which I guess is where the Vitamin K2 is.
Thanks again for your great work. Keep it up!
The MK4 sold is synthesized at a plant in Japan. They produce all the MK4 vitamin K2 in the market as extraction is more costly than synthesis. Any of the Japan trials with MK4 would list them as a source.
Hello. I am an unfortunate recipient of 5 stents in my LAD arterie, but thats another story..
Trying to lessen to “diffuse disease” marker put there on my head by the medical community- dont need any more stents. Can you recommend any good MK4 supplements? I saw your MK7 recommendations but not the MK4, which I believe would be the way to go for arterial plaque shrinkage?
thanks
Thorne labs offers a very exensive but very concentrated solution of MK4, with about 1mg/drop. Last time I bought it was 60 bucks for about 30 ML. It lasts pretty long if you take 15drops/day.
Thing is, the expert, Dr. Leon Shurgers isn’t even bothering with MK4 in his research anymore, but uses MK7. Not that I would think he is the only source, but I would NOT skip MK7 in favor of an all or nothing MK4 regimen. I’m using both. I get MK4 from Koncentrated K, The Koncentrated K capsule has 25 mg of MK-4, 0.5 mg of MK-7, 5 mg of K1 and 2 mg of Astaxanthin, at a cost of $45/60 capsules. If you take 2 capsules/day, you get 50mg of MK-4/day (more than the 45/day recommended) plus 1000 IU of MK-7 (equal or greater than one packet of natto), plus the rest. You could take only one/day and get a great amount of K for only 22.50/month, or get a super dose for 45/month. If you still want extra MK-4, I suppose you could take some drops of Thorne MK4 liquid during the day, since MK4 has a short half-life?
Hi, my mom who is 93 has been taking Puritans Pride K2 50 mcg. She had angioplasties 20 yrs ago. She takes statins, COq 10 400 mg , fish oil 2000mg , aspirin etc. for a long time. Now at this age she has now developed higher blood pressure than before probably from arteries getting narrower. My question is that if she ups her dosage of K2 to 100mcg will it help her, without side effects. Thanks.
There is NO BENEFIT from taking statins for the elderly: http://www.mdedge.com/ecardiologynews/article/138907/preventive-care/statins-no-benefit-primary-prevention-elderly
If she tapers off the statins, she can reduce her dose of CoQ10, which should be split: https://www.drsinatra.com/what-is-the-best-form-of-coq10-to-take
Has her Vitamin D level been checked? Is she taking a good multivitamin, eg Life Extension Two Per Day?
What is her hsCRP? Homocysteine?
What is her diet like? Low or high carb? Good or bad fats? Processed or whole foods?
From my experience, the use of MK4 vitamin K2 is preferred over the MK7 form; your 100 mcg dose indicates this is MK7. The MK4 form actually is used in more places in the body. When taken with extra vitamin D3, of at least 2000 IU but 1000-1500 IU per 25 pounds is a good dose for D3, the calcium scavenging process in arteries is improved and this is a major help for heart conditions.
In addition, have a look at use of the amino acid arginine. When I followed Louis Ignarros book “NO more heart disease” and added 4-6 grams of arginine daily, my blood pressure dropped by 25 points over five months to normal. You might look up his book and review newer references on clinical use of arginine as the amounts of alpha lipoic acid, coenzyme Q10, and gamma vitamin E have increased since the book’s 2001 publication date.
Statin use is very conflicted, for one thing there are reports that higher cholesterol levels lead to improved survival rates in recent research. Cholesterol, saturated fats, monounsaturated fats, and salt have been given clean bills for health in research! Its important to improve insulin sensitivity and reduce insulin levels to reduce triglycerides, primarily by reducing carbohydrates to 50-100 grams per day.
additional work in Germany shows a 3 gram dose, every 12 hours, in ratio of 2:1 arginine to citrulline (L-arginine to L-citrulline) gets the blood levels the highest in 24 hour period. Taking 3 doses 8 hours apart doubles the effect. The L-arinine must be pure, not compounded. The L-citrulline can be in form Citrulline maleate for palatability, but the citrulline still should be one half the arginine by weight. Dr. RAiner Boger did the dosing tritation research, he is head of pharmacology studies in U of Hamburg. The lowering of carbs as you said will result in instant improvement but long-term damage as calories from fat have damaging effects that take awhile to come in. Using whole plant food carbs has shown better solution, in my personal experience, it lowered net blood sugar by lowering insulin resistance several fold. Insulin resistance is just storing fat in places it is not designed to be stored in, like muscle cells, organs, etc.
Hi Chris, I have taken Coumadin for approx. 20 years now for an artificial heart valve. Recently I found out that I have a calcium build up in my veins, I attribute this to the Coumadin. Can you help me with a K2 recommendation or literature that will help me decide the optimal direction to take?
Probably you want to look up the use of high dose vitamin E, including the gamma form as a way of reducing blood clotting rates as a substitute to use of warfarin. As you seem to know, warfarin reduces all vitamin K & K2 functions in the body, creating a tendency for calcified arteries. Talk to your pharmacist about replacing the warferin and look up the clinical experience with vitamin E so you can work with the doctor on this. The doctor may want a specific treatment protocol for the use of vitamin E.
Taking the MK4 vitamin K2 will generally reverse artery calcification given reasonable health, its noted that high cortisol levels, steroid use, and various forms of starvation and over stress can also drive artery calcification. The K2 should be taken with adequate doses of vitamin D3 which boosts production of calcium handling proteins, including those that scavenge calcium. Taking a 5000 IU of retinol dose is also known to boost Matrix GLA Protein production, providing added control of calcium.
Dosing of MK4 vitamin K2 ranges from 1 mg daily for prevention to 5 or 10 mg for more serious conditions. If your condition is very serious, take the full 15 mg of K2 three times a day as is in the Japan research protocol for MK4 vitaminK2. The 45 mg per day dose was found most effective in their research trials.
Hi Chris, I am wondering if you have a recommendation for kids on dosage and brand? I’d like to use a liquid since they can’t swallow pills. Thanks for your time!
Hi: I any form of Vitamin K safe to take for a typical Polycythemia Vera or Essential Thrombocythemia patient or a patient with elevated platelets constantly?????
Great info very interesting to read. I am taking D3 but no k2 as I am on riveroxaban,will calcium build up for not taking it. Question 2,if I am able to take k2 would this help neuropathy. Thank you Chris.
Calcium build up happens due to age over 40, underproduction of MK4 vitamin K2 by the body or conditions that interfere with calcium scavenging chemistry such as anorexia, steroids or cortisol boosting stress or extreme athletic training or medical bed rest. This is normally observed by arrival of bone loss or artery calcification symptoms. Having a low intake of retinol vitamin A also contributes to reduced calcium scavenging and some references recognize low vitamin A as the cause of kidney stones. In medicine no instances of kidney stones due to vitamin D supplements have been observed at under 30,000 IU of D3 daily. Research trials with 15,000 IU of vitamin D3 have observed no side effects. So calcification only due to taking vitamin D3 is unlikely, it is more often due to age or condition.
Riveroxiban does not appear to be a warfarin path blood thinner, so taking vitamins K1 and K2 with it should have minimal or no effect. Check with your pharmacist on taking vitamin K with Riveroxiban.
The MK4 vitamin K2 may help your neuropathy if it is due to a mitochrondia condition that MK4 improves or low myelination of the nerves due to reduced MK4.
Hi David, many thanks for your expertise with your reply to my email. I will visit my chemist to see what their answer is. I will keep in touch. Many thanks Eileen.
The use of MK4 vitamin K2 will gradually reduce the calcification over 12-18 months when combined with 1000 IU of vitamin D3 per 25 pounds of weight. Typical doses are 5 mg MK4 one or two times a day with fat and meals. Vitamin K2 has been approved as an adjunct to cardiac treatment and bone loss since 1995 in Japan. The MK4 dose should be higher if you have more symptoms of calcification or bone loss. Removal of the artery blockages happens microscopically with diet changes.
To reduce your levels of artery fat blockage, reduce the intake of carbohydrates to 50 to 100 grams per day. Also reduce intake of sugar and fructose sweeteners as much as possible, fructose makes the dense, small LDL particles that are dangerous. Avoid starchy vegetables and wheat. Look up a low carb or paleo diet. This will reduce the triglycerides in the blood. Some also take plain niacin to reduce triglycerides. There is a full description of niacin use at DoctorYourself.com
Vitamin E in its natural form with the gamma tocopherol both reduces cholesterol oxidation and in doses of 400 IU or more reduces blood clotting as shown in research if clotting is a concern. There is a larger group of nutrients suggested by Dr Louis Ignarro in his “NO More Heart Disease” book which helped normalize my blood pressure.
Its OK to have saturated fats, protein, salt, cholesterol and avoid vegetable oils in your diet. The omega-6 vegetable oils are known to raise inflammation. Use of omega-3 fish oils, turmeric, grape seed extract, and ginger are known to reduce inflammation.
Have a look at track your plaque for an alternate view. I have been reading that the saturated fats actually are not dangerous for the heart, but the rest of this topic are addressed here:
http://livinlavidalowcarb.com/blog/davis-wanna-cut-plaque-in-your-arteries-slash-your-carbohydrates/2008
In recent testing research found that keeping insulin levels low resulted in fewer heart attacks, so its more important to reduce the glucose and carbohydrates that drive insulin release; high insulin levels boost heart attacks by 300%. It is important to raise your insulin sensitivity by dating the right diet and foods.
This should get you a great start!
I’m a bit concerned about the idea that taking vitamin K2, especially large doses of it, alone or with other vitamins such as D3, A, etc is going to help with heart disease and stroke.
It would seem that removing the plaque would proceed safely enough, without big chunks breaking up, but even if it is slowly melted away, and it ultimately does remove calcium from plaque deposits, and lowers the coronary calcium score, then what?
Calcium is used by the body to stabilize soft plaques against rupture. If nothing is done to remove the soft plaques at the same time as removing the calcium support system, those plaques can burst open and cause clots that can cause heart attack, stroke, and other damage.
I believe in covering bases. I have the high score 579. I’m taking K2 and D3 but also a bunch of things in addition to the main one: a whole food plant-based diet. This is known to halt plaque accumulation and in many cases to reverse it.
Calcium is only a surrogate marker for total plaque, representing 20-25 percent of the volume. Removing 20 percent of soft plaque is like removing 80 percent of calcium in terms of the amount of blockage alleviated. If soft plaque can be reduced, then the body may allow the calcium to be removed, but maybe it won’t allow calcium to be removed if it jeopardizes its plan to stabilize the dangerous soft plaque?
Thanks for your great info here! Do you have any recommendations for a liquid with MK-7? My kids and I have taken the MK-4 one you recommended from Thorne Labs for several years, but wondered if there was a good one with both kinds. Thanks!
I find the Ultra Vitamin K with Advanced K2 Complex, available from Vitacost.com to be a good starting combination. This has 1.3 mg of MK4 and 100 mcg of MK7. Life Extension makes a similar 1.0 mg MK4 and 200 mcg MK7. Be alert for possible sensitivity to the MK7 if you have not taken MK7 before. These symptoms are generally anxiety, sleeplessness, and a thumping heart beat and arrive 1 to 3 days after starting on the MK7.
Is there anyone on this forum who has an actual Calcium Score from both before and after K2 treatment? If so, what were the 2 scores, and if there was improvement how long did it take and what type K2 did you use? Also what strength was your K2?
There seem to be no direct experiments using the calcium score, but all of the research draws a circle around MK4 vitamin K2 being effective for reducing artery calcification. Most interesting are early animal experiments where giving warfarin to newborn rat pups to stop their internal MK4 production resulted in the rats dying at two months of age of burst, calcified arteries, about 10% of their life span! The research trials in Japan also noted this improvement with use of MK4 and MK4 has been allowed as an adjunct treatment for heart disease in Japan since 1995. Since MK4 is native to the body and has the right chemistry, it should work best for these purposes. There is research with the Calcium Score here using MK7 vitamin K2 made by bacteria here:
http://www.lifeextension.com/Magazine/2016/11/Vitamin-K2/Page-01
Even giving regular vitamin K1 which allows most people to boost their native MK4 production has been shown to work for slowing CAC here:
http://ajcn.nutrition.org/content/89/6/1799.full
For me, by taking a 1.3 mg dose of MK4 vitamin K2 daily, I was able to reverse a very annoying set of symptoms related to artery calcification in my chest over 15 months. These symptoms resumed when I accidentally started taking a double dose of calcium and disappeared when I found and stopped the extra calcium. Its clear that MK4 has a major affect at making the Matrix GLA proteins in the body work at scavenging calcium. MK7 appears to be partly effective at this too.
A full review of this is requires adding vitamin D3 since this boosts production of the Matrix GLA that works with MK4 and MK7. In addition, include some Retinol Vitamin A from cod liver oil or other source. In a 2009 Tuffs University study, adding Retinol to patients on high dose treatment with Vitamin D for cancer resulted in their production of MGP (a term for Matrix GLA Protein) improve, reducing their kidney stone levels and improving calcium scavenging.
Thanks for this info! It appears the studies all use fairly weak levels of vitamin K2 and got weak results. The Polish study concluded : CACS was slightly lower in the K+D group than in the D group (ΔCACS, 58.1 ±106.5 AU vs 74.4 ±127.1 AU, P = 0.7). In the K+D group, a significant decrease in the level of dp-ucMGP and total OC was observed.
CONCLUSIONS:
A 270-day course of vitamin K2 administration in patients with CKD stages 3-5 may reduce the progression of atherosclerosis, but does not significantly affect the progression of calcification.
In the other reference they found slight reduction in calcification in the carotid tests.
It’s not encouraging enough to spur a lot of interest, evidently, and we have few studies going on now about K2. I personally think it can help and maybe greatly, but requires a lot of other interventions such as diet, exercise, possibly medications, in order to work. There seems to be too many body safeguards in place that react against the rapid removal of calcium. It may be the calcium is supporting stability of dangerous softer plaques so they don’t cause ruptures and spread toxins into blood causing clots, etc. I’m still taking K2 and will continue to do so. It also may be that the right therapeutic levels of K2 have not yet been used in calcification testing. What the research so far seems to say to me, at least, is whatever these subjects are doing to themselves is not just a lack of K2 or some combination of vitamins or MGP, etc, but a formidably damaging diet, or other factors driving calcifications, so the cause is still active and overpowering the attempts at vitamin therapy. I’d love to see a study using people on whole food, low fat plant based diets for heart disease along with K2 and nitric oxide supplementations. NO deficient arteries will accumulate plaque and fail to function normally, no matter what, and this alone could undermine the K2 therapy. Endothelial dysfunction can result from certain dietary irritants, too, and introduce injury that results ultimately in calcified plaques. Exercise over a bad diet can cause more harm than good, as well. All those factors are not dealt with in these single-variable interverntions, unfortunately.
I have no problem eating Natto, in fact I like it. It is bought frozen in Asian stores. If you microwave it to defrost and warm the natto up, does this damage the vitamin K2?
On your “Updates to …” you list Green Pasture X-Factor Butter Oil as a source of vitamin K-2 added to the data base and comment that the product is fermented and contains “an unidentified set of quinones in the oil, which could upon further testing be shown to have additional vitamin K activity.”
http://www.greenpasture.org/public/products/concentratedbutteroil/
After examination of the Green Pasture website, I see there is no mention of fermentation for butter oil, but only a report that the product is “concentrated. ” In fact the owner, David Wetzel filed a patent for preparation of the butter oil which states it is heated to high temperatures. Also in an expose, Hook, Line and Stinker, the author learned that the butter came from Argentina, a claim that Mr. Wetzel did not dispute so whether it came from green grass as it states we don’t know. . Dr. Daniel also tested the butter oil with Vita K in Netherlands for all the menaquinones and possible CoQ 10 (ubinquinone). Presence of other MK’s would indicate bacterial contamination. There was no CoQ10 and some rancidity in the product at that time.
Maybe you are thinking of the Green Pasture fermented cod liver oil?
wondering if you had any comments on Bacillus subtilis? I have been hearing that it can be a major player in the intestinal bacteria by being co-factor with other beneficial microbiome bacteria. See :https://www.youtube.com/watch?v=MT6SdTUeJLc
Also – I make my own natto but do not like soybeans. Is the MK-7 primarily in the slime on the beans? Can I swish the beans in warm water or broth and just drink this with a meal or add some palm oil (vit A) or codliver oil ( A and D)? You say MK-7 is sensitive to heat – is there a range like 110 to 140 degrees?
And finally – one of the main reasons I take MK-7 and MK-4 is to help dissolve osteocytes. I have a cervical spinal canal stenosis (congenital) and have already had a corpectomy to make more space. Sounds like MK-4 is very important for this process. Any sugestions on dosage and best sources?
K2 vs coronary calcium score. The calcium scans tend to get worse despite efforts at reduction of plaques such as whole food plant-based diets and other things like vitamin K2. However, Dr. Wm Castelli (Framingham Heart study) says that the soft plaque breakup is occurring and the body pitches in by throwing calcium at it to help stabilize it. Not to worry, calcium is only 20 percent or so of plaque volume, while soft plaque is much bigger, so a 10 percent reduction in soft plaque will be greater benefit than a 10 percent calcium increase. At some point when all soft plaque is gone, then perhaps some calcium will also start to dissolve away. Make sense?
All of the papers and research I look at says that taking Mk4 vitamin K2 with vitamin D reduces artery calcification. It should be similar for MK7 as well.
I have not found ANY research in humans showing actual reductions in calcium scores. I’d greatly appreciate some links. I’ve only heard vague stories about how some patients showed some reduction, but not if it was significant statistically, or how many out of how many, etc. I’m hoping for Dr. Shurgers’ study results with MK-7! Have you got any links? Please post. I am taking Koncentrated K, a product having 500 units mk-7, and about 1 mg mk-4 in a single capsule, daily. Have not noticed anything in overall health and have not got calcium scan repeated, would rather avoid the radiation, especially if the score is just going to go up. Thanks for your excellent posts.
Have a look at : http://www.lifeextension.com/Magazine/2016/11/Vitamin-K2/Page-01
Note that even giving regular vitamin K1 which allows most people to boost their native MK4 production and has been shown to work for slowing CAC here:
http://ajcn.nutrition.org/content/89/6/1799.full
For full text on this see my reply to Mike on November 15, 2017
I’d like to let you new about a new vitamin K2 product (vK2) IT contains pharmaceutical grade MK4 (5mg) + MK7 (100mcg) available at http://www. v-k2.com
Hi C, good info tks, how did you determine what kind of fats help to shuttle the K2?
warmest regards, dR
With doses higher than 50 mpg/day K2 MK7 per day I experience an increase in arrhythmia (primarily Premature Ventricular Contractions PVCs). What are some possible explanations? Could the K2 be liberating calcium to levels that cause an excitation in the heart’s conductive calcium channel? If so, could one expect this relationship between PVCs and K2 to decrease over time as K2 decreases calcium in cardiovascular plaque?
Hi J,
“With doses higher than 50 mpg/day K2 MK7 per day I experience an increase in arrhythmia”
Its one theory that taking a lower dose of vitamin K2 may allow the calcium levels to normalize over some months until the side effects are reduced. You would have to try that and see if it works out.
One other idea is to try taking an added 200-400 mg of magnesium. This often improves the action of the heart and relaxes the nerves. Separate from this, 500-1000 mcg of chromium is known to shorten the Q period of the heart if this would be of help. My maximum heart rate went up by 15% when I started on 1000 mcg of chromium.
Thanks David. I am taking the supplemental magnesium. But I had to quit taking the K2. It was causing extreme arrhythmia. I eat a diet extremely rich in vitamin K foods and wonder if I was somehow creating an imbalance by adding the K2 MK7. I plotted the arrhythmia as a function of time, assuming a 2 (and then a 3) day half life and the extreme arrhythmia definitely is related to K2 MK7 supplementation. So it appears that K2 supplementation is not for me at the doses that most people on this forum are using. Maybe lower doses.
Hi J,
Your experience with being sensitive to MK7 vitamin K2 is typical. While most are not sensitive, the symptoms are anxiety, sleeplessness, thumping heart beat, raised blood pressure and cardiac PVC’s.
If you can find an MK4 only supplement, these rarely cause any reaction and the MK4 vitamin K2 is what the body makes for its own use. Dosage of MK4 is usually 1 mg for prevention and up to 5-10 mg for treating more serious conditions of bone loss, artery calcification, and a few other conditions. Higher doses than this were used in several research trials and safety trials in Japan with few side effects. Carlton makes a 5 mg pill and Thorne makes a liquid MK4.
Hi, Chris,
Thanks for the comprehensive resource. After trying to read it a few times, I still have this reservation (sorry if you’ve addressed this and I’ve not caught it):
You say the following: “MKs 7-9 would best reach liver and bone, and MK-4 would best reach most other tissues.” “MK-4 is unique among the K vitamins in its regulation of gene expression.” “I do not consider this study to offer any clear insight about the optimal dose of MK-4.” “[T]he lion’s share of benefit [of MK-7] came from 180 μg.” “200 μg/d is the optimal dose [of K2].”
It seems that based on the MK-7 studies, you’re suggesting a dose of overall K2. (Your supplements suggestions refer to averaging intake to 200 mcg/d regardless of the subform(s) present.) How are you making this extrapolation? I would think that we want either:
a) 100-200 mcg/d of MK-7, and we can’t yet recommend a dose of MK-4 (b/c one hasn’t been well-established)
or, b) 100-200/mcg/d of MK-7, and some separate recommended dose of MK-4 (e.g., up to 600 mcg/d [Nakamura 2014]; to benefit from the different targets/functions of MK-4 compared to MK-7).
So I don’t get how you’re recommending the mixes (e.g., your recommended Innovix K2 would provide only 33 mg of MK-7, plus some MK-4) or straight MK-4, when you seem to be saying that only from the research on MK-7 can we draw conclusions.
Hopefully that question makes sense. Thanks again for putting this together; I’d been taking Jarrow’s K-Right (they seemed to share my understanding of evaluating the doses individually: one pill = 1500mcg MK-4 (matches the Sato 2012 paper) + 180mcg MK-7 (matches the MK-7 papers you cited) + 500mcg K1 (for any K1 benefits, I guess)), but I’ve stopped now that I read the updated 600 mcg/d MK-4 figure here.
There is a lot of confusion and speculation over dosing with MK4 and MK7. What should be observed are the actual health results, not any blood level. Since the body has its own native production of MK4, the concept is to replace the loss of MK4 production happening with age or medical condition so that normal metabolism can happen. There were 13 separate research trials in Japan done with MK4 as well as safety tests at 135 mg per day. They found the 45 mg/day the most effective dose for improvement. There was also a test where a 1.5 mg dose of MK4 was effective at raising the BMD of elderly patients. It appears that the body tightly controls its uncarboxylated calcitonin levels and uses this in glucose control, so I’ve read that the excess MK4 is cut up and discarded to control these calcitonin levels. In my own experience I found that a 1.3 mg dose of MK4 with 0.1 mg of MK7 was effective over 12 months at reducing my artery calcification.
Other lower doses of vitamin K2 may be specified from European research based on diet where lower doses of MK4/MK7 from food resulted in a 30% reduction in heart disease. This is likely the basis of 100 mcg to 500 mcg doses for MK4 and MK7. Its useful if the higher doses can’t be taken.
One problem with MK7 is possible sensitivity, even a dose of 50 mcg can set this off giving those people anxiety, sleeplessness, a thumping heart beat, and raised blood pressure. Natto has 800 to 1100 mcg per serving and I read of one case where a sensitive person was awake for days after experimenting with eating three ounces of natto. MK7 is not normal to the body, so it doesn’t work as well as MK4 does. Reports on the higher forms of MKx as MK8 and above find that these tend to accumulate in the liver and have not appeared functional.
A number of the promotional arguments for MK7 actually track back to MK4 research and some authors mistakenly conflate the two vitamin K2 forms to be equal.
On innovix labs full spectrum k2 you said; from the old ultimate vitamin k2 resource.
“The MK-7 appears to be synthetic but bioidentical”
“Both forms of K2 in this product appear to be synthetic but bioidentical.”
“It contains caramel coloring derived from non-GMO corn, a potential source of allergens”
Innovix lists no dairy, eggs, corn, fish, shellfish, tree nuts, peanuts, wheat/gluten, soy, sugar, GMO, yeast, artificial colors or flavors. Soy-free Vitamin K2. Major allergen-free. Plant based K2.
I’m just curious as to where you got the info before the revision of this article.
I was diagnosed of Chronic Obstructive Pulmonary Disease (COPD) in 2012 at the age of 63. I had been a heavy smoker, my symptoms started out with dry cough and shortness of breath, i ended up in the hospital, on a ventilator. I should have known it was coming, but like most smokers, thought it would never happen to me. My COPD got significantly worse and unbearable because of my difficulty catching breath. Last year, i started on a natural COPD Herbal therapy from NewLife Herbal Clinic, i read a lot of positive reviews from patients who used the treatment and i immediately started on it. I had great relief with this herbal treatment. I breath fine now, no case of shortness of breath or chest tightness since treatment. Visit NewLife Herbal Clinic website ww w. newlifeherbalclinic. com. This COPD treatment is a miracle!!
Like David has mentioned the MK7 can cause an issue. This is reversed very quickly upon ceasing the supplement. I do wonder if there is a genetic involvement in this reaction. We are a family of 6 and all experience the MK7 the same way. Thus we all use MK4 drops from Thorne. This is a great alternative for us and works well. We’ve all got pretty sensational teeth and I’m hoping arteries!
Chris, if you had to choose between the Full Spectrum by Innovix and the MK-4 by Thorne, which would you pick?
The answer is it depends. If this is for a person who is sensitive to the MK7 form of vitamin K2, they will get anxiety, sleeplessness, and a thumping heart beat with increased blood pressure from taking the MK7. In this case its best to avoid the MK7 and take an MK4 only vitamin K2 like Thorne or Carlson 5 mg, my guess being this is 5% to 15% of people. If you are not sensitive, its fine to take the MK4 + MK7 forms, look for one having 1 mg (this is 1000 mcg) or more of the MK4 and 100-200 mcg of MK7.
I also suffer these symptoms at higher doses of K2 no matter what form I use. Could the mechanism be K2 liberating calcium from the cardiovascular system into the bloodstream, causing the nervous system to go into sympathetic mode, and causing the heart’s conductive calcium channel excitation to increase, leading to the symptoms you list? If this is true, could prolonged use of K2 liberate enough calcium from arterial plaque that the symptoms could decrease over time as the calcium levels in the plaque decrease)? I have found that this has been true for me so far. Because of this decrease over time, I have been able to slowly increase my K2 dose. But there is no way I would currently dare use the doses suggested in the article.
Hi J,
This is an interesting theory, if it could be verified it would be an interesting path for treatment. I’m starting to hear more people have the sensitivity side effects of MK7 but report this happening with MK4 which is hard to explain given the lack of side effects in several well done research trials with MK4.
If you continue to notice a reduction in symptoms over six months or a year, update us with the good news, it may mean that people can use minimal doses to start treatment and advance to larger doses later.
Excellent info, but I’m hoping you can answer one question that I haven’t seen addressed anywhere. My hubby had a heart transplant one year ago. He was diagnosed with osteopenia and prescribed a bisphosphonate. He wasn’t comfortable with some of the side effects so I researched natural ways to increase bone density and came across Vitamin K2. His cardiologist had not heard of it and advised him against it. He just went to a dermatologist who says he should definitely be taking it. Now, we’re really confused! What I really need to know is whether it’s safe since he’s immune-suppressed and these supplements are made from a fermented food source. I know about the study out of Europe that found that heart and lung transplant patients benefitted from K2 supplementation, but I don’t know if the supplements they were given are comparable to what’s available in the U.S. If anyone has info, I would so appreciate it!
Often a doctor is going to reject anything he is not familiar with and most doctors are unfamiliar with nutrition and many vitamins.
The MK4 form of vitamin K2 has an excellent safety record and I don’t know of any way it is involved with changes to immunity that might concern his doctor. Vitamin K2 is strongly involved in bone health and calcium scavenging of the arteries, both are big health improvements for cardiac patients with bone loss, it is believed that low production of MK4 vitamin K2 in the body is the common cause for these health conditions. So the lost production of MK4 needs to be replaced with a 5 mg supplement of MK4 vitamin K2 from Carlsons, Thorne, or other supplier. It is normal to suggest taking 2000 IU to 5000 IU of vitamin D3 with the vitamin K2 as this increases production of the proteins that MK4 works with, making the MK4 more effective. In case you are worried about this vitamin D3 affecting the immune system, research shows that auto immune conditions which constitute tissue rejection are _worse_ in patients with low vitamin D levels. You can read the research results here: https://www.vitamindcouncil.org/vitamin-d-deficiency-may-be-an-independent-risk-factor-for-kidney-transplant-rejection/
Thank you so much for the info! We both take 2500 mg of D3 daily and his latest labwork showed a vit. D level of around 70, I believe. I just bought a bottle of MK-7, but you’re saying he should be taking MK-4 instead. Thanks also for the link to the article. Will read that asap!
reading your article for the second time on K2 I’m a 74 year old with many many medical problems. from heart bypass surgery 10 years ago to Parkinson’s disease just now. I give credit to K2 three months ago to can lowering my A1c from 6.1 to 5.7.
Excellent work Chris, very thorough and to the point. I always appreciate your research and consider you a go-to for further elaboration and current data. Thanks again.
Hi Chris, I was diagnosed with a 20% blockage in Arteries 3 years ago through a Doppler test and I recently got retested with 0% blockage, only difference, besides having breast implants taken out was VK2 supplement, I already eat as you recommend.
Chris – thank you for your prompt reply.
I have started doing some of your recommendations before your reply, but there may be things I am not doing correctly. Strange as this may seem, since I am 70 (so getting older as you mention), but there is a possibility I over exercise, and I hadn’t considered that.
I also see some other additions to my supplement program that are now needed.
During non summer months it takes about 7000 iu of D3 to get me into your recommended range of blood value. I take 800 mg. magnesium citrate per day, is this an acceptable form?
My calcium score was in the 300’s – I don’t take any supplemental calcium, but do use grass fed dairy products, especially cheeses.
RBC magnesium is the important number. You have to ask for it. Then you would know if you re taking enough magnesium. Im betting theres a better test for calcium numbers too. Like the TSH is pretty irrelevant for a thyroid function test.
Also raw dairy is very important and fermented is best of all. Cheese is mildly fermented. Soured cream and milk, cultured buttermilk, cultured butter, yogurt, kefir.
Your dosing recommends are interesting but I seem to be having difficulty researching what K2 dosing is effective for people with high calcium heart scores (if it actually can reduce calcium plaque at all). There were 2 Netherland small studies that apparently resulted in plaque reductions at a 180 micro dose per day but that apparently took up to 3 years to see results. There is a 360 per day study going on right now but won’t complete any time soon, and these were MK7 only.
Atherosclerosis reversal seems to be controversial, but there are some varied estimations that a high K2 intake might(?) be effective.
My understanding (which may not be correct) is that Japanese who consume 3 oz. of natto daily receive a dose in the 1100-1200 micro range MK7 and that they are usually free of plaque/heart disease and have no known side effects from that high a dose.
Do you have a different recommendation dose for people with high levels of Atherosclerosis?
Hi Mike,
When reading the research on vitamin K2, you have to look at the original research, I have found commentaries and reviews where they actually conflate results for MK4 research with MK7. The two compounds should be considered separately and some intelligent people assume they both work the same. Briefly, MK4 is part of the evolved history of all mammals so it functions well in the human body and gets around well. MK7 is made by bacteria and has a different solvency so it doesn’t work a well and is not as mobile in the body. Despite natto being a Japan cultural tradition, Japanese research used the MK4 form of vitamin K2 because it was more effective. A number of western efforts to repeat this research have not turned out well. The well done Japan research used 1000 to 2000 IU of vitamin D3 which is known to boost body production of MGP which is the calcium scavenging molecule potentiated by MK4. The Western research that gave null results has used 200 and 400 IU of vitamin D3 in the reports I’ve read, giving reduced MGP. So its clear that use of MK4 vitamin K2 requires multiple factors to be fully effective.
I rid myself of mild chest artery calcification symptoms by taking 1.3 mg of MK4 and 100 mcg of MK7 for about 12-18 months along with 2000 IU of vitamin D3. A comprehensive plan for severe artery calcification would be: Take 5 mg to 15 mg of MK4 vitamin K2 daily, use the higher dose if your condition is medically dangerous. Take 5000 IU of vitamin D3 or that dose giving a 50 ng/ml to 70 ng/ml blood level of vitamin D3. Add 5000 to 10,000 IU of RETINOL vitamin A, a report out of Tuffs University on using about 15,000 IU of Retinol vitamin A in patients receiving high doses of vitamin D for cancer showed they strongly reduced complications of kidney stones. The research also showed an improvement in MPG production for better calcium scavenging in the body. Many diets are low in magnesium which balances with calcium, so taking a 200-400 mg magnesium supplement in divided doses should help the calcium issue. Boron is also known to improve calcium metabolism by strengthening bones, reducing arthritis, and reducing kidney losses of calcium.
Look over your lifestyle for any stress inducing elements that cut MK4 production in the body. Basically these are taking steroid drugs, having a high cortisol level from over exercise or under eating as in anorexia, having diabetes, radiation, or getting older. Avoid being on warferin drugs because these interfere with vitamin K and K2 production and are a known cause of artery calcification.
Wow! I didn’t know understanding the different K’s can be so scientific and complicated. I’m still a little overwhelmed and haven’t even clicked on all the “click here” buttons yet. I have been taking Walkabout’s emu oil and am concerned that maybe I have been taking too much. I would sometimes put a little of the liquid in my mouth and let it sit there for about 10 seconds before swallowing for my teeth, don’t know now if it was a good idea – or just plain unnecessary. Also, I have been taking Juka’s red palm oil. It has vitamins A, E and natural source of CoQ10 and help lower cholesterol. Cod Liver Oil by Omega 3 Innovations. I recently had blood work done and my cholesterol levels were really high. Like almost dangerously high. My feet, ankles, legs started to swell like there was a tight band around the lower part of my legs. Now reading this I’m guessing I have been missing out on MK7. I sometimes eat sauerkraut. Raw whole milk and raw cheese. I’ve lowered my salt intake as I’m not athletic as I am in my dreams. haha. But I do use either Celtic or Himalayan salt. Thyroid (Levothyroxine 100mg) is the only meds I am on. I was about ready to order more emu oil and red palm oil, but now I’m so confused. I’m gonna keep reading more info on your site and hopefully things will start to make sense. Thank you.
Thank you very much Chris, this is by far the most comprehensive resource I came across for Vitamin K and your extensive research and hard work clearly show.
I also love your articles on WAPF, you have a gift of turning the complex scientific data into simple and easy to understand articles.
A question to all please:
Has anyone tried the Bronson Vitamin K Triple Play?
It’s has the K1, MK4 and MK7 at a decent price and ranks 10 on Amazon best sellers.
I have started eating vegan diet and wondering about my vitamin K needs not being met.
Dear Chris
Thank you so much for what you are doing, you have been a blessing to us. The only thing we can think of is the fact we are Canadians and the supplements you have on your sites are US , and some are not allowed across the border or hard to find in Canada , such as Emu oilfor internal use. Which would help with CMT a forrunner of Which my husband has.
Thank you just the same.
Hello, Dr. I have been diagnosed with osteoporosis , I am interested in hearing from you regarding K2 and its benefits of it helping to improve my bones, And some statistics on how it has worked on others,
I am seeing my Rheumatoloigst today and am bringing in this article to show him about K2, MK7. I would like to show it to my doctor.
My e-mail address:angelbeach26@gmail.com
Thankyou in advance for responding,
Sincerely,
Constance Fortier
Any thoughts on Trader Joes Vitamin K2? Supplies 100 mcg as menaquinone-4. 60 tablets were around $5
Dear Dr. Chrismaster,
Greatly appreciate your extensive coverage of K2- as a retired biochemist/immunologist, I have been following the emerging story with interest. After reading “The Calcium Paradox” I was intrigued, but a bit skeptical of the claims for K2. Your resource gives me confidence that the Rotterdam study is just a part of the evidence linking CV risk to low K2. Your emphasis on grass-fed dairy/meat/eggs needs to be more widely known- I am doing all I can to spread the word at my post retirement job selling produce and baking at farmer’s markets in MD. Am handing out first page of your article at markets.
Which farmer’s markets?
Can we have a reference to support your pictogram showing that MK7 is the source of MK-4 or, another way of saying it, MK-7 converts to MK-4. ? All the literature states that MK-4 is the only MK not created by bacterial synthesis. MK-7 is created from bacterial synthesis- B. subtilis usually. Thanks!
Aurjan, this entire resource is fully references in the sections that click open for more detailed explanations.
Hi Chris,
You don’t include goose liver pate and goose fat in your data base? Kate Rheaume-Bleue’s book lists goose liver as 369 micrograms per 3 1/2 oz from Schurgers LJ et al. 2000, and Elder et al. 2006, data base. Can you comment?
Search for “goose” and you’ll find all entries in any of those papers for goose.
Hello Chris
I have read and perused through most of this article and blog. It looks like the preference is for K2-4 over K2-7 for osteoporosis. There’s so much info here I got a bit lost and confused. Can you clarify what is best for osteoporosis and do you have references to direct me to read for use of K2-4 over 7 or with 7? I know there’s been a few new publications in the past 2 years.
Additionally my Osteoporosis Specialist I go to said there was a recent meta analysis showing that K2 supplements are not beneficial for increasing bone mineral density (BMD). She did not say which form of K2, and after 3 requests still has not shared this analysis with me. I can’t find it. Maybe you know what I am speaking about? Thank you.
The history goes something like this. In 1995 taking MK4 vitamin K2 was recognized in Japan as an adjunct for treating bone loss and heart disease. There were six separate research trials later demonstrating the use of MK4 vitamin K2, 15 mg 3x daily, on the elderly, producing a 60% to 80% reduction in bone breakage rates when given with 1000 to 2000 IU of vitamin D3. There was additionally a trial that gave just 1.5 mg of MK4 to elderly patients and this showed a BMD gain in the forearm bones. There was a research review in 2006 of the 13 trials of MK4 vitamin K2 because of the spread of results. What they found was that use of BMD measurements in MK4 testing was unreliable and not to be trusted for good results, they found bone breakage rate was the critical measurement. If you review how MK4 vitamin K2 works, it improves the micro structure of the bones and the bone’s connective tissue along with balancing the bone tear down and rebuild process. As a result, the positive aspects of MK4 vitamin K2 use are invisible in large part to BMD testing that uses xrays which do not see soft tissue changes like these. BMD tests are nearly universally used in Western medicine so most doctors only see negative results in trials with vitamin K2. In addition to this problem, doses of vitamin D need to be larger than allowed in the West in order to get the body to produce more calcitonin and MGP which are carboxylated by the MK4. Most of the Western testing uses low doses of vitamin D such as 200 IU or 400 IU, amounts which are going to produce a null result in patients in the trial from low calcitonin levels. As a result all of the western medical references are to badly done research trials that seem to have the disproving of vitamin K2 as their common result. In addition to this, I read of a group of British doctors who went to Japan to review the Japan research trial results. They could not find any fault with the research but also did not believe it either.
There is also a problem of educated people confusing vitamin K2 research results by throwing all MK4 and MK7 trials together and then finding that MK7 doesn’t work as well in testing so MK4 must not work either. I’ve traced back a lot of MK7 promotional science references and have found that they often refer to results of MK4 research!
For MK7, this has not been proven to reverse bone loss in any testing, it only slows bone loss. The Japan Trials were all done with MK4 vitamin K2 even though the Japanese obviously know about natto and MK7 and decided to not use that. As it stands there is at least ten times more biological research done with MK4 vitamin K2 in humans and animals than exists for MK7.
The standard argument for MK7, that it stays in teh blood longer is a problem, since the body has well adapted transport mechanisms targeted for MK4 it turns out that MK4 is more mobile in the body and gets used in more places than MK7.
Here are some pages that have a lot of science research references. I also find good references in the articles published in Life Extension Magazine.
http://www.nbihealth.com/t-mk4-power.aspx
http://www.nbihealth.com/t-mk7-hip-fractures.aspx
https://www.inspire.com/groups/national-osteoporosis-foundation/discussion/has-anyone-seen-this-new-to-me-information-about-vit-k-2-mk-7/reply/7576315/
Molly, I made recommendations in this resource. Please see those recommendations and ignore the detailed sections that click open. If you want references, click open the detailed sections where all the references are.
Chris,
I don’t find any references on your site- can you provide a reference for: “and it helps bring the high levels of male hormones found in women with polycystic ovarian syndrome (PCOS) back down to normal.” I would also like to find more information on this topic.
Thanks
The references are in the click-open detailed sections.
Lee get Thorne K2 from iherb. Like Anne I agree that the one without D3 is best. Free shipping with Aus Post or pay shipping with DHL. I’m in Perth and buy almost everything supplement like this way.
Anna, Thank you for your recommendation and reinforcement in the previous suggestion from Anne. I wasn’t sure that I would get any response having never done this before, and I am very grateful for all the help. This Website is so informative and helpful.
Thank you, Lee
Hi Chris, I am looking for a good k2 mk-4 supplement that I can either purchase here in Australia or have shipped here, I have looked at a few of your suggestions and they won’t deliver here.
Regards, Lee Morieson
I like Thornes mk4 drops the one without the vit D. I get it from i herb. Shops to oz in about 9 days. 🖒
Anne, Thank you for your recommendation, I have been extremely unwell and hadn’t checked my emails . I am really grateful to see that I have some help , obviously this is a new tool for me,
thank you, Lee
Let me know if you find one.
Could you direct me to a good source about the benefits of Vitamin K that I could share with parents who are hesitant about giving Vitamin K to their infant at birth for whatever reason? Thanks!
There is no reason to give vitK to a newborn, unless currently indicated, ie a cranial hematoma from a posterior birth.
I can’t but maybe someone else can chime in.
Hi. Thank you for all that information. I wonder if you could give your opinion on this supplement please. I am thinking it could be good for my son who doesn’t eat a great diet and is taking vitamin D. Garden of Life, Vitamin Code, Raw K-Complex, 60 Veggie Caps. Thanks, Wendy
Thanks Wendy I added this to the list of updates to make.
Hi Chris
I’m really interested in finding out more about both vitamin K1 and K2 and was delighted to find some recent research results at last. I am dairy-intolerant so have to avoid most cheese but my entry of “goat’s cheese” into the search box returned no results so I wondered if this means that you haven’t included goat’s cheese in your studies.
Do you know of any recent studies on the link between vitamin K1 and easily bruised skin?
Many thanks, Allyson
Usually the result of easily bruised skin comes from either scurvy resulting from low vitamin C levels, other low nutrients like copper that can look like scurvy, or a few medical conditions that lead to easy bruising. Vitamin K is involved only as its required to cause clotting that limits the bleeding after the bruising has happened. Vitamin K functions mostly in the liver where it potentiates clotting functions. Healthy, young mammals and humans convert a portion of Vitamin K to MK4 vitamin K2 for use in the body. This is reduced by ill health and age, thus the need for MK4 supplements to boost calcium metabolism in older adults with bone loss or artery calcification.
Everything we found in the literature is there. If something isn’t present, it means we could not find it reported anywhere. I would encourage you to broaden your search terms, for example just search “cheese” and browse to see if your specific search is missing something you’re looking for.
Hi Chris,
Thanks for a great article.
I was wondering what’s your opinion on different forms of MK in fermented dairy.
Would these other forms of MK have same benefits as MK4 and MK7? Do they get converted to MK4 as well?
According to this research, there is quite a lot of MK in all fermented dairy
http://cdn.nutrition.org/content/1/6/e000638
Hi Ales, I believe I addressed this in the article. If you didn’t already, click open the detailed section on vitamin K forms.
This resource is very educative, thanks. Is a high blood calcium count of 10.10 mg/dl ( reference range: 8.6-10.2 mg/dl) indicative of progressive calcification of the arteries as well as advancing osteoporosis? If so , will this not require high doses of K2, up to 45 mg/day?
Thanks
It’s a mild elevation – no need to be alarmed.
That being said, elevations in serum calcium can indicate a number of conditions, so if it continues to creep upward, you will want to investigate the possible causes.
Osteoporosis is one of these possible conditions, which can be diagnosed or excluded by performing a DEXA scan. Others may include hypothyroidism, parathyroid hyperfunction (if serum calcium were above 10.5 along with an increase in PTH and alkaline phosphatase and a decrease in phosphorus), cellular membrane disruption etc. I’m not sure you need to do anything right now – as your calcium is only mildly elevated and still within range – but if it went above 10.5, you’d want to see a doctor.
Kole, I think you want to verify that calcium stays that high over time. Also, check ionized Ca, which is more expensive and difficult to get but more accurate measure. You could have little blood pH shifts or albumin levels off that are driving Ca out of reference range while ionized Ca is normal. Also don’t interpret this without some input and guidance from a doctor, as if it is consistently elevated you could have primary hyperparathyroidism or something like that. No, the solution is not high-dose K. It is to find and fix the cause of hypercalcemia, if indeed it exists.
Love your new website! I loved the old one too, though. I’m a big fan of your work! Thanks for all the time that went in to this great resource!
I take a calcium supplement 500 mg in the morning and 500mg in the evening with D3. I can’t take K2 at all health reasons, Do I need to be concerned about the calcium going into my arteries instead of bone because I am not taking k2? I take calcium carbonate as it has more elemental calcium. Thank you
Chris, if you are young the body makes its own MK4 vitamin K2. If you are older or have heart health problems, then artery calcification is a concern. The main reason for not taking vitamin K2 is if a patient is on warfarin blood thinners that work by blocking vitamin K function. If this is the case you can ask the doctor to put you on an alternate form of blood thinning. If you are having a reaction to Vitamin K2, it is likely to be the MK7 form. Switch to the MK4 form alone which has much less in the way of side effects. This can be found available by mail order on the web.
David, I was under the impression, rightly or wrongly that K2 is a fat sol vitamin and worked synergystically with the other fat soluble vitamins. And had no role to play in blood thinning. That yes vit K1 if any left to play with after the no1 priority concern of the body to stop you bleeding to death foll trauma. That K1 could be converted to K2 but with todays diet, of too little K1 absorption, that K2 needs to be viewed separately and thus provided for. That blood thinning and so warfarin would not be affected by K2?
I also dispute the NHS/mainstream line that K1 rich foods should not be eaten if on warfarin. Warfarin surely is taken to stabilize the vicosity of the blood to ensure adequate ease of pumping of the blood by the heart. If a diet rich in K1 (lots of green leafys) are eaten consistently then the warfarin medication can be adjusted accordingly! Surely limiting the persons supply of vit rich, mineral rich, nutrient rich, and microbiome supporting food is not in the interest of health? Since when does the human suffer from the lack of warfarin, if food is supplying more of the need so less medication can be taken surely that is the ideal? you have lost me! I argue this for my 87yr old mother in law, who also has macular degeneration and type 11 diabetes for which healthy veg and fruit is a necessity. I fail to see why the NHS produces a leaflet stating basically that NO Green Veg should be eaten ever. To me this is tantamount to medical negligence and bullying of the elderly. I would appreciate it if someone could explain the protocol and advice.
Hi Lynne, I am fundamentally in agreement with most of your positions. People can eat greens or take MK4 vitaminK2 while on wafarin, but this has to be considered part of the treatment so you need to take the same pill or eat the same portion of salad each day for a consistent vitamin K/K2 intake. For doctors the problem is this, a patient will go out and eat a large salad occasionally and this throws off the INR measurement that warfarin is used to control. So in the eyes of medicine, its easier to tell patients to eat no salad than to try to explain the portion control. The option for the patient is to use a non-warfarin blood thinner not affected by vitamin K/K2 in the diet.
Thanks for your reply David. It is good to get clarification.
The term ‘Block’ which I have heard before from medical quarters can be confusing, as if somehow no amount of warfarin will work as intended, if any amount of K1 rich food is consumed. As such is how it is illustrated to the patient, a printed booklet: you must never eat broccoli etc.
Tantamount to criminal negligence towards the patient, in my book.
Shockingly poor medicine. Where does the ‘hypocratic oath’ sit with this attitude.
These ‘demi gods’ in white coats with stethoscopes pronounce: this is the way it is! And nothing any one else says can shift the created mindset.
So we are met every day with our 87yr mum saying, ‘Oh and I do love broccoli but I can’t have it. I am supposed to have lots of green vegetables and fruit to help my diabetes and macrodegeneration, I was told so but I haven’t been able to have for 4yrs now because I am taking Warfarin.’ So I will end up going blind now.
Criminal! People do not develop heart disease because they are short of warfarin! The drug should be adjusted around an individuals diet. As you say, portion control is the essence of successful treatment. This could have been part of the explanation to our mother. However there is no respect towards a patient and recognition of anyone other than a med professional’s having a brain. Otherwise such a booklet would never have been printed ready to shove into the hand of patients.
Soap box, I know. But doctors should recognise what harm they cause!
Read Kate Rheaume Bleue’s book ‘Vit K2 and the Calcium Paradox’ a little known vitamin that could save your life. Maybe it will provide the answers you need?
Can you recommend a good brand of k2 that doesn’t contain or have a derivative of soy? I have a soy allergy but need a k2 supplement.
Maggie I am in Australia and also have a soy allergy. I get my caps compounded at .5c per cap for 100 per bottle of mk4. Perhaps more expensive but I know what I’m getting!
I’m 61 years old and female. I’m concerned about bone density from results of my dexa bone scan. Trying to help keep situation from getting worse. I got a supplement from Whole Foods. It’s Whole Foods brand with 100mcg MK-7 derived from chickpeas. Thank you for the info in your article. I’m also trying to eat K 2 rich foods. Your article was very helpful.
I find this hyping of vitamins such as the K2 a little irresponsible. It is not well researched, there are a lot of unknowns. I bought K2 supplement and just one pill made me really dizzy, light-headed, my legs started tingling. But it is a good business. The K2 is probably cheap to make (ferment some food and extract the vitamin), but the supplements are very expensive. By going over various forums and user experiences, after filtering paid/dishonest reviews at Amazon etc, there are a lot of people who have problems and issues tolerating K2. You speak of synergy among the ADEK vitamins and minerals, but what if someone is defficient in one or several? Should he first correct the defficiencies, and then start K2? Or take K2 from the start? I guess nobody knows. We are all experimental rabbits toying with things we dont understand.
Its possible or likely that you bought the MK7 form of vitamin K2. This is known to have side effects similar to yours for those people sensitive to it, something like 10% to 30% of the population. Much of the promotional information is about MK7 since this is the most sold product, but the great major of research has been done with the MK4 form of vitamin K2. The MK4 vitamin K2 is important and its made by the bodies of mammals in youth and good health. Production declines with age and some health condition, so supplementing then becomes needed for best health. This is usually most evidenced with bone loss or artery calcification. There are six separate research trials of MK4 showing a reduction of 60% to 90% of bone breakage rates in the elderly in trials run with MK4 vitamin K2. Trials have also been conducted on daily doses up to 135 mg of MK4 without major health concerns. So the MK4 form is actually preferred for its safety and broader use in the body. MK7 is made by bacteria and its close enough to MK4 to have some useful function. You may want to switch to the MK4 form of vitamin K2 alone which is available by mail order. Be sure to read the side panels carefully for its content.
I’ve had a lot of success with taking MK4 vitamin K2 including reversing some annoying calcification of 15 years standing. This was actually an accident, the idea was to take MK4 for my long term bone health.
Hi, I took MK7 120mcg/D3 400 IU from the company Biomin. I am 37 years old, I have been suffering from brain fog and chronic respiratory infection due to chlamydia pneumoniae for the last two years. I discovered accidentaly after sunbathing, that chronic vitamin D deficiency might be responsible for my dysfunctional immunity, so I started catching vitamin D from sun and also supplementing vitamin A and I started feeling better. So I started researching vitamin D and discovered the various cofactors (ADEK, magnesium, zinc, boron). And I decided to give the K2 a try.
The problem with persistent chlamydia pneuomiae is that when you battle this infection, you experience die off effects. You first have to feel worse before feeling better, because the bacteria are intracellular and also cause secondary porphyria.
I will try to replenish my vit D and A stores a little more and give the K2 one more try later.
HI, You have the right idea but at too low a dose. Vitamin D3 supplements for best immune response should be in the 1000 IU per 25 pounds of weight for maintenance and 1500 IU for 1-2 months if starting from a low level. This should boost the ability of your immunity to identify and fight off the infection. Aim for blood levels of 80 ng/ml of vitamin D3 if you have or buy access to tests for D. In addition, the zinc is good, combine it with a copper supplement 10% the size of the zinc Dose. Include 5000 IU to 10,000 IU of Retinol vitamin A. Anything else that can be done such as taking 1-2000 mg vitamin C and eating enough protein would be helpful. You may need to increment the vitamin D dose slowly to reduce the side effects of the immune system activity if they are too intense.
Jacck,
may I ask exactly which supplement you took and in what dose?
Thanks!
Dear Chris,
I’d like to know your take on the effect of Vitamin K2 onto *existing* gall bladder stones.
Living with two stones (diagnosed 16 years ago), for the past 12 years I had not had any problems with them any more; I even had wondered, if they were still there.
Now, two weeks into taking Vitamin K1/K2MK4/K2MK7, I have had really heavy biliary colics – the first in 12 years.
Could there be a relation to the intake?
And: Will Vitamin K2 reduce/dissolve gall bladder stones over time?
Thank you for sharing all your scientific results with us!
Chris, Gouda cheese. Where does that come in terms of being a quality source of K2??? I’ve seen some other sights that claim Gouda is great, but not in the database.
Thanks David.Yes, it is the Thorne MK4 drops I am taking. ☺
The Thorne K2 drops would be effective if they are the MK4 form of vitamin K2.
Does anyone know if NOW brand MK7 is cis or trans? Using Thorne K2 drops too. I am thinking of adding Green pasture CLO and butter oil would I be overdoing it?
Why no lamb (or lamb offal) in the database?
I had Chronic Obstructive Pulmonary Disease (COPD) for 7 years, My first symptoms were dry cough, chest tightness and shortness of breath. This was ongoing for 3 years, my first chest x-ray only showed bronchitis. Finally I went to a pulmonologist and was diagnosed with COPD, I was immediately placed on Seebri Breezhaler, it’s an inhalation powder, I take it once a day in the morning. Finally, i started on COPD Herbal Formula i ordered from NewLife Herbal Clinic, the herbal formula worked 10x better than all the medications my pulmonologist had prescribed. I have had a total decline of symptoms since i started on this herbal formula, visit www .newlifeherbalclinic .com or email info@ newlifeherbalclinic. com
Larry HEMM
Dear Chris,
I would like to let You know that there seems to be (or at least there seems to have been) a huge problem with Life Extension’s Super K supplement (spoiler: according to two 2015 lab analyses, only about 1/4th of its MK-7 content is in the bioavailable trans form):
https://omegavia.com/how-to-choose-the-right-vitamin-k2-supplement/
God bless You and Your invaluable service to us,
Laszlo
Oops, I was stupid enough not to notice Zoltan’s comment above. Sorry…
Referring to Lazlo’s comments on Life Extentions K2 supplement, I also heard whereby this supplement by Life Extentions is not to be trusted. I believe I found it on Vin Kutty site? Thank you for all you do Chris, I am learning far more from your site than any of the other sites. Rosina Lock
Rosina is referring to this article: https://omegavia.com/how-to-choose-the-right-vitamin-k2-supplement/
I see that this person is pushing his own K2 supplement. Why should I trust him? I never heard of him.
I contacted Life Extension for their side of the story.
We are happy to address your question. Life Extension’s Super K with Advanced K2 complex contains 1500 mcg of K1, 1000 mcg of K2 as menaquinone-4 and 200 mcg of K2 as menaqunione-7 (MK-7). MK-7 can exist in two forms (isomers), referred to as cis and trans. The trans form is the form typically found in nature and our product contains a minimum of approximately 100 mcg of trans MK-7. At Life Extension, we do far more testing than most companies and we have subsequently sent our vitamin K2 MK-7 to two independent labs for evaluation of cis/trans isomer content. Both labs confirmed that the product contains approximately 50% trans and 50% cis MK-7 or more.
It should be noted that we provide a much higher dose of MK-7 in our products than most companies, typically at least double. There are very few companies that claim to provide MK-7 in a pure trans form and even fewer who report testing their product to verify. For the sake of argument, let’s say a company provides a product with 100 mcg trans MK-7 per softgel. By taking Life Extension’s Super K you would be getting approximately the same 100 mcg dose of trans MK-7 as part of the 200 mcg of combined MK-7 isomers in the product.
We have considered switching to an all-trans MK-7, but the increased cost of the raw material would necessitate a lower dose of MK-7 in the product and a product price increase, yielding no advantage over the MK-7 we currently use.
We are aware of the Omegavia website you reference and the information it contains. We sent our MK-7 to one of the same labs this site claims to have utilized. The results this lab reported to us showed an approximate 50/50 split of cis and trans. A second lab we utilized reported 86% trans content. Thus, two independent labs have verified that we have an MK-7 content of approximately 50% trans or more.
Regarding the InnovixLabs product showcased on the Omeagavia website, it contains 100 mcg of MK-7 and 500 mcg of MK-4. In LE’s Super K product, you are receiving approximately 100 mcg of trans MK-7 and 1000 mcg of MK-4. It is also notable that one lab test report that is missing from the Omegavia website is an MK-7 cis/trans analysis of their very own InnovixLabs product.
After all the testing, we feel our product provides a fantastic value! While it is not 100% all trans MK-7, it is providing approximately 100 mcg of trans MK-7 and likely even more than that amount. This fact means we provide more trans MK-7 than any other product on the market at our excellent price!
Thanks for sharing this JJ!!!
Hi Chris, I’ve been using AOR K for awhile now but the Mk4/Mk7 doses are identical (60 mcg each). I believe we need much more Mk4 so I’m looking for a new supplement. I’m checking into the top one you mentioned. Do you have any thoughts on the Life Extensions Super K?
https://www.vitacost.com/life-extension-super-k-with-advanced-k2-complex-90-softgels-4
While I’m not Chris, I’ve read that the MK7 in Life Extensions Super K was more than 70% cis-MK7, i.e. useless. This is the source: https://omegavia.com/how-to-choose-the-right-vitamin-k2-supplement/ Note the conflict of interest though.
Well that’s disappointing. I’m in Canada and the one Chris recommended doesn’t ship here.
Look for sales of Thorne liquid, its 1 mg per drop and not regulated to the same dose limits as MK4 capsules. Check out Vitacost for possible delivery to Canada, they carry a Vitacost Super K which is similar to Life Extension and which I found helpful.
I have been taking vit d3 healthmasters. i started to develop anxiety with tingles particular to one side of the body and on to of head.
I started taking vit k2 drops d.plantes. think it is mk1. has a very calming affect and tingles diminished over 4 days of taking it so far to only 5 percent left. wake up with uncomfortable breathing but after taking the drops it feels like tranquilising my body. im not hypochondriac. going for MRI this morning but really felt all anxiety symptoms in hands and feet is gone. i am very healthy person organic food 15 mins run per day. 3 children (3,5,7) and sensitive to sugar all my life. shaky if i have sugar without any other food.
Thanks Jurina, let us know what you find and I hope you are ok.
When I took 5 mg (in other words, 5,000 mCg) per day of K2 as the MK4 form per day for only three days, I suddenly got severe floaters and blood leakage on one eye. I had made no other changes to my supplements. I stopped the K2 on that third day.
A few days later, after much searching online, I found a few people had similar experiences with their eyes on that dose of the MK4 form of K2.
Please be careful everyone. That eye has still not healed a week later. There is no decent explanation for why it happened. The K1 form is the form reputed to affect blood thickness somehow, but the K2 isn’t usually discussed as affecting blood thickness — yet in me, and several other people, there were these fast eye problems.
5 mg is a high dose per day of MK4, no matter what the Japanese treatment folks say.
All forms of vitamin K support blood coagulation, which should not make any difference in your blood coagulability unless you are either on a 4-hydroxycoumarin or you have an undiagnosed clotting disorder and have been eating a vitamin K-deficient diet. I’m sorry about your problem, though I don’t know what could cause it. I do agree people should be cautious about multi-milligram doses.
Thank you for reporting this serious side effect. I’ve read lots of comments on use of MK4 so this side effect seems to be rare. My only guess is that the blood vessels of the eye were in bad condition and the large dose of MK4 was removing calcium fast enough that the blood vessel healing process could not keep up. Get the advice of an alternative medicine doctor if you still need the health benefits of MK4 before starting again.
Not sure if you’ll see this five years later David, but I think your hypothesis makes sense. And especially after I just read this on another site: “Vitamin K2 (MK-7) is the only compound known to impact arterial calcification through its activation of Matrix GLA Protein (MGP), which is a potent inhibitor of vascular calcification.
MGP is abundantly expressed in the eyes, where its role is to preserve and protect the structural integrity of the trabecular meshwork, sclera, and retinal ganglion cells…”
The package insert of Glakay – the Japanese MK4 drug used to treat osteoporosis – does, in fact mention “Eye abnormalities and arthralgia” among the possible side effects, with a combined incidence rate of less than 0.1%.
Hi Chris,
Do you see any contraindication for using K2 with birth control pills?
Reason being: The Pill is thought to have some degree of a coagulant effect. While K1 and K2 are physiologically different, I want to err on the side of caution. Appreciate your input.
K2 will not impact clotting at all unless you are currently deficient or on a 4-hydroxycoumarin, so I see no reason to be concerned about birth control except to be concerned about the effect you attribute to the birth control itself.
One of the absolute best write ups on vit k I’ve read yet thanks!
The birth control issue is what I was specifically seeking out on this round of researching as I was concerned about potential side effects/contradictions with clotting/stroke or anything else….
My girl has been on it…hormonal based pills…for a long time.
She’s not on any sort of blood thinner meds. But since you mentioned ‘if you are currently deficient’… She eats well overall…some meat, eggs, cheese, butter, veggies, but if I had to bet I would say shes deficient in vit k at least/especially the k2s.
What do we need to watch for or how would u suggest adding in vit k…should we titrate the dose up slowly or watch for any particular sign of problems? Does it matter if they are taken together at the same time of day?
Thanks again.
I have found a locally (EU) manufactured supplement that has
1,200mcg RE (4,000 IU) of Vitamin A as retinyl palmitate
100mcg (4,000 IU) of Vitamin D3 and
200mcg of Vitamin K2 as all-trans MK7
dissolved in MCT oil enclosed in softgel capsules, with a bit of soy lecithin but no other additives. Does this sound like a good formulation?
A/D ratio depends on your individual need, but intrinsically I see no problems in the formulation.
Hi Chris. Have been supplementing with a higher dose of Mk4, Mk7 and D for a couple of years to treat calcification of arteries. My Pl pla2 test has been coming back very high. I was wondering if vitamin K could be keeping the plaque from calcifying thereby causing it to be more unstable.
In my experience the MK4/MK7 is definitely helpful. After starting on a 1300 mcg MK4 & 100 mcg MK7 vitamin K2 supplement with 2000 IU of vitamin D3, my artery calcification symptoms gradually reduced by half at 5 months and were largely gone by 12 months. The idea is that taking 2000-5000 IU of vitamin D3 boosts body production of the MGP proteins that scavenge calcium in the body. The MK4 vitamin K2 activates the MGP so it can work. It also helps to take cod liver oil or retinol vitamin A which further boosts MGP protein production. Address other factors of artery health such as reducing intake of fructose sugars and carbohydrates to lower triglycerides and possibly follow the protocol in “NO More Heart Disease” by Dr Louis Ignarro to further protect the arteries. Keep your caclium intake in the 500-800 mg range, I found out that too much calcium can overwhelm the improved calcium clearance. A badly labeled supplement had me taking 2000 mg of calcium per day which restarted the symptoms! You may want to take a 5 mg MK4 or more supplement for best results.
David,
Which supplement did you start with? The one that had 1,300mcg MK4 and 100mcg MK7.
Thanks!
I did start with the supplement that had 1300 mcg of MK4 vitamin K2 for about two years. About a year ago I increased this by adding 5 mg of MK4 as an experiment. This has mildly increased my testosterone level which is helpful for as I’m over 60. In the trials in Japan, they did multiple month trials with 135 mg daily to assess safety and found there were no undue problems. That is very reasonable science, it provides that a 45 mg or less dose per day is generally safe if warfarin drugs are not in use.
What is someone who is on warfarin therapy supposed to do to keep their bones strong?
Susan, calcification makes plaque less stable, not more.
There is an obsolete medical hypothesis that the older plaques are stable. This is an unreasonable theory if you consider that the CAC test or calcium artery scan is currently the best indicator of heart disease progress and it looks at total calcification as a heart disease indicator, so to stay healthy you want less artery calcification, not more.
I agree you want less calcium, but for different reasons. The scan for calcium is used as a surrogate marker for total plaque, hard and soft. Calcium is about 20-25 percent of total plaque burden. As the calcium score rises, so does the soft plaque volume, which raises risk of rupture and clots. The older harder plaques block flow and collateral arteries grow around them, saving the tissue downstream, thus many clots in younger plaque areas are more lethal, since the artery is blocked totally without any bypass in place. So goes the argument for hard plaques being ‘safer’. But against that the higher calcium score means higher plaque volume in general, so that has to be taken into account, it’s like 4 to 1 or more soft plaque to calcium. Just removing calcium without lowering soft plaque volume gives me cause for concern, which I why I am on whole plant food diet, and exercise program, along with Larginine L cittruline 2:1 blend, plus nitric oxide lozenges and kale-beet shakes spiked with 100-150 mg sodium nitrite to provide nitric oxide via the oral route. I think exercise is risky without an anti-antherogenic diet and nitric oxide supplement at my age: 71.
Chris –
MESA study, published by Criqui et al in JACC in October of 2017
This study implies that the calcium density is a good thing and reduces the likelihood of a rupture. Removing Ca will make the soft plaque more vulnerable by reducing it’s stability. Here’s a video by Dr Ford Brewer explaining the study.
https://www.youtube.com/watch?v=oxIF3bUgnuo
You’ve said that eliminating the conditions for plaque formation in animal studies led to the natural elimination of plaque from the arteries.
Can you elaborate on how such a reversal could occur.
Hi Chris, I’m new here and LOVING your website!!! Just placed my first order from U.S. Wellness Meats which arrived this very morning, so fast and convenient!!! My mouth is watering while I wait for the liverwurst to thaw, thanks so much for the discount 😉
I haven’t read through all of the comments yet, so my apologies if this has already been covered. My question is regarding Jarlsberg Lite (low fat version), wondering does it have as much vitamin K as regular Jarlsberg? Also, does sitting on a store shelf under fluorescent lights affect the K?
Thanks so much for all you do!
Hi Meme,
Light is very destructive to vitamin K. I think the question is whether the supermarket uses any kind of light shielding that you don’t notice. I don’t know about the light versus regular. If it’s not in my database, then the I certainly don’t know. But definitely the light has an adverse effect. And you’re welcome! Welcome to my site! 🙂
How would you treat vitamin A toxicity? I’ve been taking high dosages of vit A for 4-5 months, without vit K2 or D. Can vit E and K2 help?
I would not assume toxicity. A good measure of toxicity is to test fasting serum vitamin A and serum vitamin A palmitate (also called serum retinol and serum retinyl esters) in the same blood draw. In toxicity, palmitate/esters should rise above 10% of the total.
D is most relevant, and lowering the A. K and E are probably also helpful to some degree.
You would need to be specific about the Vitamin A doses and form taken. Basically you will never convert enough beat carotene to get to a toxic level of vitamin A. The Retinol form of vitamin A is the most functional and can be toxic at extreme doses, so just avoid eating polar bear liver which has millions of IU per ounce! Some people have taken 50,000 IU of Retinol vitamin A for decades without toxic effects, so levels of 25,000 IU of Retinol would be rather safe. This assumes that a reasonable vitamin D3 level is maintained by sun or 5000-10,000 IU of vitamin D3 daily. The body evolved with a balance of vitamins D and A, if you give just retinol vitamin A to a vitamin D deficient person, it makes the vitamin D deficiency worse. That effect is the source of recent claims of vitamin A toxicity at low doses.
Chris – What is your take on transdermal, sublingual and/or topical absorption of K2?
For supplementing K2, D & A the lowest cost & lowest extra/questionable ingredients comes from liquid/oil based products. They typically recommend putting into water but would sublingual be better? And is additional fat needed in the diet at that time?
p.s. I lack a gallbladder so focus on a diet rich in fat soluble vitamins and supplementation with K2.
Hi Sean,
I’m not familiar with the absorption of these products at the moment.
Plenty of information in this article and easy to understand, thank you.
I have to take a 75mg dose of Asprin daily, would vitamin K2 be ok to take aswell?, I have low Vitamin D levels at the moment and the protocol I am following suggests taking Magnesium and K2 along side the Vitamin D3
Thank you.
The K2 is not related to the aspirin. I agree with Mg and K2 alongside D3 and I would add A.
Do you recommend taking all of these – magnesium + Vitamins A, D3 and K2 – at the same time, or a few hours apart?
I recommend not worrying about it.
Great article! I appreciate all the time you spent on this. It really helps break things down to easy to understand concepts.
I am taking MK7 with vitamin d (will be switching to the MK4/7 combo). I’ve been reading that when you supplement with K2 and D, that you also need to make sure you’re getting A in the form of cod liver oil. What are your thoughts on this?
Hi Kim, I agree with that.
Hi. Thank you for your informative article. Just concerned about the level of animal fats in cheese, butter, goats live pate, eggs. How is this sensible balanced out in a daily diet?
Hi Ken, I gave examples of how to balance it in the section on foods and in the first infographic.
First thing, to me it sounds that the author might have links to some of the pro-meat-dairy-egg industries… It wouldn’t surprise me at all, in a word where we can easily find “health professionals” sitting on boards of those industries and getting some cheques on the side. Besides, I would recommend the reading of “the China Study” which is a cornerstone in the field. All the naturopath and doctors who prescribed eating diets should have at least read it. If the arguments doesn’t convince you, be the environment situation which conveys you that eating animals, dairy is bad, bad for you, bad for the environment, etc. Did you know that the meat insuatry contributes to a ton more emissions than all the cars reunited in a year!
Can I take k2 supplements ? I have factor 5 Leiden. Not on any medications except spironolactone for acne.
Hi Susie, if you are not on vitamin K antagonist medication, there is no reason at all that you should avoid vitamin K supplements. However, given that you have a medical condition that is related to blood clotting, it is still advisable to discuss this with the physician who is caring for you before deliberately changing your vitamin K intake.
You are my new best friend! I thoroughly enjoyed the article!
Question: I have a CYP3A5 non-expressor SNP. Meaning that I’m not good at synthesizing steroid hormones from Cholesterol. Would MK-4 help activate this gene? Also, do you know what genes MK-4 activate? Also should I try to boost MK-4 intake, say up to the 200 microgram or beyond?
Hi Rob, I don’t know the answers to your questions, but I don’t see any harm in taking more than 200 µg of MK-4.
Any thoughts on the 2013 book by Rheaume-Bleue book ‘Vitamin K2 and the Calcium Paradox’?
Does it contain all this information or is it more a layman approach and/or not accurately up-to-date?
Hi Ben, it is a good book, but no it does not contain everything here, or else why would I bother writing this?
Phenomenal resource!
One thing you didn’t seem to address (unless I missed it) in the guide is the Vitamin K that our gut bacteria produces. Is the Vitamin K produced by our own gut bacteria available for the body to use? Would it be MK-4 MK-7, MK-10?
Thanks.
Hi Lyle, it probably makes no contribution at all, but if it makes any contribution it is quite small.
Thanks. What about the studies that suggest otherwise like this one? https://www.ncbi.nlm.nih.gov/pubmed/1492156
The problem is that later research trials were run on rats that had no intestinal bacteria and they were still producing MK4 Vitamin K2 internally by conversion of vitamin K within the body. So the theory of intestinal bacteria as making our vitamin K2 has been disproved. There is some vitamin K2, but it is the MK7 form which is not fully suited to use by mammals.
Thanks David. Do you happen to have a link any of those studies disproving the intestinal bacteria theory?
Yes have a look at this. Its apparent that MK4 is converted from vitamin K1 for the tissues that need it, no digestive conversion by bacteria in sterile rats. While this is done with rats, note that use of MK4 is common to all mammals, including humans. Tissue distributions in rats closely resemble those I’ve seen in humans.
https://www.ncbi.nlm.nih.gov/pubmed/9468334
Hello. I sent the following questions and comments to Innovix:
I saw your product recommended but upon my own review of your website I was left feeling not confident.
Your terms and agreement page seems to avoid any responsibility.
You do not name the process or certifier of your purity and potency.
You claim full spectrum but the product has only two vitamin k subtypes. Totally misleading.
Why should I pay a premium price with the above concerns? How can I recommend this product to anyone in good conscience?
I look forward to your response.
Thank you,
NF
Thanks for the article, this is so helpful!
I still have a question…would you say 600 mcg of k2 mk7 is too much?
Hi Lance, I would find that dose neither necessary nor particularly concerning.
Chris – Great work. Is there enough data for your K2 database to sorted by mcg/kcal (such as per 200kcal)?
When considering nutrient & energy density, 100g of duck fat is slightly different than 100g of meat.
Hi Sean, that’s an interesting proposal. Personally, I find it far more useful to use per 100 g, because it is a nice compromise between being fairly close to a true serving but being a standardized unit that crosses all foods. Per calorie is interesting, but as a primary normalization it has the severe disadvantage that people do not come even close to eating similar calories of all foods at a given time. I will put this on the list to consider as a future feature of the resource.
THank you for this very helpfull blog!! Here in germany vitamin k2 is so unknown…. hope that will change in the next few years.
Hi Chris
Thanks for all the research and valuable info you provide! I consume dairy foods every day, take a multi with 180ug of MK-4 K2 and 500iu of D3. I also take 2800mg of cod liver oil in capsules providing 10,000iu of A and 1,080iu D3 per day. What is your opinion of these amounts? Thanks again
Hi Rick, I see nothing wrong with it on the surface, but nutritional needs are very individualized.
Thank you Chris for this wonderful article.
Looking around for a good MK4 and MK7 supplement I send a mail to a few companies.
Asking them how and where their products are made and if they ever tested for the Trans VS Cis ratio.
Not many answers yet.
But “NOWFOODS” replied :
“All-trans Vitamin K-2 ( menaquinone-4) is produced from natural fermentation from yeast here in USA”
To what I understood MK4 is only found in animal sources and can not be made by fermentation like MK7 can be made by Soybean fermentation.
Nowhere can I find a source that MK4 can indeed be made by fermentation.
To the question if they are “BioIdentical” their response is :
“The term “bio-identical” typically applies to hormones, not vitamins. Obviously both are natural forms of vitamin K-2.”
This also contradicts what I read on a few places.
Not that I do not trust “NowFoods” , on the contrary … But these answers somewhat do not comply with what I read about MK4 and Vit-k in general.
Sound like a reply from a “sales” representative, throwing some misinformation on top of the pile.
Any Thoughts.?
Regards,
Christian
Hi Christian, the term “bioidentical” is not really a scientific term, but itThes intention is pretty clear, and in that sense there is no reason whatsoever to limit it to hormones. I’m skeptical about their claims to derive MK-4 from yeast.
Thank you for the wonderful resource Chris.
Question: Since K is fat soluble, can I take it once a week (or month), or must it be taken daily?
I love the podcast and appreciate the time and effort you put into all your projects.
Hi Robert, it is far preferable to take a daily.
Chris, as K2 is such an important “co-conspirator” in good bone health, are you able to comment on whether a K2 deficiency would reflect itself somehow in the levels of the PTH?
Gerard, I do not yet have any reason to think it would.
Wondering about fermented wheat germ?
As with any other food, it is more about the bacteria used in the fermentation than the food itself.
Hi Chris
I just found your blog and its so helpful!!
I have been taking 45 mcg of k2 for a a couple years. It has brought my vit d up but not quite enough. So I am thinking of increasing the dose.That amount brought my sons up within 3 months. Ive been trying to find information on whether it is ok to take more when I take a low dose aspirin daily. You explained the anti coagulants better than Ive seen. From what i can find (correct me if Im wrong) the aspirin effects platelet binding and is not a vit k antagonist. To me it would seem that it would be ok with aspirin. I take the aspirin because i have heterozygous factor v leiden. None of my drs have had an answer about k2 with that. I thought k2 was primarily involved in getting ca to the right place but you mention the mk7 left i n liver may be more effective in blood clotting. I know you cannot give medical advice but if I had a more complete understanding of how much k2 effects clotting I could make my decision or bring that info to my dr. On the same note on clotting I have never found if it is known if supplements such as fish oil , turmeric, ginger and others that are blood thinning do the same as aspirin. My drs do not know. Thank you so much
Hi Sarah, aspirin is not a vitamin K antagonist, and your genetic condition does not require restriction of vitamin K intake. In most people, vitamin K is present in adequate amounts to maximize blood clotting, but if that were not the case in you, it is conceivable that vitamin K could have some effect on blood clotting. It probably wouldn’t, but your doctors should at least be aware that you are supplementing if you choose to. Vitamin K will not raise vitamin D levels.
Hi Chris,
I take “Elequis” (apaxiban) anti-coagulant. It is a “direct factor Xa inhibitor”. Do you have any different warnings/comments concerning this class of anti-coagulant ?
thanks…
Hi Chris,
sorry, I see you answered my “Eliquis” question in your response to Zoltan’s comment on Dec. 16 above …
Your link above in the article to Thorne Mk-4 links to a different product (thorne mk-2), which my wife bought thinking the k-2 was the correct product. Which is the correct one?
Greg, the link goes exactly where it should, and Thorne does not make an MK-2 supplement.
How much D3 and Vitamin A do you recommend
I don’t know if it will be answered, as doses gets into disease and treatment, a no-no for supplement pushers and gurus. I am taking a kale shake a day (kale, blueberries, strawberries and water blended finely). I also snack here and there on carrots. That will get the A safely, I also take 4000 IU/D3/day in gel cap form. A is dangerous in supplement form I have read. best of luck, Bob
Carmella, that’s highly individual. About 2 to 3000 IU per day of vitamin D, and 5000 IU of vitamin A per day is probably a good start for the average person, but ultimately you need to tailor the numbers to your own needs.
Thanks, Chris for the copious info on K2.
I noticed in another article tufts-university-confirms-that-vitamin…etc. there is mention of the benefits of using vitamin A plus D to raise both MGP levels and carboxylated MGP, while reducing the ratio of under-carboxylated MGP to carboxylated. That sounds great. I was wondering if you had any recommendations about taking vitamin A with D and K2, perhaps some idea of how much A, D, K2, etc. I am 70 and interested in reducing coronary calcium score from a scan last year, very bad news scan 579 (400 is seriously bad, anything higher makes it worse). There aren’t yet human studies published, but at end of 2017, Dr. Leon Shurgers says he expects results using the coronary calcium scan over 2 years with group of 200 patients, split into placebo and test groups, to determine what effect if any, a daily dose of 360 mcg/day of MK7 has on coronary calcium scores. I am not sure if he is using vitamins A and D or what along with the K2. Dr. Eric Berg prescribes 400 mcg/day of MK7 and, get this, 40,000 mcg/day of vitamin D3 to ‘reverse calcium’. Sounds like a very high dose of D3 to me. He has a youtube video “a miracle” talking with a man that cleared his carotid plaques in a few months on this regimen. Appreciate anything you have to say around this. Regards, Bob
Interesting! Keeping an eye on this for hubby.
We have to establish how many IUs 40,000mcg is first. Mite not be off so much for a therapeutic dose under supervision.
Bob: I am also almost 70 years old and working to reduce my CAC scores even if I am asymptomatic to all signs, such as my blood pressure is almost perfect, 65-95. I’m taking 45-mg MK-4 and MK-7 from self-made natto with cod liver oil which has high content of vitamin A and D as suggested by Weston Price. Vincent
Hi, Vincent, have you been doing this long enough to warrant a retest to see if it is working? Are you planning to retake the test and see if the score was affected?
I am also taking serrapeptase, don’t remember if I mentioned it.. I have not yet had another scan. I am thinking of monitoring my carotid arteries instead, since it is cheaper and no radiation.
Bob:
I had my 2nd CAC test in 2016 after one year of the 1st test. The result still showed about 14% increase of CAC. It was in line with the 2016 study from “Yuji Ikari, Sho Torii, Atsushi Shioi and Toshio Okano: Impact of menaquinone-4 supplementation
on coronary artery calcification and arterial
stiffness: an open label single arm study.”
However, I am combining MK-4, MK-7, Vitamin A, D from cod liver oil, with oral chelation now. I am planning to have the 3rd test in this coming August to see if there is any improvement with this strategy. I don’t worry too much about radiation, if it is done only once a year.
According to the book of Calcium Bomb, adding an antibiotic might help to eliminate the Nano bacterial. However, I will not take any antibiotic medicine unless it is in a life threatening condition.
Vincent
It sounds good, you seem to be slowing it down. I am looking to get to a therapeutic dose, not just maintenance, so I’m starting taking 2 Koncentrated K caps/day. They have 500mcg MK7 each so that is 1mg MK7/day, also they have 25mg MK4 each, so that is 50mg MK4 and some K1 and astaxanthin for antioxidant. At 500mcg/day of MK7 the reduction in calcium score is supposed to start, so I am doubling that. The caps cost 45 for 60 caps, which for me will last one month if I take 2/day. I’m also taking Neo40 lozenges one per day, and making kale shakes (kale, blueberries, straberries and spinach with a pinch of sodium nitrite to generate lots of nitric oxide and reduce stress on arteries.) Nitrites got a bad rap regarding processed meats cooked at high temp, such as bacon. But mother’s milk is loaded with nitrite, it is in the body already, and contributes to healthy levels of nitric oxide. I’m also on a vegan diet. The most dangerous plaques are not calcified, but are soft and buttery, resulting mostly from a meat/dairy/oil diet. So none of that. Good luck and write when you get the test. bob@bobluhrs.com
Hi Bob,
As you note, no one has tested how this combination could impact atherosclerosis, so you really have to guess. You could reason from the work in kidney disease that K2 needs could rise up to around 4 mg, as decent guesswork. I think up to 5,000 IU of D and 10,000 IU of A are generally safe if all taken together and I would balance that with one capsule Jarrow TocoSorb and a very good diet. This is just a safe place to start, though, and if you are reversing atherosclerosis you should certainly be working under medical supervision.
Chris
Thanks, Chris. I am under supervision by an MD, the whole food plant-based diet alone in 6 weeks lowered my cholesterol from 270 to 165, BP from 140/90 to 110/65, and in a year my weight from 220 to 180. Doctor blown away, and forbore on the statins, even though he originally suggested I go on heavy statins and cardiological care, now he’s affirming my actions, wished his other patients did the same. He probably suspects this disease may be food-borne. I chose this diet from the small but well-done human trials by Dr. Esselstyn. I did not find such strong evidence anywhere else, which is shameful that more trials on diet are not being done, but there’s just no budgets anywhere for it. No one who stuck with his diet had any further heart or stroke issues at all. One guy out of 200 had a problem and said he was on the diet, but his wife says he wasn’t. So now he is. That was over a 5 year period on cases with prior heart attacks, strokes, angina, etc. The ones who fell off the diet, only 10 percent of the 200 patients, they had 66 percent incidence of MI, stroke, deaths. I can’t find this level of evidence anywhere, I when I got my scary score of 579 calcium, I went for it. Glad I did, I am stable without symptoms, climb long flights of stairs, weight train with fairly hefty weights a few times a week. Fingers crossed, but so far so good. At my gym in I saw two people carried out on gurneys by Medic One, both in the same week, BTW.
one further interesting point, my doc and I agreed to have my protein level checked since I was abandoning meat and dairy. Prior to the plant diet, it was low-side normal, after the plant diet it went up to the exact middle of the normal range. I am eating far less protein on the plant diet, but evidently using it so as to get higher serum levels. I was a heavy meat-eater, with cholesterols around 240-270 typically. I can’t say I love the new diet, but the old one gave me acid reflux and I was impotent. Now I have mild erections here and there, and no more acid reflux or medications for that, in fact I only take metformin for slightly elevated blood sugars. But they were elevated before the plant diet, and now have lowered on it. I saw an endocrinologist who said my sugars are coming down and keep up the diet. Insulin resistance is lower now, apparently, which may be lower fat in the muscle and other tissues.
Bob, you could be using your own muscle for protein. I’d have the doc check your 3-methylhistidine levels.
Hi Chris,
I have no problems with the site but did have a question.
I was just diagnosed with osteoporosis and just started taking Maximum Potency MenaQ7, Young Life Research by NattoPharma (100 mcg).
I am also taking MRM Bone Maximizer III with K2, MK7.
My vitamin D3 intake within this supplement, along with sublingual is 6,200 iu.
Do you think my dosages are adequate?
Thanks for any information you can give.
Hi Renee,
I don’t have any basis to alter the dose recommendations above, where I suggested 200 ug/d would be the target.
Chris
Loved this article Chris, but I did read somewhere that a person needs 100 mcg of k2 to every 1000 mgs of vit d3 to antidote calcification problems. Then I read by Dr. Klinghardt that a person only needs 100mcg of MK7 per every 10, 000iu of vit D3 thats a big difference. I have been taking the first recommendation for awhile now YIKES. I better figure out how really to dose using this with the d3 before I mess myself up. How did you formulate your dosage plan?
Thanks Carri
Hi Carri,
If you mean the dosage recommendation in this article, just click the “Click Here for a More Detailed Explanation” button in that section, where I explain it in great detail.
Awesome resource, thanks!
How much K2 in pickles?
Couldn’t find anything about pickles in your searchable database and when I search on the web no one says what kind of K is in pickles (K1 or K2 or both).
Also do different kinds of pickles contain K2 and others don’t?
Ninjaneer,
If I knew how much was in pickles, pickles would be in the database.
Hi Chris,
When I search in the database (no matter what I enter — including when I just select a category and hit “search”, as you describe above), I get a page that says:
“Not found, error 404
The page you are looking for no longer exists. Perhaps you can return back to the site’s homepage and see if you can find what you are looking for. Or, you can try finding it by using the search form below.”
Do you have any suggestions for what might be wrong?
Thanks!
-Eric
Eric,
We were probably fixing the database at that point and it temporarily went offline. I’m sorry for the inconvenience.
Chris
Thanks Chris for this useful resource on vitamin K2.
More attention should be given to this important vitamin.
I always make sure I take vitamin K2 whenever I take vitamin D supplements.
Hello Chris,
As a dietitian fascinated by the topic of K2, I appreciate your article and visuals on the topic. I expect K2 will soon experience the same degree of celebrity Vitamin D has achieved in recent years. Two unrelated questions for you:
1. Any risk of using Vit K2 with oral contraceptives (as these are thought to increase blood thickness)? Forgive me in advance as I’m not an expert in coagulation physiology.
2. Given the synergistic relationship of our “bone builders” (i.e. Vit D, calcium, K2, etc), do you think K2 supplementation can increase calcidiol (25(OH)D) or calcitriol (active D) to unhealthy levels?
*I’ve seen elevated calcitriol levels in a lady taking K2… not sure if there’s a relationship.
Thanks in advance. Look forward to future info.
~Megan
Hi Megan,
I don’t see a reason that K2 should be harmful with contraceptives, nor one that should cause it to raise calcitriol.
Chris
Hey Chris,
Just thought I’d say thank you for this site and your podcast contributions (through your own and as a guest on others’). I learn so much each and every time. Gold mines.
Cheers
Adam
I have read on line that Vit k can cause gum recession in your mouth. Have you ever heard this?
Steve,
I read an unpublished observation mentioned in a review paper that doses of K1 over 1 mg/d can contribute to periodontitis, but I don’t know of any published evidence for this.
Chris,
Thank you so very much for such detailed information! I have a question about dosage for children ages 8 and 11. They have trouble swallowing capsules. My doctor told me to give them each 10 drops of Thorne Vit D3/K2 each day to get 5000 IU Vit. D3. That is the form she sells in her office. Do you think it is better for them, and more cost effective, to give them only 2 drops of that formula/day and then use the Thorne Vit. D3 without K2 for the remainder 4000IU? Or get the MK4 alone and give them one drop every 5 days? I’m not sure if I missed it in your article, but I didn’t see any recommendations for children’s dosages. They don’t eat any of the food sources of K2, except my 8 year old will eat about 4 eggs/wk. Their diet is dairy and gluten free and we don’t eat red meat. Can you recommend a liquid form of MK7? They have both had cavities, even with good oral hygiene and minimal sweets, so I assume they would benefit from that form possibly more then the MK4 for teeth and bone health. Thank you so much for any guidance you can give me!
Carrie, without necessarily supporting the recommendation to get these doses as I do not know what they are based on, I think it would be more effective to take one drop of the mixture and make up the rest of the vitamin D with a vitamin D supplement.
Trying to find a resource that discusses Vit A, D, and K for children (12-18)
Will Chris’s work apply in some way?
Thanks for the hard work.
Hi Mike, there really isn’t a basis for saying anything specific about children when it comes to K2, so my recommendation would be to make similar food selections, but let their appetite for those foods do the trick. In other words, if the child because of a low body weight relative to an adult is eating half the food, eat half the K2. But if the child because of a high growth rate is eating twice the food of an adult, eat twice the K2.
Thank you for sharing your broad, in-depth, and great article about the important nutrient which is a missing link to so many modern chronicle diseases, vitamin K2.
Theoretically, Vitamin K2s, especially MK4, should be able to reverse arterial calcification, but what is your insight into this particular important subject because it correlates much better with the incidence of sudden death from heart attack than with cholesterols?
I have experimented on myself and my wife by using vitamin K2 for improving bone density for about three years by using MK7 from self-made natto (average 50 mg/day) and myself on reversing arterial calcification by using 45mg MK4 supplement for about one year. I have observed its positive effects on improving bone densities, but not on my calcium score.
The brief results are summarized as follows:
(1) Bond density: Both of us have observed significant improvements of the bone mass densities in the spine L1-4 areas (5.5% for me in two years and 1.7% for my wife in one year), but still with minor deteriorations in both of the femur neck areas (about 2.5% less for both us, but my result showed 11% improvement in the total left femur area);
(2) Calcium score: The total score still increased 11.7% in about one year even with minor decreases in the two less severe areas.
LMCA LADD LCOM RCPP Total
7/27/2015 109 432 56 50 647
8/22/2016 144 482 55 42 723
My Internet research indicated that the calcium score is expected to be increased 20-30% per year for most people and the 11.7% deterioration is not bad compared to this number. However, I am still disappointed to see the increment.
I am planning to give one more year for this experiment. If I cannot see improvement in my calcium score, then I am planning to use chelation plus antibiotics procedure as discussed in the book of “Calcium Bomb.” However, its results on improving calcium score are still inconsistent or controversial.
I will appreciate if you can share your insight into the subject. For instance, should I consider increasing the dose to 60 mg/day of MK4? By the way, I am about 70 years old without any heart symptom and with all health indicators, except cholesterol at 230, within normal range; and the brand of MK4 I am using is from Japan used for the treatment of osteoporosis.
Vincent, there is no evidence that 60 mg per day of MK-4 for can reverse calcified atherosclerosis.
Cees Vermeer and his Rotterdam group were able to reverse warfarin-induced arterial calcification in rats by giving them K2. I think they were using MK-7 because in an interview with Joseph Mercola he recommended taking MK-7 citing the half-life argument.
BTW in that same interview Mercola asked Cees if you could get K2 from your gut bacteria. His reply – only if you eat your own faeces!
couple things, warfarin-induced calcification vs long term buildup from atherosclerosis may make a difference; rats vs humans probably makes a difference. Question: how much difference?
Eating own faeces: apes do it, rabbits do it, most animals in the wild pick some up like fast food on occasion whilst starving. I already eat my own cooking, probably not much worse. Question: how much worse? 🙂
..One detail, the K2 dosage in the Cees Vermeer Rotterdam rat study was 100ug K2 as MK4/gram food, or 100mg/kg food. If we eat about one kg food per day, that is a big dose of MK4, about twice what the Japanese are using for their osteoporosis treatments, and it was always mixed with oil, so whatever MK4 we take should also be mixed with oil. In addition, all the food was laced with it, so our intake should be at least in divided doses if not with every intake of food.
If we were to use MK7, with oil, then the dose would be much less, maybe .5mg versus 100mg, or a 200:1 reduction in dosage. Interestingly, the MK7 form has a much longer half life, and can be taken once or twice a day, versus the one hour half life of Mk4.
Hi Bob, I must say that I always found the half-life argument in favour of MK-7 unconvincing. If the body really prefers MK-7 then why does it make MK-4? That’s like saying Vit D2 is preferable to D3.
And if the MK-4 disappears from the blood where does it go? It is just as likely that the cells preferably uptake MK-4 than it is that the MK-4 is excreted. The Rotterdam study didn’t address the issue IIRC, just assumed that longer half-life is better. Chris states above in his explanation that the MK-4 IS preferential taken up by the cells.
I don’t follow your argument re the K2 requirements. Surely the relevant measure is grams/kg of body weight, not gm/kg of food. The requirement to dose continuously throughout the day would only apply if the K2 were excreted rapidly rather than stored in the cells or body fat. Again IIRC K2 is fat-soluble not water-soluble, so likely to be stored. Also why would MK-7 be 200 times more effective than the same amount of MK-4?
The reference for the Rotterdam group’s paper is
http://www.bloodjournal.org/content/109/7/2823.long?sso-checked=true
Hi, Stuart, lot of questions there. I can remember that a talk by Dr. Shurgers, he said that MK7 at a dose of 360mcg/day was tested and found to fully carboxylate MGP. That’s a dose in the hundred or more times smaller range than the MK4 typical doses like the Vermeer rat study, or Japanese of 45mg/day osteoporosis dosing. He’s using 360mcg/day MK7 in his coronary calcium scan study, which will be the first to test in humans (although the sample is small, about 200 I think) if calcium scan scores can be improved or progression slowed by use of vitamin K2. I wrote and asked him if the study will be out soon. He is funded, I think, by Nattopharma, a company making MK7, so of course there’s the question of whether any bias towards MK7 exists. There could be, but the study should still be interesting, maybe enough to get other studies funded? I hope so.
I would like to hear any comments regarding taking red rice yeast and K2 – as in when to take each supplement – I would guess several hours apart from what I have learned here. thanx.
There are two different needs here. Red Rice Yeast is a kind of natural statin, so it works the same way as any statin drug does. The problem is that statins are not very effective and cholesterol levels are poor measures of cardiac health. Current research is starting to look at small, dense LDL cholesterol particles as important to heart disease. These are caused in the majority of people by consumption of fructose and the table sugar that contains fructose. By contrast, the MK4 vitamin K2 carboxylates MGP which is the calcium scavenging protein of the body. Since calcium deposits in arteries are the most reliable predictors of heart disease, this is probably your area of interest. The MK7 for of vitamin K2 is presumed to work in this way too, but I’ve read a couple of individual commentaries where people did not clear calcium until they switched to MK4.
So to take MK4, the dose is 1 mg to 5 mg daily with 2000 IU or more of vitamin D3 and the D3 increases the production of MGP. Doses of vitamin K2 in the 300 mcg to 500 mcg (this is 0.3 mg to 0.5 mg) do strongly reduce heart disease but the assumption is you will want to do better than this. Artery calcium levels should reduce over a period of 6 to 12 months.
Rather than take the red rice yeast, I would encourage you to read further on the use of plain Niacin by Dr Andrew Saul, the topic of heart disease in Life Extension magazine online, and use of Arginine in the book “NO More Hart Disease” by Dr Louis Ignarro. All of these should be more effective than statins depending on your particular problems.
Red yeast rice and statins inhibit the synthesis of MK-4, so it makes sense to take MK-4 if taking them. It also makes sense.to take coenzyme Q10. I don’t know of any reason to impose a specific time schedule in doing so.
I notice you have 3 Green Pastures butter oil listed in your Vit. K database. One is just described just as “butter oil” while the others are either “semi-solid fraction” or “liquid fraction” of the same brand.
What does this mean in real life usage?
For ex, does it mean that when I buy Green Pastures Butter oil, I should let it come to room temperature & thoroughly mix it up, then refrigerate it to make it solid & then the vit K content is an average of the 3 forms listed, making it really about 40ug?
Or does it mean that this butter oil is really somewhat less than 81.5ug because some of it (an unknown qty) is really “semi-solid” and “liquid”?
Thanks again for this very helpful resource!
Hmmmm, i didnt see these. Just the one green pastures oil.
Hi Helene,
Under Fats & Oils, the 3rd item is Green Pastures Butter Oil, Vit.K2-81.5, then further down at about the 12th item is Green Pastures Butter Oil (semi-solid fraction)-20.3 & then the 14th item is Green Pastures Butter Oil (liquid fraction)-17.1.
I’m not 100% sure, and this question would be better directed either to the Weston a Price Foundation or to Green Pastures. However, I believe the “butter oil” would be the actual product.
This form of mixed Vitamin K includes an antioxidant.
I’m not sure there is a reason to add an antioxidant to a Vit. K supplement?
https://www.k-vitamins.com
Terri, it could conceivably improve the shelf life.
Really great work! The podcast too!
I see there’s others who also in a way have this question;
Would supplementing with 1 capsule a week with Life Extension Super K With Advanced K2 Complex give the correct amount for maximum benefit?
Is it because its fat soluble we don’t need it every day?
Some also says its best to take with D3; how much D3 would you recommend?
Your question actually involves how the two forms of vitamin K2 are different. The MK4 form is made by the body in youth and good health so its always available and is transported around the body rapidly. The general advice is to take MK4 from one to three times a day as its half life in the body is measured as several hours. The MK7 form has a half life of 3.5 days so it doesn’t need to be taken as often in theory. The Life Extension Super K With Advanced K2 Complex has 1000 mcg of MK4 and 200 mcg of MK7, so this is a daily dose of MK4. Be alert that some people are sensitive to MK7 so if you start having symptoms of anxiety, sleeplessness, and a thumping heart beat happening, you will need to switch to a MK4 only vitamin K2. So this is not a once a week supplement and I have not seen any research testing it in this way.
All supplements are always best taken in divided doses once per day or even more frequently in smaller doses when possible. The half-life argument is dubious. There is no evidence that MK-4 needs to be taken more frequently than MK-7, and if its half-life in plasma is a result of its disappearance into relevant tissues, then it makes no sense to dose the MK-4 based on its half-life in plasma.
Goose liver is a bit hard to find locally where I live, but Costco sells duck liver pate, and Aldi carries pork liver Braunschweiger (Deutsche Kuche).
Any idea if chicken/pork/duck/beef liver is a close proxy to goose liver?
Ben, you can search the database for those foods.
Thanks so much, wondering if you are familiar with this product: https://rebelhealthtribe.com/megaquinone/
The product may be OK as MK7, but much of the research they are quoting is actually from MK4 research. In Japan the seven trials that showed reductions in bone breakage rates were all done with MK4 vitamin K2. The 1995 Japan medical adjunct use of Vitamin K2 is for the MK4 form. The tests of liver cancer being reduced by 90% by vitamin K2 were done with the MK4 form. So there is a lot of MK7 promotion being done here with MK4 research. The Diabetes research used MK4: ” Forty-two healthy young male volunteers received vitamin K2 (menatetrenone; 30 mg; Eisai Co., Japan)” See https://care.diabetesjournals.org/content/34/9/e147 So not to protest, but I would like to see MK7 stand on its own merits for the sake of accurate science.
I have it in my list for the next round of revisions to review this product.
I updated this resource in a number of ways, including clearing up the hard-to-read text of the second infographic, making the search database open in a new tab, migrating to a new server that has the site running three times faster, making the database even easier to use, adding over a dozen foods including butter oil and emu oil to the database, and, culminating tonight, adding ten more supplements to the review. You can see all the updates here: https://chrismasterjohnphd.com/2016/12/29/updates-ultimate-vitamin-k2-resource/
Hi Chris,
Thanks again for this awesome resource – I keep referring back to it as I figure out my supplementation plan.
I took a K2 supplement for the first time yesterday – 2 of the Innovix Labs pills, about 6 hours apart. I understand that’s double or more than you recommend taking, but I’m trying to heal a cavity that has been hurting a lot lately, so I was keen to experiment.
I had some trouble falling asleep, and then I woke up in the middle of the night and couldn’t get back to sleep for a few hours. I also had chest pain and some anxiety. When I did fall back asleep, I woke up drenched in sweat.
1) Based on some googling, it seems that I could be reacting negatively to the MK-7? Would love to hear your thoughts on this.
2) I’ve continued to experience slight chest pain today, but my tooth hasn’t hurt all day. Do you think it’s worth trying a single dose of the Innovix, or that if I reacted to 200mcg, I’m likely to react to 100mcg?
3) Also, am I likely to react to all versions of MK-7, or is there another one I should try? I was planning on trying the Thorne MK-4 only supplement instead and trying to get some MK-7 in my diet through cheese.
4) And lastly, based on your research, do you have a dosage you could recommend for healing cavities / remineralizing teeth? I was thinking it might be higher than your 200mcg/day maintenance dose. I’ve read some accounts online of people having success with Carlson’s 5mg/day.
Thank you!
For what it’s worth, I’ve tried several brands of MK7 and react to all of them, but do fine with MK4.
Hi Renee,
Have they all been derived from natto? I’m wondering if it’s contamination with a fermentation byproduct or the MK-7 itself. Use of a synthetic product, preferably the synthetic version of MenaQ7, would help clarify that. This may be a case of “if it ain’t broke don’t fix it,” but it would be nice to know what’s causing it. Off the top of my head I don’t know a mechanism whereby MK-7 itself would cause side effects that MK-4 does not.
Chris
Thanks for the idea! I’m sure they were all natto derived. I doubt if I’ve ever tried a synthetic. I’ll definitely give it a try. Fortunately, I can feed all my failed trials to my husband, so it’s not wasted money. lol
Hi Kay,
You’re welcome! I’m glad it’s something that makes you want to come back. I do hope it to be a continually built-up general go-to resource rather than a quick read.
1) I’d love to learn more about the MK-7 reactions, but right now I don’t know of a mechanism beyond contamination with something else that would cause this.
2) Well, without knowing exactly what you’re experiencing it’s hard to more than guess at what might work or not work. You actually took 1200 mcg, not 200. I recommend that supplement taken once every three days to yield an average of 200 mcg.
Did you do the reading before or after you took the supplement? It could easily be the result of a nocebo effect (like a placebo effect, but negative) if you had already read about similar reactions online. Or it could be some real biological sensitivity, which would be especially likely if you had never heard of any such reactions before taking it.
I think you should rationally decide what you feel safe experiencing. If your safety is in danger, I can’t ethically give you any advice over the internet besides talking to a doctor. What I would do in your situation is decide whether I would feel safe experiencing that reaction again. If I would not feel endangered by the potential for another similar reaction, then I would wait a few days and take one capsule and see what happened. If I felt my safety was threatened, I wouldn’t.
Simply on a the level of figuring out what is going on, I think the following experimental protocol makes sense. Compare the following:
a) Thorne MK-4 (pure MK-4)
b) Young Life Research MenaQ7 (pure synthetic MK-7)
c) Nested Naturals K2 (pure MK-7 from fermented chickpea)
d) Healthy Origins Vitamin K2 as MK-7 (pure MK-7 from natto)
If the reaction is the same across all of them, it’s a result of vitamin K or vitamin K2 in general. If it’s comparable across the three MK-7s but doesn’t happen with MK-4, it’s probably something about MK-7 itself. If it differs among the MK-7s, it’s probably a contaminant from the production method.
Notably, this is expensive, so I wouldn’t do this unless you can afford it, or unless you know other people who want to figure this out who would be willing to crowd-fund a group experiment.
Also, if you want to make this more rigorous, see my post here about how to randomize a self-experiment:
https://chrismasterjohnphd.com/2011/09/11/how-to-do-proper-self-experiment-and/
Also, if you want to protect against the power of suggestion (which is stronger than any of us want to believe), you should get someone to help you blind the experiment by emptying the capsules into something light-protected that will make them unrecognizable to you.
All of that is probably more than is worth your while, but might be useful depending on how much effort you want to put into figuring this out.
3) I don’t know the answer to that. Cheese has more MK-8 and MK-9 than MK-7,but they are likely to have similar benefits. Cheese also provides calcium and phosphorus and other nutrients helpful to remineralizing teeth.
4) I don’t think there’s any basis to such a dosing plan. Most people who benefit from Carlson’s probably benefit from 5 mg because it’s the lowest dose they tried. I don’t think there’s any basis to believe 5 mg is needed. There really isn’t any evidence that more than 200 ug is needed except that kidney disease patients seem to need up to a couple of milligrams. So you could formulate a guess that maybe a serious dysregulation of calcium distribution in other contexts, such as serious tooth decay, might require a couple of milligrams.
Hope that helps,
Chris
The data on reactions to MK7 are sparse, mostly people noticing that something feels wrong or some discussions on internet sites. Source of the “30% are sensitive to MK7” statement comes from Liz Pizzorno’s “Your Bones”, but I’m not sure the proportion of MK7 affected people are this high. Generally the symptoms are increased anxiety, sleeplessness, and a thumping heart beat or palpitations with possibly raised blood pressure. The symptoms decay in a time line consistent with the half life of MK7 in the body which is a 50% reduction every 3.5 days. The fact that MK7 builds up over a week also means that the symptoms may start several days or a week after MK7 is started and this complicates figuring out the cause and effect for many people.
Here are some discussions about it.
https://www.inspire.com/groups/national-osteoporosis-foundation/discussion/help-mk-7-vs-mk-4-questions/ An extended MK7 discussion set, I am Tango02 there.
https://www.inspire.com/groups/national-osteoporosis-foundation/discussion/vit-k2-mk4-or-mk7-which-is-better/
https://www.inspire.com/groups/national-osteoporosis-foundation/discussion/study-compares-absorbtion-k2-mk7-mk4/
https://www.thehealthyhomeeconomist.com/which-vitamin-k2-supplement-is-best-mk-4-or-mk-7/ See third and seventh comments for MK7 reactions
https://www.amazon.com/Jarrow-Formulas-MK-7-mcg-Count/product-reviews/B0013OVVFA Two reports of MK7 raising blood pressure
Thanks, David! Those were some of the ones I came across, plus the Amazon reviews of the Innovix product (as well as other brands). It’s been 2 days since I took 200mcg of MK-7, and most of my symptoms have gone away. I would love to know the mechanism behind the reaction.
Very interesting, I’m having an odd reaction that started the day of my 1st supplementation (100 mcg 2x daily from M7 natto derived supp) One of my joints (right thumb) is frozen stiff and painful. Since K-2 moves calcium out of soft tissue I wonder if it could be a kind of calcium-store detox.
I have a feeling Chris is right about me reacting to contamination. I’m going to try the synthetic and see what happens. I don’t do well with any ferments or natto or chickpeas or soy or any legume.
I feel inflamed in the sinus areas and a bit jittery when trying MK7, but it wore off within 24 hours, iirc.
Hi Chris,
Thanks for your thorough response, much appreciated!
For #2: The 200mcg versus 100mcg referred specifically to the MK-7 content of Innovix, not the total amount of K2. One capsule contains 100mcg of MK-7, so I took 200mcg of MK-7.
As for the nocebo effect.. Yes, it is possible since I had read about such reactions when first researching K2. It’s worth noting though that I had completely forgotten about what I had read when buying and taking this supplement. It was only after I experienced the side effects that I started googling and was reminded of what I had previously read.
Thanks also for the experimentation guidelines. I’ve decided that I would like to find a supplement that I could potentially take at a higher dose of MK-4 than one capsule of the Innovix provides, so I’d rather not put myself through the Innovix again since I reacted at a dosage of 2 capsules.
Also, due to expense, and the difficulty of getting these supplements in Canada, I will hold off on a proper experiment for now. Instead, I will try the Thorne MK-4 next and see how I do.
I would however like to try another form of MK-7. Other than brand, what is the difference between the MK-7 in Innovix and Young Life Research? Are they not both synthetic and bio-identical? Or are you just suggesting it as a means of separating out the MK-4 and MK-7? In which case, I might skip over that step since I’m trying the Thorne regardless, and try one of the natural forms of MK-7 instead.
I’ll come back and post how I do with any of these supplements, in case you or anyone else is interested in potential reactions to MK-7.
In case you are looking to make your list of K2 supplements more extensive, here are some of the options available in Canada:
https://naturalfactors.com/product/vitamin-k2/
https://well.ca/products/trophic-vitamin-k2_84507.html
https://www.aor.ca/en/product/vitamin-k2
https://www.pno.ca/item/vitamin-k2.html
https://www.nowfoods.com/supplements/vitamin-k-2-100-mcg-veg-capsules
https://well.ca/products/prairie-naturals-vitamin-k2_112695.html
https://www.nowfoods.com/supplements/mk-7-vitamin-k-2-100-mcg-veg-capsules
Thanks!
What I have read is that Canadian import regulators decided to limit all vitamin K2 supplements to a 120 mcg dosage for some reason. https://www.hc-sc.gc.ca/dhp-mps/prodnatur/faq/question_industry-industrie-eng.php#a25
So its hard to get an effective dose of MK4 vitamin K2 in pills there, but there is no seeming limit on importing Thorn liquid MK4 vitamin K2. Some people report getting higher doses delivered and some mail order sites will not ship to Canada.
Young Life Research makes a synthetic MK-7 that has no MK-4 and appears to be conscious about the background ingredients, so I think it would be a good test of pure MK-7.
My experience using vitamin K for treating dental problems has both good and bad results. Over time I had used a combination of vitamin K (K1, K2-7, and K2-4), plus vitamin D, and A to heal a cracked, infected wisdom tooth. Before I had the cracked tooth I had been taking vitamin D at 2000 IU’s, vitamin k2-7 (menaquinone) 100 mcg, and vitamin k1 (phytonadione) (500 mcg) every day for a few years. About a year and a half ago I had a chip in my wisdom tooth which revealed the possibility of tooth demineralization. I started taking more vitamin K2-7 (200 mcg) and continued to have pain and inflammation in the tooth for several months with no relief. Had to constantly using clove oil as an anesthetic and antiseptic a few times a day and putted off the dreaded tooth pulling appointment a few times. Then I read about vitamin A being needed for collagen production, and both tooth and bone formation, as it works synergistically with vitamin D in this regard, and is vital for a health immune response. It is also very likely that healthy gums need vitamin A (like they need vitamin C), and infected teeth can have a gum disease component. It was the vitamin A (not as beta carotene, but the real preformed all natural retinol from fish oil) taken at between 10,000 IU’s and 25,000’s IU’s per day that caused a dramatic reversal of the tooth infection and inflammation, and there was a big reduction in pain. After a week I could chew on that tooth whereas before it was so painful that even talking or closing my mouth caused significant discomfort and pain. However, about 2 month ago I decided to add vitamin K2-4 (menatetranone) because it has a lot of research for increasing bone density and since teeth are related to bones I thought it could result in further improvement. After being on it for about 1 month I noticed an increased return of pain and sensitivity but did not immediately associate it with vitamin K2-4. After a couple months with my tooth starting to feel more swollen and a bad taste oozing out of the reddened gum area that I never experienced before and had the appearance of being infected near the affected wisdom tooth , I stopped all of the oil soluble vitamins (A, D, K1, K2-7, and K2-4) and to my amazement all the pain, inflammation and nasty tasting substance disappeared by about 95% in just 2 days! It seems that the vitamin K2-4 may have been the culprit as I was taking 5000 mcg’s which is a pharmacological dose compared to what the diet normally provides and it was the last thing I added before those symptoms developed. It was quite literally amazing how fast the tooth seemed to become normal again within just 2 days of stopping the vitamins to the point where normal chewing did not cause any pain. Keep in mind part of the tooth had been cracked off (about 25%) and I had problems with it for about a year and a half so this was a major development. I think the oil soluble vitamin plus 1500 mg of calcium did help with remineralization but at some point the vitamin K2-4 became excessive or had some type of counteracting side effect. I have added back the A and D and not noticed any problems and will cautiously add back each of the vitamin K’s and see which one or ones caused the symptoms. I would still like to supplement with some vitamin K as I do believe it (and the D and A) helped save/restore the strength of the tooth so that it didn’t have to be pulled. Even with exposed pulp (has a somewhat darkened appearance where it chipped) it is completely functional which is pretty amazing. I thought tooth pulp was supposed to be super sensitive but it actually seems hard on the exposed surface. Tooth brush and dental probes have not caused any pain now that the inflammation and/or infection is resolved. It is so much better to be able to save your teeth than have artificial restorations put in which can have high failure rates and do not address the root cause of tooth demineralization. Even just one filling with drilling away part of the tooth starts to compromise the structure of the tooth and over time when repeated will lead to eventual loss of the tooth. A word of warning about people who potentially have gluten intolerance: For 19 years I had stayed off gluten suspecting an intolerance when I was in my 20’s. I did not have any cavities for almost 20 years. Then I tried eating gluten foods again just to test if I was really intolerant . After being on gluten for a year my wisdom tooth chipped (along with oen other tooth) and when I went to the dentist they found 9 cavities. I went off all gluten and having supplemented with all the oil soluble vitamins (A,D, K, and E) and calcium, I have no signs of progression with the cavities and the severe wisdom tooth problem has resolved. So it is really worth putting a lot of effort into your diet (possible allergies/intolerances that can cause malabsorption) adding some type of supplementation. Just be aware of possible side effects with the vitamins as signs the dosage is too high or is out of balance with the other vitamins. Some recent studes with just vitamin D have found a 2000 IU dose caused a 15% increased risk of fall and fracture with the elderly though there was no mention of being supplemented with K and A which are vital for D’s function. Also do not believe the negative story about vitamin A causing osteoporosis. It is needed for the collagen part of bone formation as I mentioned before and only if supplemented without D and K can increase the risk.
Hi Brik, could you please edit this comment to break it up into paragraphs? It is extremely difficult to read paragraphs that are this long in any context, and it is much harder to read them on the screen. I will try to read your comment if you can break it up into paragraphs that have an average of 3 to 4 sentences, and a maximum of 6 to 8 sentences. Thanks, Chris
Is there any update to this situation? What kind of fish oil did you take for vitamin A? Did you eat any kind of gluten free grains during your gluten free/cavity free 20 years?
Regarding the light sensitivity of Vit K, if I bought duck fat in a clear container & then put dark tape around it when i got it home – would at least the inner section of the fat retain a good amount of the Vit K?
Hi April,
I would think that if the duck fat is opaque, blue light shouldn’t penetrate very far into it and the fat in the center should be safe. However, I think everyone should protect all food and supplements from light as much as possible.
Chris
I’m also using a K2 Menatetrenone supplement by Relentless Improvement, which is a capsule with 15000 mcg MK-4, derived from flower extract geraniol (<2% Cis form) and I typically take 1 capsule daily. Would this still be considered a synthetic source?
Since it would seem I don't necessarily need such a large dose, is there any need for reducing the dosage gradually, rather than immediately? Do you think a powdered form such as in this product could be mixed with olive oil in order to make it easily diluted (the only other ingredient is a microcrystalline cellulose) for serving smaller dosages or would some alcohol also be needed to help with solubility?
Also, I do have some severe degeneration with cervical vertebrae from an whiplash-like accident 30 years ago: is there evidence that a larger pharmacological dose of K2 is useful in a case like this to help rebuild the vertebrae? I have been working on regaining mobility in my neck .
Thank you for the wonderful resource and thank you to everyone for their comments and suggestions.
The 15 mg dose of MK4 is reasonable, but you can sub divide the capsule by putting a pin in it if its liquid and squeezing out a third or half or dividing the dry contents similarly. From what I read, MK4 improves bone by increasing the soft connective tissue content of the bone which is why it improves the tensile strength and impact resistance of the bones while not making much difference in measurement by dexa BMD tests. So the MK4 is important but needs to be combined with other factors of Vitamin D, Vitamin A, Protein, boron, and possibly zinc, copper, and vitamin C. You also need to maintain a medically approved exercise program. All of these contribute to the building of connective tissue in the bones.
These topics are beyond what Chris is discussing, so don’t discuss them here but there are discussion groups on NOF.org that answer additional questions about bone health.
Protein is often ignored by medical people, but its important to get more than 1.2 grams per kg of body mass daily in order for the body to have enough protein to build new bone. This is 65 grams per 110 pounds. Bones are 50% protein by volume. The vitamin A will be important to having a good protein metabolism to build connective tissue. If you are low in vitamin c, magnesium, zinc, or copper, or boron, this reduces how fast the new connective tissue can be built, delaying bone reconstruction. So no low protein diet and check that your vitamins have these nutrients in good quantities. Please go to NOF.org Inspire if you need further discussion on this.
Thank you David for your advice suggestions.
Could you please post references for the stated daily protein requirement for rebuilding bone?
I appreciate the reference to NOF.org, but ultimately I do not have osteoporosis, simply specific cervical degeneration due to 30 plus years of wear and tear after an injury was ignored.
Protein requirements for bones are here. Note how bone maintenance falls off steeply below 1.0 g/kg/day. This is due to the evolved conservation measures of the body so that protein is available for the most important daily needs. https://blogs.creighton.edu/heaney/2014/07/25/the-paradox-of-osteoporosis-irreversibility-2/
Thanks for the article by Dr. Heaney.
Although he makes a convincing argument about the need for getting significantly more than the RDA of protein to enable bone rebuilding, in concert with sufficient calcium, esp. in the case of the elderly who have experienced bone loss, it certainly wasn’t fully established (as he well points out towards the end of the article about the need for more testing and the difficultly of doing future trials).
Also, note that he doesn’t bring vitamin D3 into the discussion until his mention of the nature of these trials, and that he never mentions the role of vitamin K2 at all. I suspect the two original studies he based his analysis on didn’t control for either of these vitamins and I wonder what part they’d play in reducing the need for more than RDA recommended protein.
Since the first study dealt with the elderly (not defined) it would be interesting to see if either study controlled for their digestive abilities, which it might be assumed declined to some degree for at least the elderly, (with some perhaps taking acid inhibitors and perhaps others taking some form of digestive aide (HCl, pancreatin, etc..), while perhaps even others suffered from symptom indicators of poor protein digestion. It would nice to know what type of protein they were using also, and its over-all bio-availability).
I think this might also be important when measuring the amount of protein they seemed to each need to start rebuilding bone.
Hi Alan,
I added the Relentless Improvement supplement to the comprehensive review today.
The Relentless Improvement supplement is synthetic, and the “flower extract” BS in their marketing page is misleading.
I don’t know of any evidence for using a larger dose to treat this specific condition. However, you could reason from the data on kidney patients that, based on the published dose-response, they may need about 2 mg/d to maximally carboxylate MGP. You could wager a guess that other serious conditions of calcium maldistribution also require a similar amount.
I don’t know of any reason to titrate down the dose slowly.
I think you could dilute it in olive oil, but one of the reasons I like the Thorne product is it is far easier to manipulate the dose. Here, you have to worry about whether the powdered agents will mix evenly. Also, be careful to do this under low-blue light, such as a yellow light, a red light, or the lights made by lowbluelights.com to avoid destruction of the vitamin K while you are manipulating it.
You’re welcome for the resource and thank you for reading and participating in the discussion.
Chris
I have used the Thorne MK4 product and unfortunately, I found that using the dropper I ended up with significantly less servings than was expected from the labeling. I don’t know if that was due to mislabeling or the dropper over-serving the K2. Using 15 mg/day, it was used up in about 60 days, not 80 days as per labeling. If due to the dropper, and the total MK4 k2 is accurate, then I was actually taking 20 mg /day. Perhaps this is within an acceptable degree of error for this supplement given it’s safety record. Otherwise, I had no problems using the product.
Thanks for your reply and updates.
In regards to the Relentless Improvement product, please note that they do offer a MK7 -free MK4-only product for a lower price (whch I have bought via Amazon).
I’d like to let you new about a new vitamin K2 product (vK2) IT contains pharmaceutical grade MK4 (5mg) + MK7 (100mcg)
If the brand of Vitamin K2 is NOT yellow, it is not pharmaceutical grade
for more info, please visit http://www. v-k2.com
Hey Chris,
thanks for all the great work. I still have a question though. Is synthetic MK-4 really bioidentical when it’s structurally the same? I have tried supplementing with Thorne Research’s D3/K2 blend but don’t get the same teeth strengthening effects that I got from consuming grass-fed butter (same with MK-7 supplements). I can’t eat dairy anymore because of an autoimmune condition and grass-fed tallow or anything of that sort is hard to come by where I live. Do you have any thoughts/advice? Thanks again for all the great information!
Hi Moritz,
I don’t know any reason to believe that MK-4 is not biologically identical. Then again, I don’t know of a critical experiment that has shown that to be true. For example, if you could compare MK-4 derived from food and MK-4 synthesized, and then put into identical food matrices with all other compounds held constant, you could answer that question for certain. Although, it would be profoundly difficult to design that experiment.
So, I am satisfied for now with believing that assays of the chemical structure are correct that the structures, and thus the biological properties, are the same.
What is notable is that grass-fed butter is a food, not a supplement, and it is full of all kinds of other things. So, perhaps the broad spectrum of nutrients in the butter, including even the fatty acids, are providing you with benefits that no K vitamin on its own provides.
Chris
Kris can I get signed up for your newsletter? I saw a link to do so but then lost it and can’t find it
Thanks
Hi Teri,
You can sign up at chrismasterjohnphd.com/newsletter
Chris
Hi Chris–
Thanks for such a great resource on K2.
For those of us that like seeing a lot of data and using phone screens more frequently, are you planning any kind of table format or downloadable CSV form for the food data? Maybe a simple table that can be sorted by column with total K2 and mk4 and mk7 info, with links for the detailed results?
Hi Serge,
I don’t really see how a downloadable csv is easier to use on a phone. That strikes me as much more difficult to use, given that it would involve lots of scrolling, and given that phones are not really designed to deal well with CSVs (though I suppose Google is on its way to improving that).
What currently, feature wise, do you find yourself unable to do with this database on mobile?
I find that it works great on my iphone. Loads very quick now with the server migration, easy to type into the box, easy to read the result.
I believe what you can’t currently do that would be useful is sort by specific MKs. I wanted to do that, but couldn’t figure out a way to make the interface user-friendly by launch time. It’s a feature I hope to add in the near future.
However, that has nothing to do with mobile versus desktop.
What do you want on mobile? What else do you want, in terms of specific features?
Chris
I love all your research and the way you explain things. I also love that you “name names” so I don’t waste anytime if I want to take some of your advice. Thank you for doing what you do. I started following you years ago when a doctor tried scaring me into taking cholesterol medicine.
Debbie, thanks for the props! I appreciate your participation here.
Thank you, Chris, for this wonderful article! As a diabetic, I follow a ketogenic lifestyle and run a group helping others control their diabetes. This article will be very helpful!
I recently had a dexascan that showed some Bone loss (osteopenia, not at an osteoporosis level). My doc wanted to put me on Fosomax, which I refused due to the complications it can cause and also that the FDA had warned Mercy that it should NOT be used for osteopenia.
Anyway, I’ve been researching and learning about osteopenia and D3, K2, calcium, and magnesium! Interesting.
Your great in depth article came along , thank you!!
Do you have a suggestion of which of the supplements you suggested would be best? A combo of all the mks or focus more on one?
Your reviews are great, and I love that they give links and prices. I know our health is priceless, but not everyone has endless finds😊
Hi Susan, great to hear from you! I culled out three supplements as my top recommendations. I like the Innovix for its combination best, but I think it depends on your background diet as well. For example, if you ate tons of natto and never ate animal products, I’d focus more on MK-4, or if you ate lots of goose liver and never ate anything fermented, I’d focus more on MK-7. But I think a mix is best for most people.
By the way, Chris, I finally listened to the podcast that goes with this a few days ago and it was fantastic! I am a auditory learner and while I might not read all of the expanded sections, I love hearing all the details in the podcast. Thanks for doing them and for making the https://chrismasterjohnphd.com/amazon link. That will be an easy way for me and others to contribute to you financially.
And, my husband watches a lot of YouTube, but will only watch health videos that DON’T have the details. lol So, consider adding to your future projects making videos for the masses and put them on a separate channel or mark them in some way (like the Dummies book titles, but something else) so newbies won’t stumble into the detailed videos never to return. lol
And, lastly thank you so much for offering all of this great content free. I would hate for anyone to not get this information because of money and people who can afford to contribute financially will be on the lookout for your paid products and services.
Hi ReneeAnn,
I’m glad you loved the podcast! That’s great to hear about different learning styles. The second youtube channel sounds like a great idea and producing video content is something I’ll expand into more seriously in 2017.
Thank you for thinking about my financial welfare! Yes, it is wonderful to have this free content. The affiliate links help it sort of break even and justify my time spent on the free material, and the traffic to my site has increased enormously, which will help me put out things I charge for successfully. So, I’m hoping for a model where each things helps out the other and allows me to alternate between paid and free information in a way that produces tons of epic free stuff like this for everyone to share.
Chris
Corrected post
First I want to thank you for going out on a limb to better understand and share some of your thoughts about the unknowns of vitamin K dosage and side effects. I’m hoping you can clarify a question about what form of vitamin K2 you were referring to as well as answer a couple of questions I have. In episode 29 of your podcast, you suggest 200 mcg of vitamin K2 as a possibly safe, efficient dosage compared to the 45 mg in the osteoporosis studies. Was this 200 mcg dosage you mentioned the MK4 form of vitamin K2 since the osteo studies you were referring to used 45,000 mcg? If so, why do you think something at least 40 times lower in dosage might have a bone health benefit? Is there research to show that 200 mcg can generate sufficient carboxylated osteocalcin, or is it possible you were referring to the MK7 form since 180 mcg appears to have a significant effect in generating OC in human studies? Are there studies using lower dosages of MK4 that support good levels of OC, and if so, do you think MK4 and MK7 might have equivalent potencies in generating OC, or do they target different tissues for ucOC to OC conversion?
Thanks,
Brien
Update: Just found this recent study which seems to partially answer one of my questions and shows the importance of fine tuning the dosage. “Fifteen healthy males aged 25.0 years (median) participated in a non-placebo-controlled dose-examination study. They received menaquinone-4 daily for 5 weeks at 0, 300, 600, 900, and 1500 μg/day in weeks 1, 2, 3, 4, and 5, respectively. Compared with baseline, serum γ-carboxylated osteocalcin levels were significantly greater at an intake of 900 μg/day or more; serum undercarboxylated osteocalcin levels and the ratio of serum undercarboxylated osteocalcin to γ-carboxylated osteocalcin were significantly lower than baseline at doses of 600 μg/day or more.” https://www.ncbi.nlm.nih.gov/pubmed/25163392
Hi Brien,
Thanks for your kind words.
This article contains very detailed answers to your questions. Please click open the boxes that say “Click here for a more detailed explanation” under the section “The Health Benefits of Vitamin K2” and read both “Biochemistry” and “Evidence,” and then click open the box under “How Much Vitamin K2 Do We Need?” These are the most relevant, but the box under “Why the Form of Vitamin K You Eat Is So Important” may also be useful.
I do not want to discuss this extensively until you’ve read those, but here are some very brief answers:
1) I was referring to total K2 intake because there is no basis to give form-specific dosing recommendations.
2) The 45 mg/d MK-4 osteoporosis studies have no relevance at all to the value of vitamin K nutrition. They are using supraphysiological doses of MK-4 in which case it should be regarded as a drug.
3) Vitamin K has an important role in bone mineralization, and this is not related to the pharmacological effects of MK-4 as a drug.
4) The bone benefit probably has little if anything to do with the carboxylation of osteocalcin. It probably derives most of its benefit from the carboxylation of MGP.
5) There is no basis for distinguishing the dose-related potencies of MK-4 and MK-7 on osteocalcin. But they almost certainly have different tissue distributions.
Point 5 is why I believe it is best to distribute total K2 intake among various forms.
Chris
Thank you Chris!
Your tutorials you recommended under “Biochemistry” and “Evidence” were very helpful in me gaining a better understanding of the different but complementary and overlapping roles of each MK type. It makes sense that we should get a mixture of each type and the sum of the dosages should be 200 mcg as you suggested in the Podcast.
I can see I misunderstood the different roles of the vitamin K dependent proteins and now understand the metabolic role of osteocalcin versus the bone growth role of matrix GLA protein. Very interesting indeed!
I’m also trying to determine what dosage of vitamin A is needed depending on individual requirements and vitamin D intake since insufficient vit A can result in vitamin D toxicity and decreased bone density. Is this because vit A has a role in collagen production and bone contains a collagen matrix? I recall seeing on the Weston A. Price website that the recommended ratio range of vit A to vit D is 5 – 8 to 1. Is there a way to find out which part of the range is best for a person? Does the vitamin K2 intake impact that ratio and is there a suggested ratio between A and K? I’ve even heard that vitamin E is involved in the interaction of oil soluble vitamins and is needed to prevent both A and D toxicity possibly related to its role as an antioxidant, but its difficult to know what a safe dosage is since there have so many negative studies on vitamin E and heart health.
Is there a way of knowing what a relatively safe vitamin D dosage is short of having your blood level tested?
Thanks,
Brien
Have you also considered the role of iron Brian, if supplementing with vit D. This brilliant resource of Chris’s on K2 is invaluable and no doubt we should be supplementing with K2 and getting MK4 from our diet. But vitamin D supplementation can I believe increase iron absorption, dysregulate copper/iron metabolism and leave us with dangerously high levels of stored iron, google Morley Robbins work on iron. So I believe we need to be careful on many fronts as the system works as a whole. just as we see with calcium metabolism, K2 and the other fat soluble vitamins. Are there any pointers you can give us Chris when it comes to fat sol vitamins particularly D and iron/copper metabolism. Or thoughts on Morley Robbins work? Would be much appreciated.
I take vit d and my ferritins horribly low, even with taking iron! I wish vit d raised absorption so alarmingly. I cant raise my ferritin no matter what.
Was 26, after 3 mos of iron pills, tested at 11, less than half what it was.
Hi Lynne,
That is interesting that you heard vitamin D can increase iron levels and dysregulate copper metabolism. When I was in my 20’s my ferritin level was 210, a level very high for some only 25. usually it is only 35 to 70 at that age. I felt very ill from it with brain fog, fatigue, and joint pain. I subsequently donated blood several times bringing it down to a more reasonable level of 70. I had been taking extra vit D back then, lying out in the sun, and taking iron pills here and tehre so maybe the D made it worse. I now take Milk Thistle and turmeric every day, and both of these have the ability to chelate and remove excess iron. Milk Thistle was tested for its iron reducing ability in clinical studies and its silymarin content was very effective in binding to iron and causing its excretion.
I think one of the biggest tragedies going on in our society is the
rampant dissemination of the false recommendation that everyone should be taking high dosages of vitamin D without having blood levels tested and without balancing it with the essential balancing partners of especially vitamin A, but also vit K. There is a growing understanding of the need for vit K to prevent calcification, but even these people don’t recognize just how vital vit A is for preventing vit D toxicity. I think this actually killed my Dad by causing him to develop COPD which I think was actually emphysema. He had been taking vit D for many years without the essential balanced levels of vit A. Vit A is required for healthy epithelial cells including those lining the lungs and air sacks. By depleting his vit A, since as Chris pointed out, “This suggests that vitamin D increases the need for and turnover of vitamin A.” , he basically was starving for vit A and destroying his lungs by this deficiency and gasping for air which required constant use of his oxygen tank.
Such horrendous suffering che experiences could have been avoided if our free market, for profit society was more compassionately responsible and didn’t have its slanted, inaccurate marketing message of “high dose vitamin D is good for you” without considering the consequences upon millions of unwitting people who will be harmed with calcified arteries, emphysema, cancers, heart attacks, strokes and other hideous maladies leading to death. Walmart and other big box stores like Costco are irresponsibly selling high dose vit D at 5000 IU’s or more without the balance of vit A a contained in it or having a safety warning to supplement with these other vitamins A and K, and to test blood levels to ensure the need for supplementation. I have known so many people who tell me theirdoctors were prescribing 50,000 IU’s per week of vit D for depression which will lead to horrible health problems within a few years down the line. This is a real national tragedy with everyone blindly and recklessly being led to jump onto the vit D bandwagon because “its the most studied” vitamin and can cure and prevent virtually every known disease and malady to mankind. Shame on the vitamin D Council for propagating this careless misinformation. Thank God for Chris Masterjohn, Ph.D. and the WAPF for warning people about the need for the full spectrum of nutrients that interact together in balanced proportions.
Brien
Helene, a) are you taking an absorbable iron, there is a lot of rubbish out there being sold, Ferrous Sulphate won’t help anyone. I am sure you are eating tons of iron rich foods and if you eat/take vit c at the same time that will help with absorption. So eat your grass fed liver with lots of lemon juice b) are you sure you need to raise your stored iron levels. highish Ferritin is an indication of tissue breakdown and inflammation. And puts you at risk of harmful unbound iron flooding your system when the cell dies. I presume you have had a full iron panel blood test – serum iron, total iron binding capacity and transferrin saturation % so know what your real iron status is. All that being the case Morley Robbins (you tube interviews) research/discusses the role of iron and copper, working together and cerulplasmin, zinc magnesium all synergystically working together, fat sol vitamins. Got to get it all right or nothing is going to shift so it seems. Morley Robbins states that med prof have iron/ferritin all wrong and I think he says ferritin of 20 is ideal? I have heard that cardiologists like to see ferritin lower than that.
Helene, I think Chris has researched the role of iron, I believe he has a potential iron issue. So I am trying to find articles Chris has done to try and understand. I was advised to look at Morey Robbins work and it does seem to make sense. I would definitely listen to Morley Robbins but I would definitely trust Chris’s stance, if I can find such info. Perhaps Chris’s facebook page?
Hi Lynne,
I’m not familiar with an effect of vitamin D on iron absorption. Could you point me to a very succinct source arguing in favor of this point?
Chris
Hi Lynne,
Actually ferritin is strongly protective of free iron doing damage. It increases in the immune response to sequester free iron and prevent pathogens from having access to it.
Chris
Hi Lynne,
I do have an iron issue but haven’t written much about it. I’ll be doing a podcast on iron soon. 🙂
Chris
Hi Brien, awful to hear of your father’s suffering and death that could have been prevented. I am with you on all points, and I live in the UK with the the often archaic NHS. I believe similarly that my parents died unnecessarily and that’s putting it nicely, killed is how I really feel. My dad being treated for asthma for 12 months following a short chest infection when really the bacteria had migrated to his heart and all along were destroying his mitral valve and consequently his oxygen carrying red blood cells. but all he got was a steroid inhaler. It’s not as if all the signs of total weakness, unable to get breath, couple of months and a small stroke. For goodness sake when do the med profession join the dots! Neurology here standard practice is refer to cardiology who determined as just routine referral that dad fine, declared nothing wrong with his heart! I insisted there was and demanded further monitoring. The cardiologist stated that would be many weeks but agreed. During that period my dad suffered his heart attack.
My mum celiac – on gluten free diet, Med prof sent for her out of the blue to review her case!! Endoscopy – no sign of disease – well no ! Why would there be, she had healed, having been on a strict gluten free diet for 24 years. They told her to resume eating gluten for 6 weeks and watch for signs of stomach upset and if none she was cured and could eat a normal diet. My mum believing anyone with a white coat and a stethoscope utters words of truth and wisdom, did as she was told. No digestive issues, they came later – she wasn’t told to look for neurological issues – bed ridden with migraines, vertigo, eventually dementia like symptoms and eventually dying of pancreatic cancer all linked to gluten. Why did her doctors not make the link, but instead live in a world of tunnel vision and still unfortunately for millions, still do.
We truly have to take responsibility for our own health.
Interesting that you did manage to get your ferritin levels down to such a good level with blood donations. My ferritin is 140 and so I wish to donate but quite frankly am so worried because my serum iron is so low and saturation is only 18% So I guess anemia of inflammation where my body is storing iron to prevent bacteria/ parasite infection feeding on the iron.
So would blood donation still be appropriate when I am so low in iron? I f anyone could give me any insight into this conundrum, I would be truly grateful.
I no longer have blood loss through menstruation but when I did I was always ill with headaches and dizziness which with hindsight could have been an anaemic reaction.
This summer the Govt health guidelines, have announced that everyone should be supplementing with vitamin D. No mention of K2 and the other fat soluble vitamins. And this in a country where the main health guideline is to eat a low fat diet!
A few years ago I was sent a prescription from the hospital following a bone density scan for the prevention of the possibility that I may develop pre osteopenia (which is pre osteoporosis) because they weren’t sure if my height had reduced slightly!! You only have to take a deep breath when having height measured and it can swell a couple of inches 🙂 The medication was vit D + calcium! aggh heaven help us.
Now that IS something. I was told under 50 is not good and if im still tired, to get it to 100. AND that my very low ferritin was due to inflammation! Lol
All this from a functional MD.
Oh dear lord…
Whe I get internet enough for a browser i will look at Robbins vid.
Hi Lynne,
Thank you for sharing the unfortunate background about what happened to your parents in the medical system. It just confirms that we so often can’t rely on the system or trust that they have the expertise and do their due diligence to treat us properly.
Regarding your question about the ferritin levels, inflammation can falsely elevate the ferritin number so they suggest repeating the test once the inflammation is brought under control. If your ferritin is high but your serum iron and saturation is low that could be a sign of a falsely elevated ferritin value, or it could be that your body is sequestering the iron to keep you from getting infections and to reduce oxidative damage from inflammation. There are other causes of anemia such as deficiencies of zinc, vitamin B-6, copper, and possibly other nutrients and causes. However, if your ferritin really is confirmed to be that high it might be a good idea to donate the blood. For every 1 pint I donated it brought my ferritin number down by about 20 to 25 points which roughly corresponds to about 200 to 250 mg of stored iron. I had some inflammatory joint issues at the time so I thought perhaps that the high ferritin value could have been a false value. However, after donating blood about 4 or 5 times it brought the ferritin value down to a safe number which confirmed to me that the original high value was not a false value caused by inflammation. I did feel a lot better with improved mental acuity and joint function.
Hi Brien,
Thanks for your positive feedback and I’m glad you found the detailed sections helpful.
I honestly do not believe there is sufficient data to recommend specific ratios of A and D, and I also don’t believe that a particular ratio is best. I believe it is best to moderate status of each individually but in a similar way.
In other words, if you are megadosing supplements, you ought to megadose them all equally or give equal attention to the possibility of megadosing each. And if you are leaving it up to sheer luck whether you get adequacy, you ought to do that with all of them. But the safest approach is to use a relatively conservative evidence-based way to manage each status in what we currently gather to be an optimal range.
For vitamin D this is rather easy. Unless you have a VDR mutation that makes you insensitive to vitamin D, I think you want to have your 25(OH)D somewhere between 30-40 for most whites and somewhere between 25-35 for most non-whites, and in all cases keep your PTH down around 30 or below.
For vitamin A this is less clear, because serum retinol is the only marker and it has its caveats. However, I think you want your fasting serum retinol close to the middle of the reference range. And a good baseline is probably to get 3-5000 IU/day as retinol, with lots of red, orange, yellow, and green vegetables to supplement with this. But if you have dry eyes, dry skin, hyperkeratosis, or other such problems you may need more.
I think you can follow my K2 recommendations here without that changing the others.
For vitamin E, you do not want to megadose K or E without megadosing the other. But the doses recommended herein are not megadoses and I don’t think you have to worry about E at those doses.
Chris
Thank you for putting the time and effort to educate others about this! I enjoyed the infographics that summed up everything for the visual learners. I know I can rely on your page for any research-backed information about nutrition.
You’re welcome Mindy! Thank you for relying on my page. 🙂
Thanks so much for this resource! I really appreciate all the work that you do and am stoked that you’re producing this kind of content now. It’s awesome.
There’s a K2 supplement from a popular and respected Canadian brand that you could add to your supplement review. AOR makes a 120mcg MK4/MK7 blend available in softgel and capsule. It can be a little pricey (though perhaps not in US$). The capsules are usually around $25 (60cap) and the softgels around $30 (also 60) in most stores. MK4 is from pharmaceutical synthesis and MK7 from natto.
https://www.aor.ca/en/product/vitamin-k2
https://www.aor.ca/en/product/vitamin-k2-softgels
Available online (and usually on sale) here: https://www.nationalnutrition.ca/SearchResult.aspx?KeyWords=aor%20k2&All=True
All the best!
Thanks Jay! I’ll check it out for the next round of revisions to the supplement review.
Chris
Hi again,
Thanks for checking this out for your update! Some may be interested to know that in Canada the maximum amount of K2 allowed in an over-the-counter supplement is 120mcg. That’s probably why AOR’s low-dose MK-4/7 isn’t available to order online except from Canadian distributors, and the 15mg MK-4 product (and other high-dose K2 supps) is not available in Canada.
Kind regards,
Jay
Interesting, Jay, thanks for the explanation.
What did humans find vitamin K before cheese and natto were invented? Is it at all possible to reach healhy levels without those foods?
They probably discovered pretty quickly to make both and the benefits of eating both.
Plus theres eggs and goose liver that they ate Im sure.
Ula and Hélène,
Plus there are probably a lot of local and culture-specific foods that are very rich in it. Imagine if you were eating emu oil as a food rather than supplement. Very high. Some organs that aren’t in the database like brain are very high, which we know from looking at rats. Goose is probably one example of livers that are very high and there are probably others.
Weston Price’s research on traditional diets is very interesting here because you see that each culture had accumulated wisdom about hard-to-get foods rich in fat-soluble vitamins that they prized and put special effort on procuring.
We are biased because we have a very generic view of what can be eaten, so we take out cheese and natto and it looks like there isn’t much left.
Chris
When I was a child, my dad used to kill a pig sometimes and we did have the brains. But it was only one small meal for the whole family every few months. So if you eat all the eggs, brains and livers you could realistically get your hands on (eating the whole animal), will that be enough? I come from Poland and we do not have emus here.
Hi Olivkah,
According to Wikipedia’s list of Polish cheeses, they have been made in Poland for almost 8,000 years. So, I think if you were to look at K2-rich foods in the traditional Polish diet, cheese would be important.
I don’t know if all the eggs, brains, and livers would always give you optimal K2, but it would certainly help.
Chris
Chris,
Great article! I have been taking Life Extension’s Super K with Advanced K2 Complex, is this too high of a does for everyday use?
Supplement Facts
Serving Size 1 softgel
Amount Per Serving
Vitamin C (as Ascorbyl palmitate)
10 mg
Vitamin K activity
2700 mcg
From:
Vitamin K1 (as phytonadione)
1500 mcg
Vitamin K2 (as menaquinone-4)
1000 mcg
Vitamin K2 (as menaquinone-7)
200 mcg
https://www.lifeextension.com/Vitamins-Supplements/item01834/Super-K-with-Advanced-K2-Complex
Hi Erik,
I reviewed this in the comprehensive supplement review. Just click open the detailed box after the section “The Three Best Supplements…”
Chris
Hi David
Yes that is the exact timeframe for us too! Takes 3 days before the nasty symptoms (severe insomnia, anxiety and jitters with palpitations) subside. I’m a devil for persistence though and keep tweaking all our supplements and then trying again! Having dairy and soy allergies is the pits! I’d much rather we were all gorging ourselves on Edam and natto.
Anna
Hi Anna,
Given the time period for decay of symptoms of three days, I think it is much more likely that a supplement has MK7 in it than only MK4. It is also possible you are reacting to the other components in the pills. Try a different reputable manufacturer of MK4 only pills and see if you get the same results. MK4 is part of the evolutionary development of all mammals so it would be really unusual if you were reacting to it
David,
I agree that your suggestion of a different MK-4 supplement to test for contamination makes sense.
However, I don’t see a basis for the time decay of symptoms comment unless you are referring to half life in the blood, but why would symptoms be driven by its presence in the blood?
Perhaps you meant something else, but without knowing the mechanism of side effect there isn’t a basis for estimating the time it will last for based on the form of vitamin K.
Most MK-4 supplements have doses higher than what any mammal would eat in most diets, so there’s nothing particular strange to reacting to it.
But the safety of high dose MK-4 suggests side effects of even those high doses are only a few percent. But blog comments are not a random sample of the population, so it wouldn’t be unusual to find comments about unusual reactions in blog comments.
Chris
I primarily agree with your statements! This case could be due to anything. My best thought is since the symptoms in repetition take about three days to dissipate, fully resemble MK7 sensitivity symptoms, and this is the half life of MK7 in the blood, one easy theory is that the MK4 supplement is contaminated with some MK7 and the individual is sensitive to that MK7. Changing the source to another MK4 only pill should prove if this theory is true. But their symptoms fully suggest those of MK7 in an MK7 sensitive person.
David,
I think we are agreed on many things, but I don’t know of any condition named “MK-7 sensitivity” and I’d like to see some support that it is more than a collection of anecdotes about side effects from MK-7 supplements.
Chris
Great resource. Thank you! Could you add the liverwurst from us wellness meats. I think it is a combo of different kinds of offal.
Hi Cora,
Thanks! I’d love to see what’s in it, but to my knowledge no one has measured it. If someone does, I’ll definitely put it in the database!
Chris
Thanks so much for this thorough and great article. It looks like you have too many comments to respond to, but I was trying to figure out if the supplement I’m taking is equal to the ones you recommend, or if I should look into switching. I’m currently using Life Extension Super K with Advanced K2 Complex, taking one a day. I’m wondering if it’s too high of a dose for a healthy and healthy eating person.
Hi Nancy,
I reviewed this supplement in the “comprehensive review.” You can click it open using the green box underneath the “The Three Best Vitamin K2 Supplements” section.
Chris
Aha, thank you!
This is an incredible resource ( I feel guilty not paying for it!) And the podcast was so, so informative. I give osteoporosis lectures at my Pilates training centre in Paris (and, I have osteopenia myself) so will be listening to it over and over to try and understand more about this complicated subject. Thank you so much
Thanks Marjean! When I release something that costs money you can pay for that. But I’ll keep pumping out free stuff too. 🙂
Also, remember that anytime you shop on Amazon, to click through one of Chris’s links and he will get some revenue.
Chris, it would help me and others do this if you put a top level menu item for this.
Hi ReneeAnn,
Thanks!
I want to be nice to my users and not clutter my top menu with requests for money. However, since you asked I made a special link that you can use and share with other people that I hope is roughly just as convenient:
chrismasterjohnphd.com/amazon
It should be super easy to remember and it goes right to the Amazon front page. 🙂
Chris
Great information!
Which is best, -trans or -cis forms of mk-4 and mk-7? Other than price. 🙂
janusz
janusz, they should be all-trans.
I could not find k2 supplemental studies during pregnancy, any advice on that subject?
Harmen,
I don’t have specific advice that would differ from non-pregnant women and adult men.
Chris
Heĺlo,
What about the Vit K shot given to new born babies?
Hi Leonie,
Could you please try asking a more specific question?
Thanks,
Chris
This is a wonderful educational presentation.
THANK YOU for all your hard work.
I learned a lot of very important info.
You’re welcome, Barbara!
I am a home birth midwife and Chapter Leader in Georgia. I’ve been intrigued by this since I read “Vitamin K and the Calcium Paradox” years ago. I recommend (strongly) all my clients take d3 and k2 in addition to pastured liver (tablets if necessary), eat pastured butter and lots of eggs, lard, tallow…all things the industrial medical model obstetrics tells pregnant momma to avoid! This whole article and the graphics and the links…I can’t wait to incorporate them into my client packages and my Chapter meetings! Thank you!
Thanks Cindy! You’re quite welcome!
Chris
Any thoughts on K1 food recommendations for people that are Factor V Leiden hetero or homozygotes? Should certain leafy greens be limited in the diet?
Hi Dan,
The genetic issue does not affect vitamin K intake. The treatment does. Anyone on warfarin or any related 4-hydroxycoumarins must limit their K intake and adjust in under supervision of the prescribing physician. Treatment with anticoagulants that do not work by inhibiting vitamin K metabolism does not require vitamin K restriction and supervision. So, it’s all about the medication.
Chris
I was thinking primarily about a person who is heterozygous, as opposed to homozygotes which are usually identified fairly early through some type of adverse situation and are placed on lifetime anticoagulant therapy. The newer classes of drugs such as the Factor 10a inhibitors, which I take, are a double edged sword IMO and a worry for ER physicians justifiably so, I believe, because there are no current approved reversal agents for them as opposed to Coumarin/Warfarin. and intravenous vit K. I have simple R.A.T.S. tourniquets in the house, in the car and on me all of the time as about the only precaution I can take to aid myself in the case of some type of accident that can go from bad to worse quickly simply because of this tiny little tablet I take every day. My main concern for heterozygotes, particularly if they are undiagnosed and have no clue about their condition is that if they are trying to be better about their diet and they incorporate a large amount of dark green leafy vegetables as part of their new diet do they increase their overall chances of an adverse clotting event because of this new intake, or even if they have always eaten dark green leafy vegetables does their overall odds of an event increase simply because of age since age seems to be just about the leading indicator for so many diseases and conditions we know about. It’s been quite a while since I have studied the hemostasis cascade though and that’s why I wanted to find out if there was any known connection between increased vitamin K intake, in any form, and an increase in adverse clotting events in a person who produces some portion, or all, of their Factor V in Leiden variant. I’d like to find a good comprehensive hemostasis cascade resource that incorporates all of the most up to date molecular mechanisms if you know of one. I’ve often wondered if anybody ever actually came up with a way to directly assay Factor V Leiden from a venous sample. D Dimer seems to be the current most useful analyte for working with FV at the moment with the ELISA method seemingly the most touted gold standard test even if almost nobody is performing it.
Thanks!
Hi Dan,
Please try to break up your text into paragraphs. It’s difficult to read text this long that isn’t, especially on a screen.
I don’t see anything in what you wrote to see a reason why this should be a concern. Vitamin K is not a coagulant. It’s only relevant to people on coumarins for the singular reason that the mechanism of action of those drugs is to cause a vitamin K deficiency. Vitamin K in that case does not cause any other harm except to reverse the vitamin K deficiency.
I don’t know that much about factor V leiden, but from what I do know I don’t see how vitamin K is relevant in someone who isn’t deficient and isn’t on a coumarin.
I don’t know of a comprehensive resource on the coagulation cascade. I would imagine you could find something by searching pubmed with the right keywords or looking for a recent edition of whatever the leading hematology textbook is.
Chris
I don’t understand why my comment of 12/9 is still awaiting moderation when there are newer comments that you have replied to.
Hi Harry,
Sorry, the system keeps some comments for moderation and lets others through according to an algorithm that predicts the likelihood of spam, and there was a glitch in the back end of the site that prevented some comments that were pending moderation from being seen.
Chris
Hi Chris
Thanks for this. So helpful for me and my patients. I love the format and illustrations. So easy to read, comprehend and page through when referencing it again.
Rosann Volmert DO
Thanks Rosann! You’re welcome for it. Ease of use was definitely one of my top goals, so I’m glad to hear the positive feedback on it.
Chris
URGENT!!
Thanks for all this. It came at an interesting time since just TODAY i was told by my doc that my pre-op blood K came back high. I am scheduled for nose surgery Dec 28 and for the last month i have increased my Thorne D/K to about 4000IU to get my D up. I didn’t realize that also meant a very high dose of K – 800. I guess they put you on blood thinners during the surgery so this puts me at risk. 1- do you think in 10 days the results will improve? 2- do you really think i am at risk?
THANKS!!
Hi Susan,
1) Yes, it should absolutely resolve within 10 days if you stop the supplementation.
2) Please discuss the risk with the physician and not with anyone on the internet.
Chris
Wow, what a great post, thank you for your time & energy Chris! I do wonder about this K2 in food content, and I know there hasn’t been much research done in finding the exact amount in all the foods, but could I assume other ruminant’s meat (ex lamb, mutton, venison) will have pretty much the same content of K2 as beef does? I ask cos due to where I live lamb & venison makes up the majority of my meat intake. Thanks again 🙂
Hi Rob,
It’s a reasonable guess, but even different samples of beef are likely to be different depending on the diet of the animal.
Chris
If MK-4 boosts sex hormones and fights cancer, what about breast cancer that is estrogen/progesterone positive. Seems like MK-4 could encourage cancer growth instead of inhibiting it. Or does MK-4 stop conversion of normal cells to malignant ones but have no positive affect on cancerous cells? er+/pr+/her- breast cancer is treated with aromatase inhibitors such as Arimidex to prevent production of estrogen by the body. Is there any effect of vitamin K on this treatment?
Hi Nancy,
We can only guess. MK-4 increases testosterone production through direct actions on male gonadal cells, and inhibits the growth of cancerous cells derived from a number of different cancerous lines. Any vitamin K that reaches bone improves insulin sensitivity, which impacts other hormones. How all this would play out to affect the amount of estrogen and the profile of different estrogens in females, combined with the direct effect of MK-4 on breast cancer cells, is not known.
Chris
Hi Chris,
Nice post.
Was wondering if my Thorne Research K2 that has expired a year ago, kept in dark shelf, still do the job?
I’ve been taking intermitently with their K2/D, but found my D 25-OH to be insufficient (22ng/mL)
Chris
Hi Christoph,
I think if it was kept out of light it’s probably stable. However, I don’t know as I haven’t seen data for the stability of vitamin K over the course of years.
Chris
Hi Chris thanks for some great info. Wish these sups available in U.K.! I can’t get search to work but maybe it’s me
Hi Aud,
Probably due to a slow connection combined with my slow server. I’m on a faster server now so I’d try it again. It loads much faster now.
Chris
Thanks Chris. This is a great companion to Kate’s book The Calcium Paradox. I currently supplement with 400 mics of NOW MK7. Thinking of adding an MK4 to round it off. I need to have another in depth read of your article.
You’re welcome Anne. Read it to your heart’s content. 🙂
A really fantastic post and thank-you so much for sharing all your hard work and research on Vitamin K with us. Much appreciated.
Thanks for your appreciation, Kathleen, and you’re very welcome.
hey doctor nice job, i am brazilian and In my country there are many manipulation pharmacies and I would like to know if the ratio of mk4 and mk7 would be 80% and 40% respectively
80 and 20%
Leonardo, there is no evidence to support any given ratio.
Chris
Hi and thanks!
I’ve heard that the half-life of bisphosphonates is long: their effect may be exerted long after the administration has ended. Is there a similar long period with statins? Also: up in Canada we have access to the reasonably priced brand, Natural Factors. Do you have any comments on their product? (I order a half-dozen at a time: for my family and one friend)
Hi Barb,
I don’t know what the long-term effect of statins or bisphosphonates is on the conversion. It’s been studied at the cellular level rather than in humans taking the drugs.
If you can link directly to the specific product, I’ll include it when I update the review section.
Chris
Thanks Chris! I’ve now had a chance to enjoy the k2 podcast (it will require _at_least_ a second listen!) My mom was on bisphosphonates for 20 years and statins for less. I guess I’ll just try to make sure she has some MK-4 along with the MK-7 I’ve had her on. The MK-7 brand I mentioned is promoted at https://naturalfactors.com/product/vitamin-k2/ and I pick up 90 100mcg caplets for CAD$15 (~ USD $11.50)
oopth! please correct: That’s 120 (not 90) capsules (not caplets, if that makes a difference)
Thanks Barb, I’ll cover that one in the next set of revisions to the supplement review. Glad you enjoyed the podcast!
Chris,
Great post!
Question: There is a lot of research that suggests that Natto can lower elevated blood pressure because it contains compounds that are ACE-I (Angiotensin Converting Enzymes Inhibitors). While this is good, I take ARBs (Angiotensin II Receptor Blockers) for blood pressure reduction and their seems to be some reports then warn against taking ACE-I and ARBs together.
Should I stop eating my daily Natto while on ARBs?
Bill
Hi Bill,
I don’t know the answer to that, and I think you should discuss any potential interactions with your medication directly with the prescribing physician.
Chris
Hi Chris,
I enjoyed meeting you and hearing your lectures in Montgomery. Thank you so much for this article and for the format. This format is an exceptional way to communicate. I often skim articles and hope I don’t miss something important. With this format, I read the whole article completely, only opening one in depth section that I was particularly interested in, and was confident that I came away with all of the major points you were making. I hope you will use this format often. Thanks for all of your work.
Hi ReneeAnn,
That’s exactly what I was going for with the format, so thank you for your feedback. I will definitely do it more often, though producing something of this magnitude takes months. Just weeks going into the formatting, though hopefully once we have a system up and running we can work more efficiently. Still, I think this will be maybe a 4x-per-year thing. Let’s wait and see what the new year brings. 🙂
Great to meet you too!
Chris
Awesome article Chris!
I am curious why did they use high doses of MK-4 in the osteoporosis trials when you say MK-7 is the type favored for bone health?
As far as dental health is concerned, is it strictly in teeth mineralization? Any influence on plaque accumulation on the teeth? Also I believe I heard quite long ago that oral health mimics vascular health in the body; so if you build up a lot of plaque on your teeth it would be the same in your arteries and veins? Any truth to this and would higher MK-7(or MK-4) doses reduce dental plaque buildup? I eat a largely clean primal style diet but always seem to build up a lot of plaque on my bottom 4 teeth…
Thanks for the awesome resource!
Hi Dan,
The osteoporosis trials are not related to the nutritional effects of vitamin K, which is what this article is about. They used supraphysiological doses of MK-4 as an osteoporosis drug.
I think the effects on oral health probably include modulation of the microbiome, and much of that is probably mediated by MK-4 in saliva. Unfortunately, its role in dental health is profoundly understudied, and that is due partly to the profound resistance of dental medicine to thinking nutritionally.
Oral health does correlate with vascular health, but I don’t think you should make assumptions about your vascular health on the basis of your oral plaque.
Chris
When I take high dose K I have minimal plaque/tartar. Hygienists notice.
Curious, what form of Vitamin K do you take, and in what dose?
Great article! I did not know about the gene expression difference or mk-7 going to the liver. Mk-4 is usually larger because it has a much shorter half life. I take Relentless Improvement brand from Amazon. It has 15mg of mk-4 & 60mcg of mk-7. I usually take 1, but sometimes 2 per day.
David,
Thanks!
There is insufficient evidence to say MK-4 is needed in larger doses, and the half life is not relevant. I go into great detail about this in the click-to-expand section under “Why the Form of Vitamin K You Eat Is So Important.”
Chris
I’d like to let you new about a new vitamin K2 product (vK2). It contains pharmaceutical grade MK4 (5mg) + MK7 (100mcg).
If the brand of Vitamin K2 you take is NOT yellow, then its not pharmaceutical grade and probably contains Chinese ingredients.
Chris –
Very innovative design. I am not sure what kind of feedback you are looking for, but here are a couple of thoughts and questions:
– I agree with Noora’s suggestion that a pdf of this page would be nice. Maybe something to think about as you write other pages
– I think you might want to define what you mean by shareable link. Copyrighted material but Ok to post to another web page or document?
– you might want to add upfront rhat the Share widget is in the header. Since the images are fairly long, if you scroll down to the middle of an image and then start clicking it thinking some kind of Share option will appear, you don’t see the Share option because you can’t see the header
– I agree with comment that the database might work better in a separate tab
– I don’t think you need the first green oval/button that opens up the green ovals for Biochemistry and Evidence.
– wow, those detail sections are long! I think any detail sections over 3-4 vertical screens worth should open up as a separate tab. A reader halfway through the Biochemistry section has to click way too many times either up or down to close down this section and go back to the simpler content. Maybe all the detail sections should open a new tab if they are going to be long.
– I expected when I closed the detailed explanations that if I clicked on Close at the end that they would be collapsed again. But when I opened again, it looks like both Biochemistry and Evidence were both open. If I just wanted to go to Evidence, I had to search or click a bunch. Maybe add text under each button “Click button to close detailed information.”
Hope this feedback is helpful.
Peter,
Thank you very much for your feedback.
Making a pdf is not a priority but might happen eventually. This is designed for interactivity and is not all that amenable to a pdf version.
“Shareable” refers to function, not prescription. I’m not telling you what is permissable. It is literally shareable because you can click the share button. There are one-click buttons to share to social media, and there is embed code to embed the image in a blog post or web page. If you do so, please use the embed code and please do not take a picture or screenshot of it. The graphic contains links back to this article.
Good point about alerting to the location of the share button. I’ll think about how to best revise the text by week’s end.
Thanks for reinforcing the new tab idea. That might happen by tomorrow.
I see your point about the two-nested feature at the top but honestly I think it makes little difference one way or another. The current way provides more consistency, so I went with that.
I respectfully disagree about the new tab for the detailed section. The fact that they are in gray boxes makes it incredibly easy on any device to scroll to the top or bottom in seconds. I have tried this on desktop and mobile and it is extremely easy. By contrast, opening in a new tab would be a real pain on mobile. I’m also not sure how to do that without making a different web page, and that hurts search ability on search engines. I also don’t like how it would reduce the smoothness of the design.
On your last point, I’m not really sure what the problem is. If you close the big nest but not the little nest, you open back up the big nest and it is just like you had it. It’s very intuitive. If you have a box that you left a mess and you put it in a drawer, you open the drawer and the box is still a mess. If you neatly close it and put it back in the drawer, you open the drawer and it’s neatly put away.
Anyway, good to have the discussion on all these points. Thanks for the feedback!
Chris
Chris – agree that the detailed sections scrolling versus new tab works much better on phone. I wasn’t thinking about mobile.
Thanks Peter! The majority of people who read my site do so on mobile. In fact, the most common operating system is iOS at 36%, which has a major lead over Windows at 28%. I will never again produce content that doesn’t treat mobile as more important than desktop. But, I don’t want my desktop people to be left in the dust, so I try to make it a very close #2. 🙂
Peter, the database now opens in a new tab.
Thanks for such an insightful post! If I take the Thorne Research MK-4, should I ALSO be taking the Nested Naturals in order to also get MK-7? I just ordered the Thorne online based on one of your older K2 posts (before this one was published), and I’m wondering if I should take it alone, combine it with the Nested Naturals, or try to return it and buy the Innovix. Thanks!
Hi Kay,
Innovix is simpler and I’ll probably switch to it when my bottle of Thorne is out (which takes forever!), but yes I think combining Thorne and NN makes sense.
Chris
Thanks, Chris! I ended up cancelling the Thorne order and going with the Innovix.
It would be amazing if you created a resource like this for Vitamin D! 🙂 There’s so much confusing info out there on whether/how much to supplement, especially if we’re already taking FCLO.
Kay,
Great idea! Can’t wait to do more like this. 🙂
Chris
Thanks Chris for this well-resourced, informative and exhaustive resource!
Much appreciated.
I have a few questions that you might be able to answer.
1) The Mercola starter kit does not contain any Bacillus subtilis (Bacillus natto). How is this starter supposed to help produce vitamin K2?
2) Are the values in the database single measurements or the averages of multiple measurements? If the latter, do we know anything about variance?
3) Given that many in the WAPF/paleo/Primal/ancestral/PHD community tend to eat animals from head to toe, is there any chance you could expand the Offal section of the database with things like bone marrow, gizzards, spleen, brain, testicles, tripe etc.?
Hi Zoltan,
1) I reached out to Dr. Mercola for more documentation on this and haven’t heard back from him yet. I’ll update the article if and when I do. In the mean time, I’m not sure the answer to your question, but there is not only one bacteria that makes MKs.
2) Sometimes, sometimes not. When *we* took averages, we reported that in the title. But we didn’t record details if averages were reported in the literature. However, in every single circumstance you can click “view more details” and obtain the reference from which the data came, and look at the original source yourself to satisfy any questions you have about an individual measurement.
3) I will expand the database with new data as I obtain it continually. Some extra measurements will be in tomorrow. For some of these, you probably have to guess based on rat data, and I’m not sure about how to put that in the database but I’ll think about it.
Chris
Thank you! When you mean rat data, are you referring to this study?
https://jn.nutrition.org/content/138/3/492.long
Zoltan, no, not specifically.
The infographics aren’t displaying for me. Is it just my computer or has something gone wrong? I really like the visual aids. 🙂
Hi Diane,
It may be your connection, but it could have been a transient disappearance while they were being edited or something as well. Try again and see. If the problem continues try on a different browser or device and see if there is any trend and let me know. Everything is displaying for me.
Chris
Hi there Chris
Got your details via Mark Sisson’s website “Marks Daily Apple”.
I couldn’t spot a review of Natural Factors K2. I think these are recommended by Dr Kate Rheaume-Blueu.
Also, it’s a shame there is no test for vit K2 levels. As an alternative, is there a blood test for calcium available? If there is high calcium in the blood stream, would that indicate it’s not in the bones where it should be?
Regards
Hi Charles,
No, serum calcium is tightly regulated and that would not be useful here.
Thanks for the supplement recommendation. I focused on ones that made it easy to get 200 ug without additional nutrients. However, due to requests, I will include this and others in the next round of additions later this week.
Chris
Hi Chris,
Does the length of the aging/ripening process matter in terms of K2 content? I noticed that for Jarlsberg cheese, K2 was 74 mcg. However, this seems to be based on the original type which is aged about 3 months. Recently they have introduced another type («special reserve») which is aged for a minimum of 12 months.
Unni
Hi Unni,
Apparently not. I discuss this in the click-to-expand section under how to get it from foods, and that can also be seen in the database by comparing values for gamalost of different aging values.
Chris
Thank you so much for this amazing resource! I am so excited to have all of this information put together in such a user friendly way. Definitely sharing this valuable info with our readers too! Thank you again!
You’re welcome, Mandy, and thank you for the appreciation and for sharing!
Chris
Hi Chris!
This is a wonderful article! I REALLY appreciate your thoroughness along with your clear communication! The graphics are excellent!
So my request is that you do a thorough investigation and explanation of Vitamin A. It seems to be overlooked because people equate the carotenes with vitamin A in the body. I am hypothyroid and I found out (after trying to get my A with palm oil!) that I just turn yellow. Currently I’m taking a supplement as well as consuming a pound of beef liver weekly. I’m just very interested in getting the word out about how essential vitamin A is!
Hi Kathy,
Maybe an ultimate vitamin A resource is on the horizon. 🙂
Chris
Beef liver is also very high in copper, about 12 mg per 100 g, so a lb is about 50 mg, which means you’re getting over 7 mg/day of copper, just from the liver. Some people need higher doses of copper, but for most people this is a higher intake
than is needed.
Dr. Masterjohn, this is a wonderful summary of a very complex subject. I only subscribed to your blog today. This is some your best work. I was becoming somewhat disillusioned with the podcast, due the complexity, not that one should overly simplify a complex subject. I was about to need “Biochemistry for Dummies”. However, the way you present the subject matter(a la the graphic novel approach), allowing the reader to dive as deep as needed is a stroke of genius. Keep up the good work, it is very much appreciated .
Thanks Linda! I will continue refining to make my stuff as accessible as possible yet as satisfying as possible to people with a deep hunger for detail. Tough to balance but I’m glad that with my first true attempt at it I’ve gotten so much positive feedback.
Chris
Any thoughts on someone with factor five leiden supplementing with K2. Having trouble finding any info on this.
Kathy,
If it is treated with warfarin or another 4-hydroxycoumarin supplementing with vitamin K must be managed by the physician and is completely unsafe to use without such oversight.
Chris
If you are being treated with warfarin to avoid potential blood clots, this can not be combined with vitamin K2 unless the doctor does the extra work of including that in his calculations of the INR. It may be a better choice to go to a non-warfarin blood thinning drug that functions by a separate biological pathway and would be safe to use with vitamins K1 and K2. Long temr use of warfarin also reduces production of MK4 vitamin K2 in the body with a resulting combination of bone loss and increased artery calcification. The doctors references will note this side effect which is prevented by vitamin K2!
David,
Harder than it sounds in many cases, but, agreed.
Chris
What if you are already being treated with a blood thinner that isn’t a vitamin K antagonist? Apixaban (Eliquis) springs to mind but there are others too. And of course there are people on low-dose aspirin or other antiplatelet medications.
Is taking vitamin K in general, or vitamin K2 in particular, safe in these cases?
Zoltan,
Well, you shouldn’t make any medication-dependent decisions without discussing them with the prescribing physician, but, in short, yes. Vitamin K is not a coagulant. It only impairs the anticoagulant effect of anticoagulants whose mechanism of action is to cause a vitamin K deficiency. In other words, vitamin K interferes with deliberate induction of vitamin K deficiency.
Truly exceptional! This is the best review of vitamin K I have yet encountered. Really brilliant. Thanks a lot for investing the tremendous amount of time and energy you have had to in order to produce this. Really, hats off, and thanks a million. I’m going to re-blog the link to this resource for my followers.
Thanks Guillaume! I appreciate both the props and the shares.
Hi Chris, I’ve always enjoyed your articles, thanks so much for all of your work. This one was great. I was really excited to check out your database for K2 and quickly typed in “kefir”. No results. I’m an avid fan of kefir and make my own, have had the same culture for several years now. It seems to me that kefir should have a good concentration of K2 but I haven’t seen any data, just speculation. Have you ever seen any?
Hi Deb,
Thanks! Unfortunately I haven’t seen kefir data but if I obtain some I will add it to the database. Just because it’s fermented doesn’t mean it’s rich in K2 but I’m sure it has at least some.
Chris
Wow!! Another great Masterpiece from the Masterjohn! I really appreciate the work you put into your research and presentation! On any subject I research and chase down all the various rabbit holes I go to you first due to the trust I have in your vast knowledge! Besides by sharing your website and podcasts with as many people as I can to show my appreciation for all your hard work- I feel they all need to learn from the best source available- Keep up the awesome work!
Thanks Eric!
Hi Chris, great stuff! Love the work you do. I was wondering about the vitamin K shot for babies and why that is necessary nowadays? Is it an abject lack of vitamin K in mothers’ diets or an inability for it to cross placenta and/or get into mother’s milk? That’s the story I’ve heard but wondering if you’ve come across anything?
Thank you!
Lawrence
Hi Lawrence,
Vitamin K does cross the placenta and make it into mother’s milk, so I think it is about the vitamin K status of the mother.
Chris
This is the information I’ve been looking for. I’m writing my thesis on nutrition and fertility, and I’m about a month away from having a baby. Yesterday while trying to research vitamin K and fertility I got caught up in the war of opinions re the vitamin K shot for newborns. This is my fourth child, and I didn’t have any of my other children receive the shot, but it’s really weighing on me this time. I’ve been taking Thorne K for a while, since before I got pregnant, so I *think* we should be ok. But there is A LOT of buzz about whether K actually crosses the placenta or not. One study says that fat soluble vitamins do cross, but very poorly… And people use this as proof that they do cross. That’s great, but… poor is poor. What else can you give me, folks? Can you point me in the direction of research on this? I found one study from Japan showing that for at risk babies supplementing mother’s was sufficient prophylaxis. So what’s the deal with the research? I’m going a little crazy here.
*supplementing mother’s of babies at risk of vitamin K deficiency bleeding was sufficient prophylaxis for the at risk babies
Hi Chris, I’ve bothered by the tone of my comment yesterday. It sounds accusatory, and I certainly did not mean to accuse you or your team of anything. When I said “folks” I was referring to conversations I’d been reading around the internet. I am frustrated, but not at you. I appreciate all of the hard work you’ve always put into your writing. I’ve been a big fan since 2010 when I was introduced to your work. Thank you for all you do!
Sorry for the late reply and thanks Melissa!
Hi Chris,
What’s your recomendation for amount of k2 to oral vitamin D?
I’ve heard 100mcg of mk7 for every 1000 Iu of oral D and if it’s MK4 how much per 1000IU
My understanding is taking vitamin D creates more K2 dependent proteins , thus requiring more k2
Thank you,
Chris
Hi Chris,
I’ve never seen any data that could support such recommendations. The principle is true, but I don’t think that has been sufficiently quantified in any way to yield practical insights, and there is no obvious reason it should be expressed as a ratio. At the present time, I think it is better to get a couple hundreds mcg K2 and to optimize D with 25(OH)D and PTH.
Chris
Its true that taking more Vitamin D3 tends to create more calcium handling proteins that require vitamin K2 to function. This is the basis of many successful MK4 research trials in giving 1000 or 2000 IU of vitamin D with vitamin K2 to improve the results. This is not the only factor in vitamin K2 dosing. Several things reduce body production of MK4 vitamin K2, so the personal needs and rates of MK4 dosing can vary greatly. Taking steroids or warfarin shuts down MK4 production. Being stressed by anorexia, age, or athletic over training reduces MK4 production. Marathon running enthusiasts who run every day for four months instead of taking rest days each week are known to get stress fractures in their legs and are probably tanking their MK4 production. So personal MK4 requirements vary more than requiring any simple proportion with vitamin D.
I have mild osteopenia and take Bone Restore from Life Extension which includes K2. This allowed me to drop a separate K2. Any opinions on that?
Julia,
Looks pretty good to me.
Chris
Great Article!
Thanks Karl!
Great post Chris!
Super well explained as always!
Do you have any information about Emu Oil as a MK-4 food source?
It looks like that there is another full spectrum of vitamin K2 available on Amazon https://smile.amazon.com/gp/product/B018FARO4G/ref=oh_aui_search_detailpage?ie=UTF8&psc=1
Have you heard about this one?
Thanks.
Thanks Hena!
As a food oil emu oil is very rich in MK-4. As a supplement, it is low per capsule. Four tablespoons provides 200 ug.
Thanks for pointing out the supplement. This week I will update the supplement review with some of the ones I’ve missed that people are requesting.
Chris
Hey Chris. Amazing work as always! I know you’re planning on adding emu oil in the food section, so curious if you recommend that as opposed to synthetic supplementation. I’ve been taking about 3 capsules of Walkabout emu oil a day, but that’s probably only the equivalent of one tablespoon, maybe.
Hi Chris,
I think it is a great product. It takes 4 tablespoons to yield 200 ug, so three capsules, while beneficial, shouldn’t be seen as a total K2 source.
Chris
Have to imagine 3-4 capsules is probably about 100ug or so? I usually eat 1-2 pastured egg yolks per day, some hard cheese, often dark chicken meat and some fermented veggies. Just trying to decide whether or not to ditch the emu oil and go with Thorne K2. Not sure you ever disclosed, but curious how you get your K2! Thanks as always!
Chris,
No, 3-4 capsules is nowhere near 2 tablespoons. There are about 4 ug per capsule.
I think if you eat a lot of natural K2, and you don’t have a history of ill health effects that come from inadequate K2, then I would go with the natural emu oil and the collection of K2-rich foods. But, if you have reason to think you have a very high need, then you might want to take a concentrated supplement like Thorne.
Oh wow, thanks for this info. Walkabout makes it seem like their emu oil is absolutely packed with K2. I already ordered Throne K2, so perhaps after a while of supplementation with 200ug I’ll go back to it.
Assume there’s no risk in one drop of Thorne K2 per day? Or is that overkill long term? I saw Kresser recommends a drop per day as a maintenance dose. (Last question, I promise!)
Hi Chris,
I think it’s a little overkill but I often use that dose and I’m not worried about harm. I will probably try the Innovix when my Thorne runs out. The emu oil is very packed with K2 as far as foods go.
Chirs
If you have the Thorne MK4 supplement that has 1mg per drop, but you want to take a smaller dose every day, presumably you could dilute it in MCT oil. For example, mixing 1 oz of Thorne MK4 (the whole bottle) with 4 oz of MCT oil would change the concentration to 200 mcg/drop.
Great point Nick. You just have to be careful about mixing homogeneously and avoiding exposure to blue light during the preparation.
Chris
Hello Chris,
I very interested in the role K2 plays with the immune system, particularly if there is any role in the body’s natural defense against biofilms perhaps by shunting calcium away from these structures.
Ugh, typos. “I’m”
Mackay,
Very interesting question, but not one I’ve studied. If you find anything on that post it here!
Chris
Excellent resource!
Surely, you are aware of the https://translate.google.com/ being able to translate Japanese pdfs to English like “Sato (2012) cited a Japanese paper”. Of course, this would take even more huge amounts of your team’s time.
My humble wish would be to get this resource information also as a white paper pdf if you are not interested to write a traditional review paper.
Thanks Noora!
I’m aware of Google translate. In fact, several papers that were critical to certain sections were very old papers I had translated from German about ten years ago using Google translate in one of its earlier incarnations.
However, the paper I linked to is not indexed for pubmed and I didn’t have the time to chase it down with interlibrary loan during the time course to get this out.
I do intend to publish additional iterations of this and so I can chase it down and update if need be.
I don’t intend to publish this in alternative formats right now.
Thanks,
Chris
About pdf:
Understood that your main audience is a lay person.
However, pdf would be the preferred source for academics for easy access to citations and tables of concentrations. Leading to hesitation of forwarding this to academic colleagues.
Hi Noora,
There are probably thousands of pdfs about vitamin K out there, and there are dozens of references within this to good reviews that are in pdf format aimed at academics.
Chris
Hi Chris,
Thank you for this valuable information.
Can you please comment on the Vitamin K content in duck liver?
In many areas ( in Canada), only duck liver is available .
Also, how much Vitamin K is left after cooking the goose/duck liver?
Thank you
Sanda
Hi Sanda,
Please check the database for duck liver. If you don’t see it there, we don’t have it right now. I do intend to add some more data in the next week.
Chris
Very many thanks. Comprehensive article. One minor niggle – can you keep to grams or ozs ( or put both) and could you please insert iu’s in addition to ug’s for us.
Thanks Dot, good point. I was trying to make the numbers easy to read and comparison wasn’t the purpose of the infographic, but a couple people mentioned that so I’ll think about the best presentation of that for the future. There’s no such thing as an IU of vitamin K.
Great info Chris.
Quick question about K2 for plant based folk (firmly setting aside any discussion of why whether ethical or religious or dislike).
Clearly your advocating meat but if for whatever reason you couldn’t access meat would natto or MK7 supplements and/or synthetic MK4 supplements statisfy your criteria? Perhaps a MK4/7 fortified Olive oil or algae DHA/EPA oil?
Many thanks
Brendon
Hi Brendon,
As with other nutrients such as vitamin A, some vegans will be good at the conversion and others not, making the final conversion product (MK-4) more reliable when present in the diet. To my knowledge, the only way to do that for MK-4 right now that is vegan is to use synthetics. I have included synthetic MK-4 supplements in the reviews and recommendations.
Chris
Thank you for all this information but if some one has probkem how can he take chease or egg or chicken the get k2 while docters recommend him not to eat proten
Hi Ghania,
You can eat the food, or you can take a supplement.
Chris
THANK YOU!! Really an ultimate resource page for K2. Thanks for your efforts and public service.
You’re welcome, Shafqat, thank you for your appreciation!
Chris
Chris, do not want to be alerted with regard to alerts, how to escape! Luv U but!?!?..
Hi Linda,
Sorry, but you’ll have to explain what your problem is in clearer terms.
Chris
Curious on the dosing of vitamin K if not done daily . . . does this still provide the same benefit? I understand the reasoning behind dosing daily for better adherence, but am curious if the body can still reap the benefits if dosed every few days as it appears K2 MK4 has a relative short half-life.
Hi Taylor,
The half life is totally irrelevant because vitamin K is used in the tissues from which it is taken up in the blood, not in the lipoproteins that carry it through the blood. On this, I recommend reading the click-to-expand section under “Why the Form of Vitamin K You Eat Is So Important” and reading the second subsection, “Side Chain Length and Saturation Determines Tissue Distribution” which covers lipoprotein transport.
No one knows the answer to your question as it hasn’t been studied. My inclination is that it is bioavailable, but I would prefer smaller doses on a daily basis because 1) it’s *possible* that more goes to the liver at higher doses, and 2) it’s *possible* that more menadione is generated in the intestines at higher doses, causing more spilloff into the urine as glutathione conjugates.
But, I suspect that there is plenty of circulation of in tact MK-4 to many extrahepatic tissues at 1 mg doses.
Chris
You are the man Chris! Thank you for your reply and information.
I had actually tried to find this information out and contacted a couple of manufacturers to which they could not address the question as effectively as you just did.
Keep up the good work, would love to see you continue this with other essential nutrients.
So many opinions out there it’s hard to find a reliable source. Your depth of knowledge and application of it is much needed in this space.
Keep up the good work!
Thanks Taylor! I don’t think supplement companies often have any clue what they are doing, based on the amount of BS in their advertisements. Either that or their chemists know what they are doing but don’t review their marketing department’s materials for accuracy.
Anyway, the information I put in there is NOT easy to find and had to be pieced together from a ton of different sources. I really appreciate all the love for this ton of ton of work I did.
Chris thank you for this super detailed post. I read that Emu oil was a good source of k2 and I think the WAPF tested this or were planning to. Any thoughts? It was the Walkabout brand that they seemed to be recommending.
Chloe,
Emu oil is great as a food oil and will be added to the database. As capsules, it’s a low amount per capsule. 4 tablespoons provides 200 ug. It’s a good product, but a few capsules won’t provide your complete needs for K2.
Chris
Cloe, emu oil is now added to the database.
Would cheese, egg yolk and dark poultry meat from factory farmed animals have any K2 in them; if any, would it be anything like the humanly raised, pastured animals that your numbers come from? Ppl always give these sources and say to eat them from quality animals. Never anything about K2 levels in commonly found animal, which is all most working American families can afford. We eat alot of these 3 aforementioned foods in fact…they’re great nutritious, cheap foods.
Hélène,
It is the opposite. Virtually all of the measurements are from commercial foods available in the supermarket. Search the database and you can find the content of any food you want. Presumably, pastured is better. But there’s no data on that.
Chris
Do you not recommend the fclo (with butter oil for the K2) anymore? I though taking this would butter oil would meet my K2 needs daily so with vitamin D, A and O3s daily needs met in the fclo, my fat soluble vitamins would be taken care of (We eat alot of nuts here and some grains, always whole, so vit E is good too) .
Was just surprised to not see the high vitamin butter oil listed as a food or supplement source.
Hi Hélène,
I think it’s a great product. I’m not recommending products in general here. I’m recommending an aim to get K2, and listing many different ways to get it.
For the butter oil, its measured K2 content is meaningful but rather low, and way too low to be listed as a supplement that can give 200 ug here.
However, it is very high in unidentified quinones. It’s possible those are other forms of K2 not measured, such as tetrahydromenaquinones. But I’m not going to list it as such until that is verified. So it would be cool to see it measured.
Chris
Your dosage recommendations don’t take into account the differences between MK-4 and MK-7, including the fact that MK-4 is eliminated more quickly. Please tell us more about how much of each you think we should be taking in supplement form.
Hi Jeanne,
I have indeed taken this into account very extensively, and if you read that section you will see why there is no evidence for the statement that MK-4 is eliminated more quickly. Please click to expand the detailed section under “Why the Form of Vitamin K You Eat Is So Important.”
Chris
First, thank you from the heart for this valuable information. And , for no charge is a gift.
I have He Familial Hypercholesterolemia. I take Crestor because I am finally convinced I Will live better longer with a particle number less than the original 2448. I also had a Calcium scan that revealed disease.
I studied Chris Kressers “High Cholesterol Action Plan” and take supplements as he recommends.
I drink raw milk Keifir, Kombucha and take a probiotic daily. I use a HFLC guide for food intake.
I’d like to think one of your supplements would help me regarding the station I take daily. Any comments/suggestions?
By the way, years ago at the WAP conference in Atlanta where I live , I asked your opinion of my total cholesterol of 430. You immediatly suggested FH. Thank you , because it was then I broke through the denial. It was really hard to understand how I could run so high when
I was eating WAP style.
So, I’d welcome your thoughts
Joan M Wills
Hi Joan,
I’m not entirely sure what you are asking me, but statins inhibit a number of important compounds including, as discussed in here, MK-4 synthesis, so you might want to include that as well as CoQ10. I’m glad to hear you got a handle on the FH!
Chris
Amazing resource…. very well done. Thank you for all the time and effort.
Thanks Garry! You’re very welcome. The time and effort was my pleasure.
Thanks chris.
I have a question,if pork is good source of mk4 then I see no reason that lamb or beef not being a good source.and they are ruminant so probably they should have more k2 than pork.
I know you mentioned pork because recently a reaserch came out about this,and there is no study like that on lamb or cow,but what do you think,are you agree with that logic?
Hi Payman,
Pork is mostly rich in MK-10 and MK-11, not MK-4.
Chris
Excellent post, very interesting, I did not know about Vitamin K until Richard Nikoley told me about it. This information is valuable far beyond the US (I’m French) it would be cool to have other sources than Amazon and other online stores, cause the shipping anywhere outside of the US will be super expensive. Can it be found in vitamin stores line GNC or Vitamin Shoppe or will it be crap ? Thanks !
Hi I use http://www.iherb.com to purchase some supplements from the US, but not all brands are allowed to ship overseas. Other way it is find a third party to purchase what you need and see if they are prepared to ship to France or whatever. I am in Australia.
Hi Philippe,
If you find the same brand at GNC or Vitamin Shoppe it should be the same. What online retailer do you recommend that works well for France?
Chris
Excellent, Excellent, Excellent 🙂 I would like to know if pasture free range Duck Eggs not just hens eggs are a valuable sorce of K2 MK 4, I choose Duck Eggs as the farmer I purchase eggs from at the farmers market (UK) raises both. They tell me stories of how the hens and ducks play around and hide sometimes when they are called to come in at night so a definite good source but I still feel that ducks are more likely to forage and eat grass where as the hens diet will no doubt be supplemented by some grain. I appreciated that in your post you pointed out the fact that the darker/brighter the yolk, then the more K2 the egg may provide. The Duck egg yolks are really orange. I did do a search for Duck Eggs but no information, brilliant resource and information.
Thanks Lynne
Hi Lynne,
I have data on duck breast and fat but not eggs. I think the more grass they eat, the more K2 they will naturally have in their eggs.
Chris
I’ve been told that chickens that consume marigold petals in their feed will produce eggs with darker orange yolks. Would marigolds help with vitamin K levels?
Thank you Chris. I have been a big fan of yours prcisely for your indepth coverage of a subject and your out of the box thinking. I have been a personal traditional foods chef for many years. Not due to my diet but inabilitty to handle stress which led to malignant hypertention and as a consequence kidney failure, I sm on dislysis. It isn’t just food that supports health! My research tells me that K2 and methaquloine can keep calcium out of my arteries and heart which is a consequence of the dislysis process. I needed help picking the best supplement. Your analysis made this possible. Allopathicmedicine and RD’s are no help in this regard. You are amazing.
Thanks Georgia! I’m glad my supplement review could help!
Hello
The poster who mentioned anxiety, insomnia, and a thumping heart from MK-7 may be interested to know our entire family (2ad, 4ch) have these horrid side effects when supplemental MK-4 is used. No matter the dose. We all have a soy allergy so have never tried the supps or foods derived from soy for MK-7. Thank you Chris for mentioning the Nested Naturals K2. This may be an option for us!
Brilliant article with wonderful infographics. Great!
Thanks for sharing your story Anna. Thanks also for the positive feedback on the article and graphics!
Hello Anna, I recently read of one other person who had an MK7 typical reaction to taking an MK4 only labeled vitamin K2 supplement by a reliable national manufacturer. While I have no immediate explanation, when they stopped taking it, it took three days for the symptoms to go away. This kind of time period would be more typical of MK7 than of MK4 so I wonder if the cause is contamination with MK7. In rare cases people do have unusual reactions to supplements content other than the vitamin.
Its propably caused by hypocalcemia.
There have been studies showing that Vitamin K2 can cause hypocalcemia.
A comprehensive resource.
I’m surprised you didn’t mention Koncentrared K in your review. Available from https://www.k-vitamins.com/ it contains 5mg of K1, 25mg of MK-4, .5mg of MK-7 and 2mg Astaxanthin per tablet.
Probably more than a healthy person needs, but for those worried about atherosclerosis or osteoporosis, it can’t be beat.
Hi Andrew,
My review focused on supplements that are easy to get close to 200 ug from so I limited to around 1 mg per lowest dose or less. However, due to the demand for coverage of other supplements, I’ll be adding them to the review in the next update.
Chris
Andrew, I just sent a similar note to Chris regarding this intriguing product as I’m considering getting it but I’m hesitant until I find out more about its quality. Are you using it?
Brilliant, brilliant!!! Thanks for user-friendly, thorough research. I have always been so curious: why is Edam the preferred source, and not Gouda, for example?
I would appreciate an explanation.
thanks
Johanita
Hi Johanita,
I’m not sure what you mean by preferred. I used edam in the infographic just as an example. There are a ton of cheeses in the database, and their contents vary. I think any of them are great if you tolerate them and eat the right amount.
Chris
I’m confused too. I pulled up dairy and saw no references for eithe rBrie or gouda cheese. Am I missing something?
Hi Sonia,
We collected everything we could find in the peer reviewed literature and didn’t come up with values for gouda and brie. There are two possibilities: 1) we missed something or 2) numbers floating around the internet for these cheeses are being generalized from descriptions like “soft,” “hard,” “Edam type” and so on.
It would be great if you could point me to a source in the literature or with original documentation on brie and gouda if you believe they are missing from this database.
Thanks,
Chris
Great graphics aid the readability and understanding for a broader audience. Thank you.
I make my own sauerkraut here in Belgium from local organic cabbages. Sometimes I eat it raw but generally, cooked (with boiled meat in the Alsace style). Any thoughts on K2 content?
Thanks Sammy. I think it would likely be similar to the sauerkraut in the database. Fairly low.
Chris
Thanks Chris for your usual high standards of research.
I tried to use your catalog of foods. The only problem is that
after one search is finished, on cannot go back and search for another food.
The program always takes you back to the very beginning of the
article. Perhaps this can be corrected in future editions.
Hi Ian,
This week I’ll try to fix that. I believe the simplest thing would be to have it open in a new page.
Another option would be to have the search results displayed on the same page without going to a new one.
Any thoughts on either choice?
I will add one other thing, which is that it takes 5 seconds to load. I find that obnoxious, and I am transferring my whole web site to a virtual private server though that will take a few days.
Chris
I will put my two cents in…always prefer opening a new page. 🙂
Celeste and Ian,
It now opens in a new page. Also, I’m on a new server and it loads a lot faster now.
Chris
I am taking 180 mcg of Jarrow bioactive MK-7 from natto and hoping this will help. Proper distribution of calcium has been a problem for me in the past. A few years age, I had to have a tooth pulled because my body was cannibalizing it. I have had lots of kidney stones. I had a heart attack about 15 years ago. I do eat quite a bit of raw milk aged cheddar, pastured eggs and chicken thighs.
I appreciate the info about light sensitivity. I have been keeping my meds and supplements in day-of-the-week boxes. Given the number of things I take, that is the only practical way. I guess I have wasted a lot of money on K2 and some other things that got degraded. Since reading this article, I have started keeping the K2 in the fridge with my fish oil. I suppose I should put the D3 there too.
Hi Harry,
I always err on the side of protecting anything from light. Really can’t hurt anything to do so.
Chris
Hi Chris!
I was wondering about the same thing, on how to store vitamin supplements, especially fat soluble ones.
During Summer, the temperatures inside my house can fluctuate between 25-30 ºC. I usually store them inside my kitchen, in the cupboard: it’s dry and it is not exposed to light, but it’s definitely not cold.
Is it really safe to store them in the refrigerator? It seems many people store them there, however I’ve also read that they can get condensation in the bottle and the moisture will simply spoil the supplements.
What do you think is the best way to store supplements besides avoiding light exposure?
Thank you for this awesome resource about vitamin K! It will hold a place alongside my most revered evidence-based textbooks.
You’re welcome Christine, thanks for your reverence! 🙂
Chris
I love everything you write. I am particularly interested in atherosclerosis casused by high lp(a). I know nutrition is involved in this process, and I would like to know your recommendations to halt or reverse this process.
Hi Susan,
I don’t believe high Lp(a) causes atherosclerosis, but, that’s another topic I’ll try to get to elsewhere. I do have a Facebook Live recording that covered it so you might want to search the site for Lp(a).
Chris
Chris,
Great post! Questions:
Several publications discuss: ‘Effects of Nattokinase on Blood Pressure”
https://www.researchgate.net/profile/Yangsoo_Jang/publication/23439158_Effects_of_Nattokinase_on_Blood_Pressure_A_Randomized_Controlled_Trial/links/00b4953cd9439b63b5000000.pdf?origin=publication_detail
Of course Natto is very high in MK7 and it is also high in Nattokinase which contains ACE inhibitors. Although, this is good for lowering blood pressure, it requires medical supervision and is not recommended with other blood pressure medications especially ARBs. Do you think there should be a warning in your newsletter about these kinds of interactions along the lines that you provide warnings for Coumadin etc?
Hi Bill,
You make a good point, but ultimately this resource is about vitamin K2, not natto. How much natto do you have to eat to interfere with the medication? If it’s less than 20 grams a day I should consider adding something about it.
Chris
This is an incredibly generous post and so thorough…but this is what I have come to expect from you. It will take me some time to digest it all but I will savor it. 😉 Thank you so much. I doubt I will have a single question when I am done. I suspect this is a small book. Would love for you to tackle one topic at a time in this manner. It would be an encyclopedia of great value. I know fat soluble vitamins are your area of expertise … perhaps A and D could be next. 🙂 Great Work! 🙂
Thanks Celeste!
I’m hoping the organization will help with savoring. I feel like it will be easier to keep track of the details you read if you read one detailed section at a time, and you feel like you finished it, than if this were a 30,000 word blog post and you stopped 10% of the way through and took a break.
Yes, I do feel like it would be a small book. Doing it with others is a great idea. There was so much learning that went into this, like days at a time going into each decision of what to use to make the infographics shareable and what to use to make the sections click-to-expand, trying things and ditching them, etc, etc, that now with a good model we could do future ones faster. But, got lots to do. So we’ll see what happens.
Chris
Just be sure you do not burn out…you are much too valuable a resource. 🙂
Celeste,
I will make sure. Thanks for looking out. 🙂
Chris
You seem to have missed the successful seven of thirteen trials of MK4 vitamin K2 done in Japan. These were very through in assisting bone loss patients and they had execellant results of about an 80% reduction in bone breakage rates. The research trials actually measured bone breakages in elderly adults. While expensive, this is the best metric available, most research BMD scans for vitamin K2 give weak results and the theory is that MK4 works on improving the connective tissue and microstructure in bone and this is not easily visible on a dexa a scan. There was even a published review saying that BMD testing was a bad measurement to use in vitamin K2 research and the fracture end point was preferred. In theJapan research trials, MK4 proved to be better at preventing bone breakages than most bone loss drugs!
Much of the science information used to promote the MK7 form of K2 can be seen to trace back to actual MK4 research when you look up the test sources and see the actual health outcomes. I find this objectionable with Dr Mercolas web site where MK7 is supported by quoting MK4 based research. There are educated people who quote MK4 research in favor of MK7 because some reports call it all vitamin K2 or they miss the biological differences.
Any measurement claiming “stays in the blood longer” is NOT a health metric, we are looking for measured health improvements and not blood levels. Indeed, high blood levels may indicate immobility in the body. You have not mentioned that about one in three people are sensitive to MK 7 which gives them anxiety, sleeplessness, and a thumping heart beat. These people have to use the MK4 form. This is a common comment in postings about MK7 in web discussions.
The last gasp of logic is that the Japan experimenters knew about MK7 which is well known in their culture as natto but for scientific reasons they choose to use the MK4 form in their research. Our bodies have a long evolutionary development path in using MK4, but MK7 is native to bacteria, not humans. Appreciate that hazard.
Hope this helps!
Dave
Thanks Dave, but will be nice to have included all the links to the many things you mention, but not one link to web discussions, research etc, I hope next time will be more positive contribution for everyone.
I came across the same Japanese studies about MK-4 and bone density. There are several studies–here’s a link to just one: https://www.ncbi.nlm.nih.gov/pubmed/21944271
Chris–Maybe you’re not familiar Pure Encapsulations’ product: Synergy K. That’s the one I take and recommend for patients. It’s made a big difference for some patients with Raynaud’s. (I don’t have Raynaud’s, but personally I found that 2 capsules 2x/day was an overdose, so I stick to 1-2x/day and that’s what I recommend.)
https://www.pureencapsulations.com/synergy-k-improved.html
vitamin D3 1,000 iu
vitamin K 1,545 mcg.
from:
vitamin K1 500 mcg.
vitamin K2 (menaquinone-4) 1,000 mcg.
vitamin K2 (menaquinone-7) 45 mcg.
What were your overdose symptoms? I found taking 5 mg. Gave me severe bloodshot eyes.
Hi Jeanette,
I was looking specifically for supplements around 1 mg or lower to make it easy to take on average 200 ug and made the cut off Life Extension’s which gives 1.2 mg K2. However, there seems to be demand for reviewing a few higher-dose products, so in the first revision, probably later this week, I’ll include a few higher-dose supplements like this one.
Chris
Cynthia–While I generally felt my extremities were warmer taking the Synergy K, after 1-2 weeks at 4 capsules per day (~4 g) it started getting interesting: Periodically I would get fleeting ice-cold sensations in my nose, toes, and fingertips, only a few seconds or so–then I’d revert to normal. I allowed it to last about a week or so until the frequency started happening daily or multiple times per day. Cutting down to 2 capsules/day (~2 g) gives me no symptoms of the sort.
Chris–thank you! I appreciate your work and look forward to your updates.
Best,
Jeannette
Jeanette,
Interesting. I wonder if that could have been due to MK-4 inhibition of bone resorption and loss of the metabolic rate-stimulating effects of osteocalcin.
Chris
Hi Dave,
I didn’t miss those trials at all, and they are discussed in several of the click-to-expand detailed sections.
I’d appreciate a reference for your statement that one in three people get anxiety or similar problems from MK-7 supplements.
I agree the half-life argument is bogus.
However, the utilization of MK-4 at 45 mg/d is a pharmacological use and not a nutritional one. This resource is primarily about vitamin K as a nutrient.
Chris
I was just going to post a comment that the metabolic half life of mk4 is hours while same for mk7 is days. Many papers are coming out now saying there is a dose dependent improvement in agglomeration of alpha synuclein (putative cause of Parkinson’s ) by mk4 ranging from 1 to 20 micromolar concentration. Moreover mk4 goes more successfully to the brain. So the 45mg dosed over 24 hrs makes sense to me for those focused on neuron health.
David, thank you for bringing up the fact that bone mineral density is only one feature of healthy, resilient, bone. I’m hoping I also have a healthy collagen matrix for the minerals to deposit onto.
You can certainly tell how much work you put into this! Thank you so much. This is very comprehensive and understandable about a very important subject. Thank you again!!!
Thanks Laura! Yes it was a ton of work. Glad it shows. 🙂
Chris
Best post I have seen ever!
Thanks Neil!
Genial, thanks Chris for the excellent post, do you like any critics? from a healthy oldie born in the 1940’s, please for the links to other research etc instead of light green please use the default dark blue or similar darker color to help our vision, the same can be said for some of the graphics with white or very similar color font. Thank you.
Hi Camilo,
The white in the infographics was brought up by someone else and I’ll see if we can improve the contrast this week.
For the color of the links, I’m going to have to put that off until the next time I modify my theme. It could be a while. But I appreciate you pointing it out and I’ll take it into consideration at the proper time.
Chris
Hi Chris,
I immediate feeling is one of gratitude and appreciation for everything you do and for this great resource that you’ve provided. I read all your stuff or most of it, time permitting. I do some teaching presentations for Standard Process West and always enrich those presentation with the fantastic info and research that you share. You are incredibly generous and make our world a better place with your thirst for knowledge and understanding of health and nutrition. Thank you!
Thanks Larry! I appreciate your feedback and your own appreciation.
Hi Chris, great article. Thank you! What about the MK-4 in emu oil? Isn’t that the best source of natural MK-4? Thanks.
Hi Gina,
As a food oil, emu is a great source of MK-4. The amount per capsule is low, so I’m not including it in the supplement review, but this coming week I will have it added to the database as a food. (About 4 tablespoons are necessary to get 200 ug K2.)
Chris
Hi Gina,
Emu oil is now in the database.
Chris
416.5mcg per 100ml –> ~4mcg per capsule, and about 60mcg per tablespoon. So yes, you need more than 3 tablespoons of this stuff to meet your 200mcg requirement. The capsules seem useless as you would have to take almost 50 of them every day.
Zoltan,
That doesn’t make them “useless.” Five capsules would give you 20 ug, and that could be a doubling of K2 intake for someone with a very low intake of 20 ug, which would make a big difference. The benefit becomes exponentially greater the lower your baseline intake.
For someone who gets 180 ug per day from foods, the extra 20 ug would be comparatively meaningless.
But the emu oil has other things besides MK-4, so even in the context of someone with a K2-rich diet it could be beneficial for its other properties.
Chris
Chris,
Good point about 20mcg making a big difference for folks with a very low intake.
On a related note I see the data in the database is specifically for Walkabout Australian emu oil – would you expect a significant deviation from these figures for emus raised elsewhere, e.g. in Europe?
Zoltan,
I don’t know about other emus. Walkabout has some experimental data showing their emu oil has greater effectiveness against arthritis in animal models than a different genotype of emus. But I don’t think anyone’s tested the variety of emu oils for K2. So, I’d consider it an unknown.
Chris
Thanks so much Chris!
As always Chris, thanks for your diligence, detail and easy to understand summary that also inlides wonderful info on how to access and use K2. Brilliant!
Thanks Rosemary!
Thank you for this wonderfully in depth information on K-2. It came just at the moment I was googling K-2 info. You have a way of making the involved research easy to understand and with a protocol that makes one know how to proceed. I have just begun taking emu oil from Walkabout along with my pasture raised soy free raw milk butter & I have noticed an improvement in the inflammation in my old body.
Thanks TikiBlu! I’m glad it was helpful and came at the right time, and that your health is improving.
Chris
Fully comprehensive and takes out the confusion. Thanks so much for the info.
You’re welcome Mirian!
Wonderful combination of visuals and text. Thank you for this invaluable resource
Thanks Rob A! You’re welcome.
Outstanding – thank you!!!
You’re welcome Susan!
Wonderful post, thank you!
Thanks Country Farmer!
So happy to find this just at a time I’ve been scared half to death with a new diagnosis of osteoporosis and the high-powered drugs prescribed typically. I need to know what is a therapeutic combination of K types and amount for helping osteo folks!
Glad you made it here!
How often should I eat a 4oz piece of calf liver to have adequate Vitamin K levels?
Healthy Female, age 45
Hi Kyria,
You can look up calf liver in the database to see how much it would take to get 1-200 ug.
Chris
HI TRIED TO FIND CALVES LIVER FOR I TOO WANT TO KNOW HOW MUCH YOU HAVE TO EAT rEAD THAT YOU SHOULDNT EAT IT EVERY DAY HIGH IN VITAMIN A.BUT AS A CHILD WE ATE IT ALL THE TIME.
Vitamin A toxicity is often overstated and mostly (if not entirely) resulted from synthetic pills not real food. I often eat 1–1.5 pounds a week, not quite daily, with no detrimental effects. Also I’ve real that traditional diets are estimated to contain huge amounts of A. Something like 10,000 iu, though I could have the number or unit wrong.
Still, if you can, might be good to find multiple sources so as not to depend on one food alone. I’m really appreciating both the food list and the cheat sheet where Chris has done the comparison shopping I was slogging through and got bogged down and never finished. Really appreciating both will help us get enough K2.
@Antonio: Agreed – pretty much all the cases of vitamin A toxicity I’ve read about comes from the person having taken vitamin A through synthetic supplements. Vitamin A through natural sources like food that naturally contains it (e.g. liver) will not cause toxicity, or will only do so if the person eats an insanely high amount.
I also eat liver on a regular basis–sometimes a lot of it in one sitting–and like Antonio I have never experienced negative effects.
I don’t buy that it’s because of “synthetic supplements.” I think it much more likely that people have problems with vitamin A supplementation because they are not also getting enough D3 and K2. As I understand it, these three vitamins all play nicely together and help prevent toxicity in any one of them.
For someone with an absolute aversion to liver, they need a solution besides “oh, just eat a lot of egg yolks and vegetables.” A lot of people have trouble converting beta carotene anyway. I’m probably one of them, going on my health history and how my body’s responded to A supplementation. I just make sure it’s a high-quality A supplement derived from cod liver oil and *not* utilizing polyunsaturated oils like corn oil and soybean oil, which can actually (I heard) destroy the vitamin, rendering the capsules well nigh useless.
And I always take A, D3, and K2 together!
I know of a poor fellow who got a severe case of toxicity from eating liver everyday. He knew better than to do that. Unfortunately, I do not know what happened to him. He was upset at people in the group that used to say that you cannot get toxicity from food.
Very comprehensive and useful review, thank you.
Your food database basically provides a ranking by total K2 content, from highest content to least.
It would be very useful if it could also provide a ranking by MK4 content. It seems easier to get enough MK7 from food, given that you mentioned that MK9 behaves similarly to MK7, and natto, fermented soybeans, and Jarlsberg cheese would be good sources of either MK7 or MK9.
Thank you.
Hi Madeleine,
Every single food you can click on “view more details” to find a full listing of all menaquinones.
I believe it would be an enhancement to be able to *rank* them by specific MKs, and I’ll look into that for the future. Initially, it provided difficult to do that and keep the interface user-friendly, so I’ll have to think more about the design and do some testing before introducing that functionality.
Chris
Very, very cool, Chris! Thanks for writing this up! The MK-4 vs MK-7 discussion is especially interesting; looking forward to hearing more about the longer chain variants in pork…
Thanks Jesse, and you’re welcome!